You can browse the changelog as-is, or use the filter tools to show only the changes between version numbers and / or date ranges by entering a value in one of the relevant "From" fields.
You can also filter by Type to eg. show only "Product" changes, which can be helpful for people already doing the protocol.
| wdt_ID | wdt_created_by | Date | wdt_last_edited_by | wdt_last_edited_at | Ver | Rev | Type | Change | Description |
|---|---|---|---|---|---|---|---|---|---|
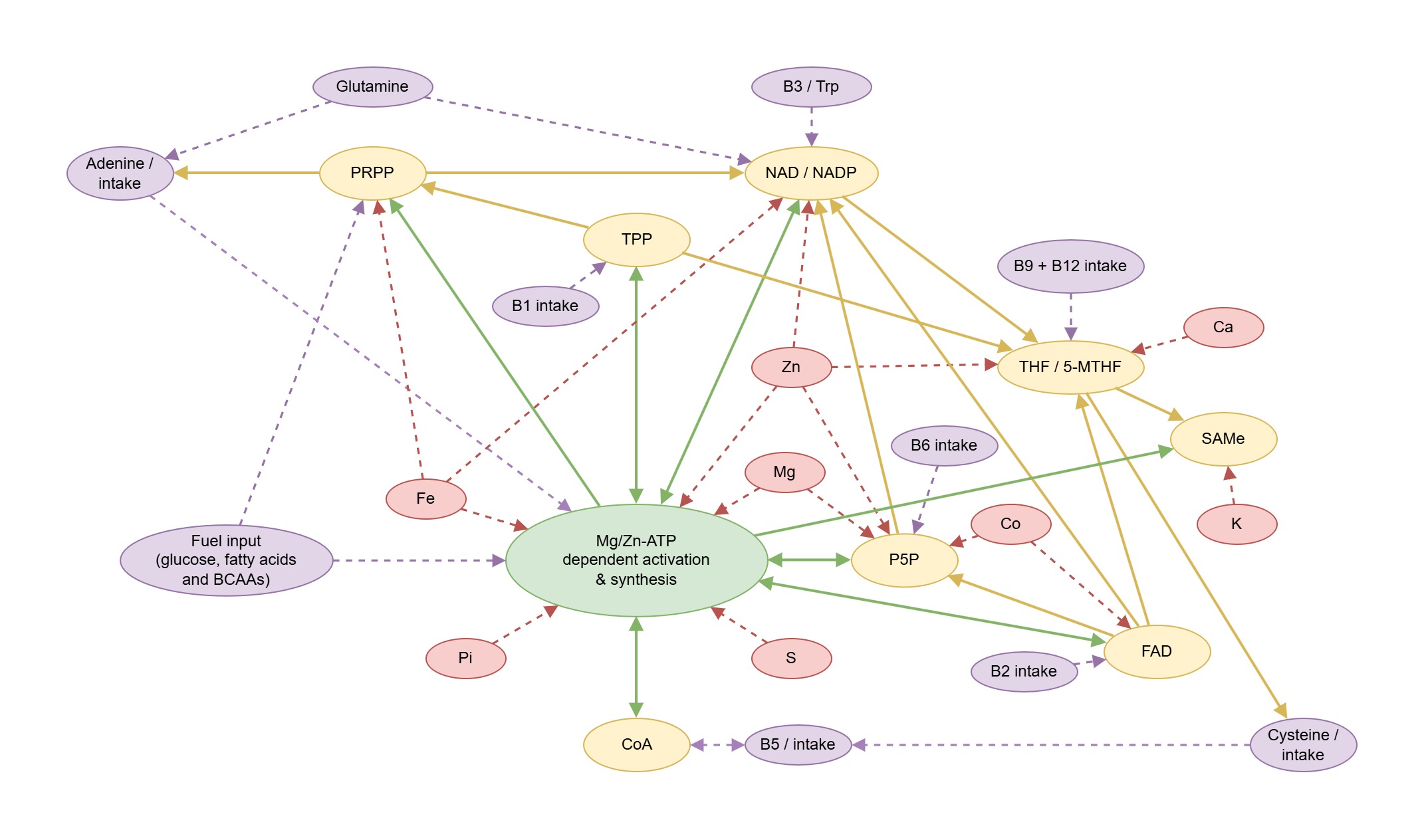
| 382 | 3dghs2 | 09/06/2026 | 3dghs2 | 09/06/2026 05:26 AM | 3.8 | Website | Update | Additional Figures added to Metabolic Pathway Tool and zoom function / rendering bug on Chrome, Edge corrected. | |
| 381 | 3dghs2 | 27/05/2026 | 3dghs2 | 27/05/2026 07:05 AM | 3.8 | Product | Addition | MiaDMSA and (optional) Pectasol added for selective toxic metals chelation / removal. | |
| 380 | 3dghs2 | 27/05/2026 | 3dghs2 | 27/05/2026 07:03 AM | 3.8 | Product | Update | Silica - bamboo replaced by Mesoporosil | |
| 379 | 3dghs2 | 02/05/2026 | 3dghs2 | 02/05/2026 11:52 AM | 3.8 | Website | Update | "OAT Wizard" - Universal OAT Interpreter replaces all existing individual OAT tools. Genova Diagnostics NutrEval and Metabolomix report added. Collect your data -> Organic Acids Tests section updated. | |
| 378 | 3dghs2 | 29/04/2026 | 3dghs2 | 29/04/2026 01:17 PM | 3.8 | Website | Update | OMX OAT Interpreter Tool added and connected to Metabolic Pathway Overlay Tool. | |
| 377 | 3dghs2 | 29/04/2026 | 3dghs2 | 29/04/2026 06:44 AM | 3.8 | Website | Update | Theriome and Metabolic Pathway tools updated to support new PDF layout and Z-score for Aristotle Plus. | |
| 376 | 3dghs2 | 26/04/2026 | 3dghs2 | 26/04/2026 10:22 AM | 3.8 | Website | Update | NutriPATH OAT Interpreter tool added and connected to Metabolic Pathway Overlay tool. | |
| 375 | 3dghs2 | 25/04/2026 | 3dghs2 | 25/04/2026 02:01 AM | 3.8 | Website | Update | Vibrant OAT Interpreter tool added and connected to Metabolic Pathway Overlay tool. Nordic v4 report compatibility added to MosaicDX OAT interpreter tool. | |
| 374 | 3dghs2 | 22/04/2026 | 3dghs2 | 22/04/2026 04:54 AM | 3.8 | Website | Update | Metabolic Pathway Overlay tool now features multiple diagrams, PDF export and better landscape support on mobile devices. | |
| 373 | 3dghs2 | 21/04/2026 | 3dghs2 | 21/04/2026 02:00 AM | 3.8 | Website | Update | MosaicDX OAT Tool now accepts v2 Nordic Labs rebranded PDFs. | |
| 372 | 3dghs2 | 20/04/2026 | 3dghs2 | 20/04/2026 02:25 PM | 3.8 | Website | Update | Metabolic Pathway Tool - significant performance enhancements and mobile UI bugfixes. "See also" feature added for highlighting up/downstream logic. | |
| 371 | 3dghs2 | 16/04/2026 | 3dghs2 | 16/04/2026 04:27 AM | 3.8 | Product | Replace | Monocalcium phosphate replaced with calcium aspartate. Magnesium aspartate replaced with magnesium phosphoglycerate. Benefits for onboarding simplicity and repletion efficiency. | |
| 370 | 3dghs2 | 15/04/2026 | 3dghs2 | 15/04/2026 09:34 AM | 3.8 | Product | Addition | Ashwagandha added to getting started section and all protocol stages to support thyroid function. | |
| 369 | 3dghs2 | 14/04/2026 | 3dghs2 | 14/04/2026 08:28 AM | 3.8 | Product | Update | Glycine dose increased from 5-15g. Serine dose increased from 2-4g. Both amino acids moved from the shake to the sipper. | |
| 368 | 3dghs2 | 12/04/2026 | 3dghs2 | 12/04/2026 01:32 PM | 3.8 | Website | Update | Major updates for Metabolic Pathway Overlay, MosaicDX OAT and Theriome Aristotle tools. Support for Aristotle Plus. Updated scoring system. Pattern interpretations added. | |
| 367 | 3dghs2 | 27/03/2026 | 3dghs2 | 27/03/2026 09:07 AM | 3.8 | Website | Update | Metabolic Pathway Tool now accepts original PDF files and pre-processes them through the related BF tools. Mosaic OAT tool now auto-corrects left shift, when present. | |
| 366 | 3dghs2 | 26/03/2026 | 3dghs2 | 26/03/2026 11:52 AM | 3.8 | Website | Update | Oligoscan Processor tool now supports multilingual reports for both So/Check and Oligoscan. Metabolic Pathway Overlay tool has a broad array of minor fixes and improvements. | |
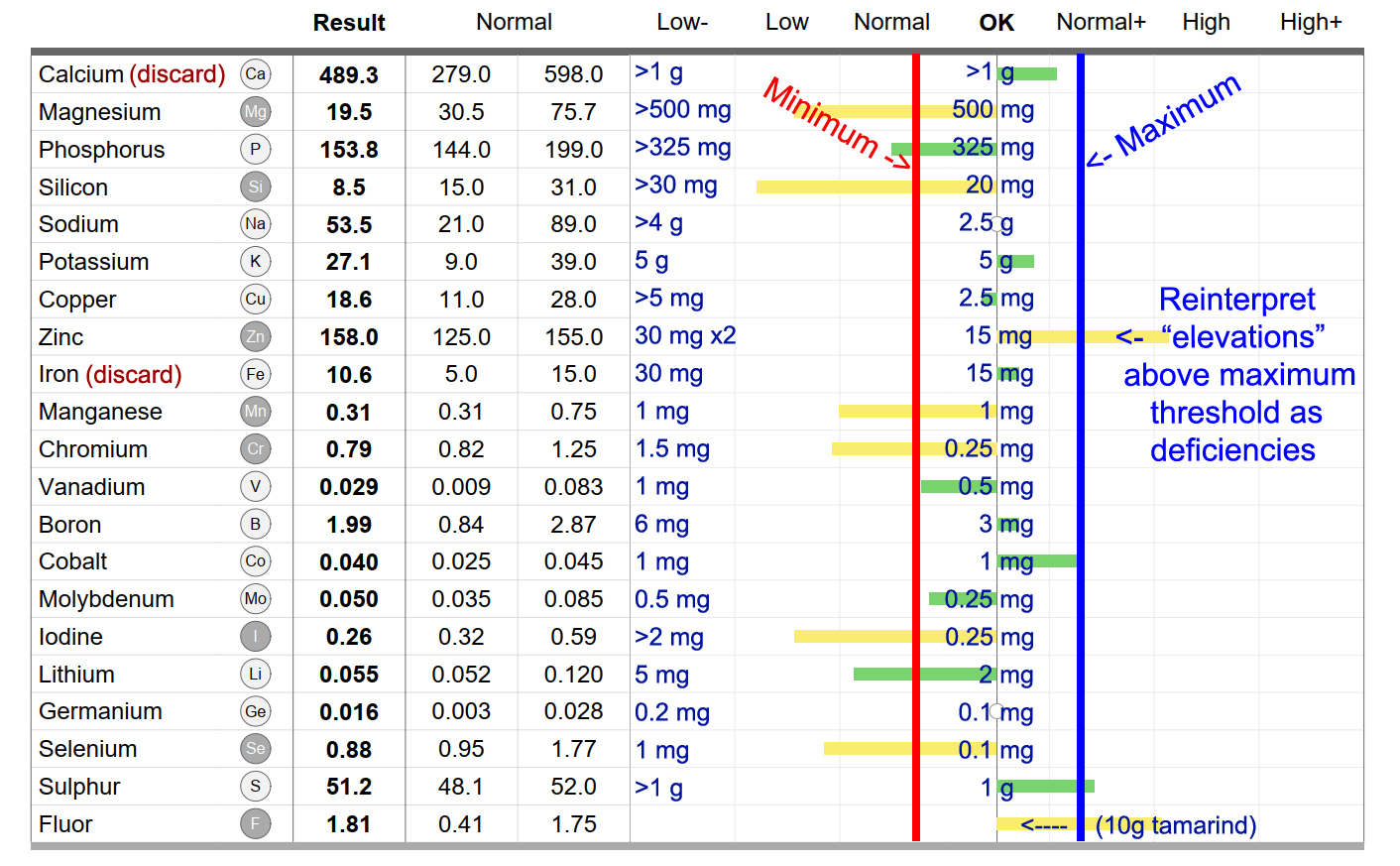
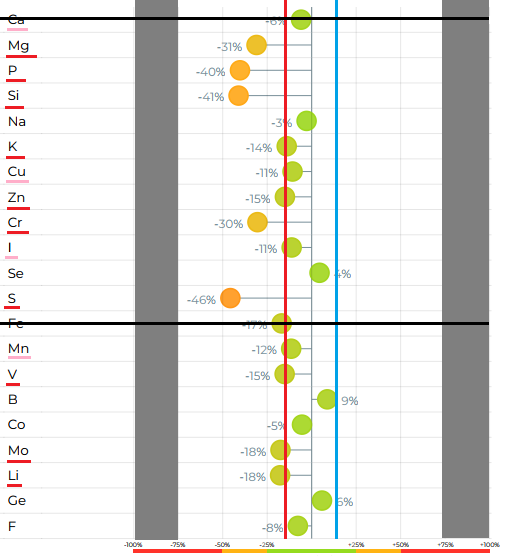
| 365 | 3dghs2 | 23/03/2026 | 3dghs2 | 23/03/2026 04:49 AM | 3.8 | Website | Update | Metabolic Pathway Overlay tool released. Currently supports Oligoscan, MosaicDX OAT and Theriome Aristotle report outputs from BF tools. | |
| 364 | 3dghs2 | 20/03/2026 | 3dghs2 | 20/03/2026 03:24 AM | 3.8 | Website | Update | Oligoscan Processor tool now supports SO/Check reports. Heavy metal values have been normalised between report types. Comparison report detects / adapts to any source. | |
| 363 | 3dghs2 | 19/03/2026 | 3dghs2 | 19/03/2026 12:02 PM | 3.8 | Website | Update | Find an Oligoscan Practitioner updated with over 130 additional locations. | |
| 362 | 3dghs2 | 01/03/2026 | 3dghs2 | 01/03/2026 11:54 PM | 3.8 | Website | Update | Oligoscan Processor tool now falls back to OCR attempts for scanned images. Option to anonymise outputs. Comparison report generation feature added. | |
| 361 | 3dghs2 | 28/02/2026 | 3dghs2 | 28/02/2026 11:29 PM | 3.8 | Website | Update | Electrolytes Calculator tool updated with a broad range of compounds and automatic pre-fill function. | |
| 360 | 3dghs2 | 23/02/2026 | 3dghs2 | 23/02/2026 08:48 AM | 3.8 | Text | Update | The importance of pacing section updated for clarity. | |
| 359 | 3dghs2 | 18/02/2026 | 3dghs2 | 23/02/2026 08:53 AM | 3.8 | Website | Update | Corrected / updated mobile UI menu CSS for very low width resolution and added hovering mobile menu. Oligoscan processor and Meal Planner updated. | |
| 358 | 3dghs2 | 11/02/2026 | 3dghs2 | 18/02/2026 03:32 AM | 3.8 | Website | Update | Dark/light theme switcher added, with OS sensing. Electrolytes calculation tool added. | |
| 357 | 3dghs2 | 07/02/2026 | 3dghs2 | 07/02/2026 11:28 PM | 3.8 | Website | Update | User interface updated for enhanced readability and navigation. | |
| 356 | 3dghs2 | 02/02/2026 | 3dghs2 | 02/02/2026 08:08 AM | 3.7 | Text | Update | Mosaic OAT and Theriome Aristotle tools both updated - sporting new bar graph displays, updated PDF export functions and minor dictionary updates. | |
| 355 | 3dghs2 | 28/01/2026 | 3dghs2 | 28/01/2026 07:13 AM | 3.7 | Text | Update | Added "Meal Planner" tool. Added compounds to electrolytes section. Corrected text and dosing for biotin (alternate). | |
| 354 | 3dghs2 | 17/01/2026 | 3dghs2 | 17/01/2026 04:07 AM | 3.7 | Text | Update | Overhauled "2 The protocol" and related "Getting started" sections, for easier onboarding and clarity. The "Getting started" section content can now also be found on a stand-alone page (also in the website navigation menu), to reduce information overload. | |
| 353 | 3dghs2 | 15/01/2026 | 3dghs2 | 15/01/2026 06:37 AM | 3.7 | Text | Update | Added "daily" DIY sipper/shot recipe to the getting started daily run-sheet subsections, for simpler onboarding. Added reflux / vitamin U content to 2.2.3 Living without chronic dysbiosis. | |
| 352 | 3dghs2 | 14/01/2026 | 3dghs2 | 14/01/2026 05:09 AM | 3.7 | Text | Update | Integrated starting order (onboarding) groups into the daily run-sheets / schedules. | |
| 351 | 3dghs2 | 12/01/2026 | 3dghs2 | 12/01/2026 01:44 AM | 3.7 | Product | Addition | Resveratrol added back into the protocol for protection against excess lactic acid during onboarding electrolyte repletion and during metabolic stress. | |
| 350 | 3dghs2 | 09/01/2026 | 3dghs2 | 09/01/2026 04:14 AM | 3.7 | Product | Removed | Hesperidin removed from DIY shake recipe and main protocol pathway (replaced by MB microdosing). Can be used for specific hypometabolic events. | |
| 349 | 3dghs2 | 07/01/2026 | 3dghs2 | 07/01/2026 10:10 PM | 3.7 | Text | Update | Minor clarity updates. Corrected daily supplement schedule error - was missing Methylene Blue. | |
| 348 | 3dghs2 | 07/01/2026 | 3dghs2 | 07/01/2026 10:09 PM | 3.7 | Product | Source | Cobalt sources for US, EU, AU updated. | |
| 347 | 3dghs2 | 06/01/2026 | 3dghs2 | 06/01/2026 04:42 AM | 3.7 | Text | Update | Added content for fungi and metabolic acidosis to Gastrointestinal biofilms and pathogens subsection of 2.2.3 Living without chronic dysbiosis. | |
| 346 | 3dghs2 | 30/12/2025 | 3dghs2 | 30/12/2025 07:12 AM | 3.7 | Text | Update | Getting started section updated with downloadable daily schedules. Sympathetic overdrive section updated for clarity around influence of impaired nasal breathing + infection / inflammation. | |
| 345 | 3dghs2 | 22/12/2025 | 3dghs2 | 22/12/2025 12:20 PM | 3.7 | Text | Update | Updated the beginning of paragraph 2 in 2.2.4 The importance of “pacing” or “just enough activity” for clarity, as it was being misinterpreted widely that PEM was fear. Apologies for any confusion. | |
| 344 | 3dghs2 | 19/12/2025 | 3dghs2 | 19/12/2025 06:05 AM | 3.7 | Product | Addition | Inosine added to pre-protocol support and all stages. | |
| 343 | 3dghs2 | 18/12/2025 | 3dghs2 | 18/12/2025 12:32 PM | 3.7 | Tool | Update | Mosaic OAT Interpreter now works with the new v3 2025 report layouts. | |
| 342 | 3dghs2 | 29/11/2025 | 3dghs2 | 29/11/2025 02:19 AM | 3.7 | Text | Update | Uridine, Mg, P and carbohydrates added to rapid withdrawal support. 60-70% ethanol mentioned in DIY antiseptic subsection of 2.2.3 Living without chronic dysbiosis | |
| 341 | 3dghs2 | 28/11/2025 | 3dghs2 | 28/11/2025 03:01 AM | 3.7 | Text | Update | Your nervous system sends "predictions", not "facts" subsection added to 2.2.6 Cortisol, limbic system, glycogen and IFN-γ | |
| 340 | 3dghs2 | 24/11/2025 | 3dghs2 | 24/11/2025 04:58 AM | 3.7 | Text | Update | An easier onboarding process for ordering products, etc. can now be found in the Getting started subsection of "2 The protocol". | |
| 338 | 3dghs2 | 18/11/2025 | 3dghs2 | 18/11/2025 03:17 AM | 3.7 | Product | Addition | Uridine monophosphate added to sublingual dosing schedule, pre-protocol support. | |
| 339 | 3dghs2 | 18/11/2025 | 3dghs2 | 18/11/2025 03:17 AM | 3.7 | Product | Addition | D-ribose added to DIY sipper recipe and pre-protocol support. | |
| 337 | 3dghs2 | 17/11/2025 | 3dghs2 | 17/11/2025 03:09 AM | 3.7 | Text | Update | Updated DIY sipper, pre-protocol support and electrolytes sections to match monocalcium phosphate product upgrade. | |
| 336 | 3dghs2 | 17/11/2025 | 3dghs2 | 17/11/2025 03:08 AM | 3.7 | Product | Replace | Dicalcium phosphate upgraded to monocalcium phosphate for improved solubility and flavour, plus increased phosphate intake. | |
| 335 | 3dghs2 | 14/11/2025 | 3dghs2 | 14/11/2025 10:27 PM | 3.7 | Text | Update | Minor updates for clarity in pre-protocol and elecetrolytes section. | |
| 334 | 3dghs | 12/11/2025 | 3dghs | 12/11/2025 02:39 AM | 3.7 | Text | Update | Table of parasympathetic influences added to 2.2.6 Cortisol, limbic system, glycogen and IFN-γ, Sympathetic overdrive subsection. | |
| 333 | 3dghs | 10/11/2025 | 3dghs | 10/11/2025 07:11 AM | 3.7 | Text | Update | 2.2.6 Cortisol, limbic system, glycogen and IFN-γ updated, eATP P2X7 cascade added. | |
| Date | Ver | Type |