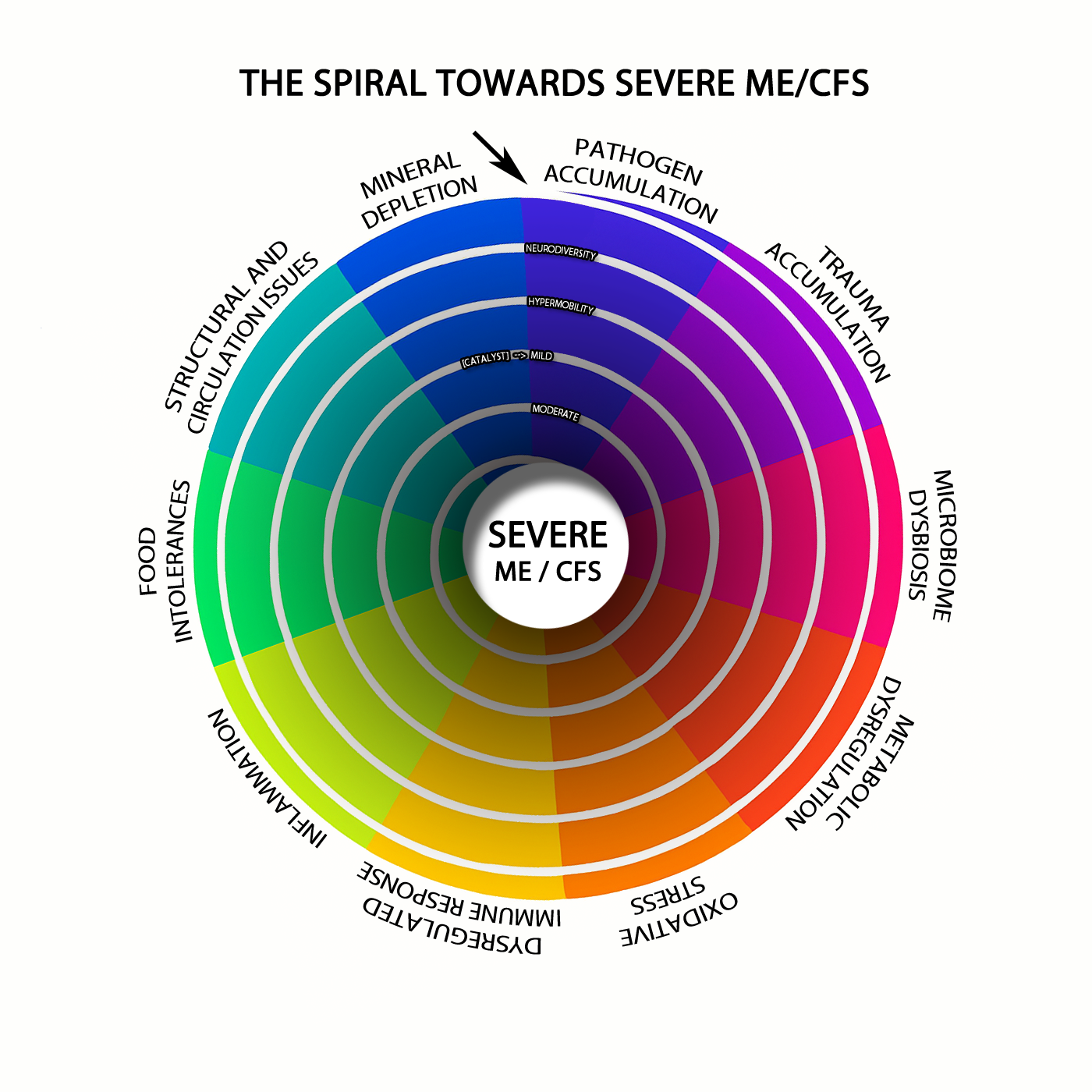
This model aims to explain how a long-term illness could develop when the body slowly loses control over energy production, mineral balance, immune signalling, stress hormones, gut microbes and inflammation. It does not assume there is one single cause. Instead, it describes a situation where many small problems build up over time, then eventually lock together into a self-reinforcing cycle.
The main idea is that the body may become trapped in a “survival mode” that is useful for short-term danger, but damaging if it continues for months or years.
In a healthy body, cells constantly manage several linked systems. They make energy from food, store glucose as glycogen, recycle antioxidants, move minerals into the right places, remove toxic metals and chemical waste, calm inflammation after danger has passed, and switch between stress mode and recovery mode. This model proposes that chronic disease can appear when those systems stop coordinating properly.
One possible starting point is before birth. A baby may inherit some risk from the mother’s biology during pregnancy, including metal exposure, mineral status, immune activation, inflammation, stress hormones or altered glucose handling. In this model, gestational diabetes is not viewed only as “too much sugar”. It may also reflect a problem with how glucose is stored and processed. If the body does not have enough magnesium, phosphate, zinc, selenium, folate, choline or other helper nutrients, it may struggle to turn glucose into glycogen, antioxidants and repair materials. So high blood sugar during pregnancy may sometimes be a sign that the glucose-management system is already under strain.
After birth, the model suggests a slow decline rather than one sudden break. Stress, poor sleep, infections, trauma, insufficient carbohydrate intake, low mineral intake, connective tissue problems, neurodivergent stress load, gut problems or toxin exposure may gradually reduce the body’s ability to adapt. For a long time, the person may still function, but they are functioning with less spare capacity.
A central part of this model is redox balance. Redox is the cell’s system for moving electrons during energy production and antioxidant defence. Two important redox systems are NAD⁺/NADH and NADP⁺/NADPH. These are like rechargeable chemical carriers. NAD⁺ helps cells process fuel and keep mitochondria working. NADPH helps recycle antioxidants such as glutathione. Glutathione is one of the body’s main systems for controlling oxidative stress and handling toxic metals.
If NAD⁺, NADPH and glutathione become weak, several things can happen at once. Energy production becomes less stable. The body becomes worse at clearing chemical waste. Toxic metals may be harder to remove. Essential minerals may be lost or moved into the wrong places. Inflammation becomes harder to switch off. Cells may begin to act as if they are under constant threat.
This is where the model becomes more serious. A major immune event may push the system past a threshold. This could be an infection, immune flare, surgery, pregnancy, overexertion, heat stress, toxin exposure, severe sleep loss, emotional trauma or another strong biological stressor. The immune system may release inflammatory signals such as TNF-alpha, IL-1beta, IL-6, IL-10 and IL-22. These signals can increase hepcidin, a hormone that controls iron movement.
Hepcidin is important because it changes how the body moves metals. It can reduce iron export from cells and alter mineral transport through systems such as ferroportin and DMT1. In simple terms, inflammation can cause metals and minerals to be moved out of the blood and into organs such as the liver, spleen, kidneys, immune cells and possibly the brain. This means blood tests may show low minerals, while tissues may still be overloaded or misallocated. The issue is not just deficiency or toxicity. It is poor distribution.
Once this redistribution happens, the body may struggle to maintain basic energy chemistry. Glycogen storage may fall. Glycolysis, the first stage of glucose breakdown, may become unstable. The mitochondria may struggle to process fuel through the TCA cycle and electron transport chain. NAD⁺ may become harder to regenerate. NADPH may become less available for antioxidant defence. ATP, the cell’s main energy molecule, may become harder to use properly.
At the same time, ATP can become a danger signal outside cells. Inside cells, ATP is useful energy. Outside cells, ATP often tells the immune system that tissue is stressed or damaged. This is called extracellular ATP signalling. Normally, extracellular ATP is quickly broken down into ADP, AMP, adenosine and inosine, which can help calm inflammation and support recovery. But in this model, that calming sequence may become impaired.
The result is a split: cells may have too little usable energy inside, while too much danger signalling happens outside. Extracellular ATP can activate receptors on mast cells, immune cells, nerves, blood vessels, gut lining cells, skin cells and brain support cells. This can increase inflammation, pain signalling, mast-cell activation, oxidative stress, cytokine release and “cell danger” signalling. Instead of resolving the problem, the signal keeps repeating.
The gut microbiome may then adapt to this stressed environment. If the body is stuck in sympathetic overdrive, with low oxygen in tissues, poor gut movement, low bile flow, weak immunity and unstable glucose storage, some microbes may shift toward fermentation. This may increase ethanol, acetaldehyde, D-lactate, hydrogen sulphide, ammonia and other microbial products. These may be useful in small amounts or short bursts, but harmful if produced chronically.
Acetaldehyde is especially important in this model. It is a reactive chemical produced from alcohol metabolism and by some microbes. The body normally clears it using aldehyde dehydrogenase enzymes, often shortened to ALDH. These enzymes require good NAD⁺ redox. If NAD⁺ is low or poorly recycled, acetaldehyde clearance may fall. But acetaldehyde itself can further damage redox balance. This creates a loop: poor NAD⁺ makes acetaldehyde harder to clear, and acetaldehyde makes NAD⁺ problems worse.
Acetaldehyde may also interfere with nutrient function. It may reduce zinc availability, disturb magnesium-dependent enzymes, form adducts with thiamine, impair active vitamin B6 handling, affect riboflavin conversion into FMN and FAD, disturb folate and B12 metabolism, lower SAMe, affect retinoic acid signalling, impair CoQ10 production and worsen BH4 oxidation. This could create a “functional deficiency” state. The nutrient may be present in the diet or even appear normal in blood, but may not work properly inside cells.
This connects to histamine. Histamine is not only involved in allergies. It also affects blood vessels, the gut, the brain, immune cells and energy metabolism. In this model, histamine may rise for two reasons: mast cells release more of it, and the body clears it more poorly. Gut barrier damage, antigen exposure, extracellular ATP, oxidative stress and inflammation may trigger mast cells. At the same time, acetaldehyde, low zinc and impaired ALDH or DAO activity may reduce histamine breakdown.
High histamine can then worsen the energy problem. In the liver, histamine signalling may promote glycogen breakdown, reducing stored glucose. This can contribute to blood sugar instability, adrenaline surges, POTS-like symptoms and post-exertional malaise. Histamine may also increase sensitivity to beta-adrenergic signalling, meaning the body reacts more strongly to stress hormones such as adrenaline. Exercise, which normally helps adaptation, may then trigger an exaggerated histamine and inflammatory response.
Another important loop involves nitric oxide and BH4. BH4 helps enzymes make nitric oxide properly. Nitric oxide helps blood vessels relax and supports healthy circulation. If oxidative stress damages BH4, nitric oxide production may become uncoupled, meaning the system produces more superoxide instead. Nitric oxide and superoxide can combine to form peroxynitrite, a damaging reactive molecule. Peroxynitrite may inhibit mitochondrial complex I, making NAD⁺/NADH redox worse. This links oxidative stress, poor blood flow, mitochondrial inhibition and acetaldehyde clearance into one cycle.
As these loops build, the nervous system may shift into sympathetic dominance. The sympathetic nervous system is the “fight or flight” side of the autonomic nervous system. At first, this is protective. It raises alertness, mobilises glucose, supports blood pressure and keeps the person functioning. But if the body cannot restore glycogen, clear glutamate, regenerate NAD⁺, calm extracellular ATP signalling or return to parasympathetic recovery, the stress response becomes maladaptive.
This may create a situation where the body keeps trying to mobilise energy, but cannot store or use that energy properly. Adrenaline, cAMP-PKA signalling, calcium stress, glutamate release, histamine, extracellular ATP and inflammatory cytokines may all amplify each other. The person is biologically pushed to “keep going”, while the recovery systems needed to repair the damage are underpowered.
Connective tissue may also be part of the model, not just a side issue. Collagen production depends on oxygen, iron, vitamin C, copper, silica, glycine, proline, lysine, ATP, redox balance and enzymes such as prolyl hydroxylases. If the body has acidaemia, lactate buildup, hypoxia signalling, oxidative stress, low minerals, poor NADPH repair and chronic inflammation, collagen maintenance may suffer. This could contribute to hEDS-like or vEDS-like features, gut barrier weakness, unstable blood vessels, poor lymph flow, pain, joint instability and higher sensitivity to mechanical stress. Mechanical stress can then release more extracellular ATP and activate mast cells, feeding back into the same cycle.
Over time, the immune system may become both overactive and ineffective. It may produce inflammation, but fail to clear pathogens properly. Poor sleep, low ATP, mineral misallocation, cortisol dysregulation, weak interferon responses and poor nutrient activation may allow viral, bacterial, fungal or other reservoirs to persist. These reservoirs can then keep triggering cytokines, hepcidin, mast cells, extracellular ATP and oxidative stress.
This is why the “what came first?” question becomes less useful in established disease. Early on, the main trigger might have been infection, toxic metals, poor mineral status, pregnancy, trauma, connective tissue fragility, gut dysbiosis, neurodevelopmental stress, histamine intolerance or immune activation. But later, all of these can become connected.
Acidaemia worsens mineral wasting. Mineral wasting worsens ATP chemistry. Poor ATP chemistry weakens glutathione. Low glutathione worsens metal retention. Metal retention worsens mitochondrial redox. Poor redox worsens acetaldehyde clearance. Acetaldehyde worsens histamine clearance. Histamine worsens glycogen instability. Low glycogen worsens adrenaline surges. Adrenaline increases extracellular ATP release. Extracellular ATP sustains inflammation. Inflammation increases hepcidin. Hepcidin worsens metal redistribution. The cycle continues.
The persistence problem is therefore different from a simple lack of vitamins or calories. Vitamins and macronutrients can change fairly quickly. Minerals and metals behave differently. They are stored, transported, locked away, released and redistributed by the liver, kidneys, gut, immune system, mitochondria, glutathione system and inflammatory signals. Once this system is disturbed, it may become harder to get essential minerals into the right places and toxic metals out of the wrong places.
In this model, chronic disease is maintained by a locked pattern: low functional minerals, poor ATP chemistry, weak NAD⁺ and NADPH redox, low glutathione capacity, metal misallocation, acetaldehyde burden, histamine excess, extracellular ATP danger signalling, sympathetic overdrive, glutamate elevation, connective tissue instability, microbiome fermentation, immune weakness and repeated inflammatory triggering.
The treatment implication is that fixing one input may not be enough. Adding one vitamin, one mineral, one antimicrobial, one anti-inflammatory or one diet change may help briefly, but may fail if the wider system remains locked. The goal would be to restore coordination: improve mineral transport, rebuild glutathione, restore NAD⁺ and NADPH balance, reduce acetaldehyde and peroxynitrite stress, improve glycogen storage, calm histamine signalling, reduce excessive extracellular ATP danger signalling, restore adenosine and inosine recovery pathways, reduce maladaptive sympathetic drive, support parasympathetic metabolism, stabilise collagen repair and gradually shift the microbiome away from harmful fermentation.
The core claim is not that the body is permanently broken. It is that the body may become trapped in a defensive state that was originally meant to protect it. Over time, that protective state becomes self-sustaining and harmful. Recovery would require carefully interrupting the loops that keep the mineral, redox, immune, histamine, purine, microbiome and nervous-system problems locked together.
One of the challenges in addressing this condition is its cyclic nature - symptoms often improve and worsen in waves. This pattern, combined with inhibited nutrient absorption in the small intestine, makes it extremely difficult to correct mineral deficiencies through diet or oral supplements alone. Research shows that homeostasis for at least 12 minerals / metals may be affected at various times, depending on the state of inflammation.
During chronic inflammation, accurately measuring systemic mineral levels becomes very difficult, because inflammatory signalling changes how minerals move across cell membranes throughout different tissues in the body. Some tissues will store higher amounts of minerals, eg. brain, liver and kidneys, while other tissues will be deficient. Measuring mineral status via serum or red blood cells in this state becomes highly problematic.
Recent studies have uncovered that disruption of key immune regulators, along with ongoing inflammation involving a hormone called hepcidin, disturbs the body's balance of many biologically essential minerals and also heavy metals. These minerals rely on shared transportation systems in our cells called divalent metal transporter 1 and ferroportin. When the mineral + metal status is disrupted, it creates a cascade of additional problems throughout the body.
In conditions such as ME/CFS, long COVID and post vaccine syndrome, the body’s capacity for cellular energy production is undermined. The underlying problem involves mitochondrial dysfunction, whether due to persistent infection, immune activation, resource insufficiency or accumulated tissue damage. When the mitochondria falter, cells are forced to rely more heavily on glycolysis for energy. This shift leads to chronic lactic acid accumulation and a persistent decrease in blood pH.
In response to ongoing metabolic stress and the resulting acidosis, the body triggers a cascade of immune and neuroendocrine signals. The immune system releases inflammatory cytokines, such as IL-6 and TNF-alpha, which then drive the production of hepcidin by the liver. Hepcidin, a key regulator of mineral and metals metabolism, acts on the gut to limit the absorption of iron and related metals by downregulating importers such as DMT1 and exporters such as ferroportin. As a result, the passage of iron and other divalent metals from the diet into the circulation is reduced, and minerals + metals already in the bloodstream become sequestered inside tissues such as the kidneys, liver, spleen, and brain. Where glutathione synthesis is impaired, these heavy metals may accumulate.
This process is initially a protective strategy. By limiting the availability of key minerals, the body restricts resources that pathogens require to thrive. However, in the context of chronic illness where the original threat is not eliminated, this same mechanism persists far beyond its useful window. Over time, a paradox emerges. Blood tests often show low levels of circulating iron, phosphate, and other minerals, while specific tissue stores may remain normal or even elevated. Attempts to supplement minerals can be ineffective, as the transport machinery that moves these nutrients to where they are needed remains switched off or actively reversed.
The ongoing (lactic) acidosis and inflammation also affects the kidneys, which respond by increasing the loss of phosphate, calcium, magnesium, sodium, potassium and zinc in the urine. Since these are required for the synthesis of ATP, its depletion further undermines energy production. The end result is an energy crisis that deepens with each episode of exertion.
Sensing this sustained crisis, the body turns to its last line of defence, the sympathoadrenal system. There is a persistent increase in adrenaline production as the nervous system attempts to compensate for perceived danger. This is experienced as a combination of agitation, racing heart, tremor, and anxiety layered atop profound fatigue. Instead of resolving the energy shortage, these stress signals only amplify the sense of physiological emergency, setting the stage for worsening symptoms after physical or mental activity.
Endogenous morphine signalling and sympathetic drive pull the
cyclic adenosine monophosphate-protein kinase A axis, (cAMP-PKA), in
opposite directions, yet over time they converge on the same
transcription factor, the cAMP response-element binding protein (CREB).
Activation of µ-opioid receptors engages the inhibitory G-protein family
(Gi), suppresses adenylyl cyclase, lowers basal cAMP and reduces PKA
activity. In compensation, neurons and hepatocytes increase expression
of certain cyclase isoforms, of the catalytic sub-unit of PKA and of
CREB itself, gradually restoring throughput despite continuing receptor
inhibition. Sympathetic tone, arriving through β-adrenergic stimulatory
G-proteins (Gs), pushes cAMP the other way; each burst of adrenaline,
also called epinephrine, now strikes tissue that has already multiplied
its signalling hardware.
The result is a primed system that
appears stable while endogenous morphine persists yet stores potential
energy in surplus adenylyl cyclase and poised PKA. Once phosphorylated,
CREB drives transcription of more cyclase, more PKA and, in neurons, of
tyrosine hydroxylase, thereby increasing catecholamine synthesis.
Hepatocytes receiving the same molecular message phosphorylate glycogen
phosphorylase, switch off glycogen synthase and release glucose
immediately. When endogenous morphine production falters or is abruptly
blocked, the Gi restraint disappears, cAMP rises rapidly and the
accumulated PKA is unleashed within minutes. Sympathetic drive, already
high because mitochondrial efficiency is low and hepatic glycogen
scarce, now meets no opposition; adrenaline surges, blood glucose
oscillates and extra-synaptic N-methyl-D-aspartate (NMDA) receptors
become fully phosphorylated by elevated levels of released glutamate, lowering their activation threshold and
producing the familiar excitotoxic features of withdrawal.
Within
this cascade CREB serves as the molecular memory of every prior
fluctuation. Each bout of sympathetic overdrive or transient opioid
deficit leaves behind additional CREB protein and its gene products,
shortening the interval from stimulus to metabolic consequence. The
patient therefore drifts into a state where small changes in endogenous
morphine output, histamine release or catecholamine load provoke
disproportionate swings in glucose availability, heart rate and cortical
excitability—instability that underlies the pacing challenge addressed
in this protocol.
Interventions that reduce cAMP production,
accelerate its breakdown or compete for CREB-dependent transcription
restore margin. The objective is not to abolish sympathetic signalling or CREB
phosphorylation but to shrink their excursions so that hepatic glycogen
can recover, mitochondrial redox can normalise and the system regains
the elasticity lost through repeated compensatory cycles.
Clinically, the primary cycle is seen as persistent fatigue that is unrelieved by rest, recurrent post-exertional crashes, and laboratory findings of low serum iron or phosphate with dysregulated ferritin. Neurological symptoms, such as poor concentration, temperature instability, and orthostatic intolerance, are common. Standard supplementation of iron or other minerals rarely produces sustained benefit because the underlying pattern of restricted absorption and pathological sequestration is not addressed.
The persistence of this state reflects the body’s failure to clear the original insult, whether it is an unresolved infection, ongoing tissue injury, or chronic immune activation. The alarm response that should have been brief and decisive becomes maladaptive, locking the system in a defensive posture that slowly undermines every aspect of metabolism.
This pattern is not the result of psychological weakness or lack of effort. Rather, it is a measurable, predictable, and highly conserved biological response that has become stuck due to the failure to resolve its initiating cause. Effecting recovery requires addressing the source of the ongoing alarm, not simply replacing what is lost downstream.
We have further observed that other minerals become depleted in this disease model. For example, silicon may be lost when it combines with acetaldehyde produced by microorganisms. Zinc is also chelated by acetaldehyde and excreted during acidaemia. Additionally, food intolerances / dietary restrictions and toxins from bacteria or fungi can disrupt zinc and other mineral levels in the body.
When certain minerals become deficient, it affects numerous bodily functions. For instance, shortages of minerals like lithium and rubidium can worsen brain chemistry and kidney function. Impaired kidneys then lead to electrolyte imbalances that disrupt energy production, nerve function, immune activity, and muscle contractions—including those of the heart. This creates a progressive array of cycles which further weaken the immune system and severely disrupts the beneficial microbe communities throughout the body.
The resulting chain reaction affects numerous bodily systems: our immune system becomes dysregulated, brain chemical balances shift, stress hormone levels change, vitamin metabolism alters, cholesterol production fluctuates, and regulation of histamine, hormones, kidney function, and even body temperature becomes compromised.
Early testing of this experimental treatment protocol has shown encouraging results. Some individuals have achieved long-term remission, while others are showing significant improvement on their path to recovery. Formal clinical trials are now being organised to study these effects more systematically.
This pattern of metabolic disruption appears in many infections and chronic health conditions. Associated problems include dysregulated innate immune response, cellular energy production issues, low oxygen levels within cells, nervous system dysfunction, histamine regulation problems, and challenges in producing collagen.
As research continues, patterns of deficiencies and biomarkers may help characterise subgroups and guide hypotheses about disease features and severity, rather than providing reliable individual prediction on their own. [121] [122] [123] [124] This growing understanding is continuously improving treatment approaches, offering new hope for those suffering from these challenging conditions.
The intervention protocol continues to evolve as we uncover more about how these complex systems interact and how homeostasis can be restored more efficiently.
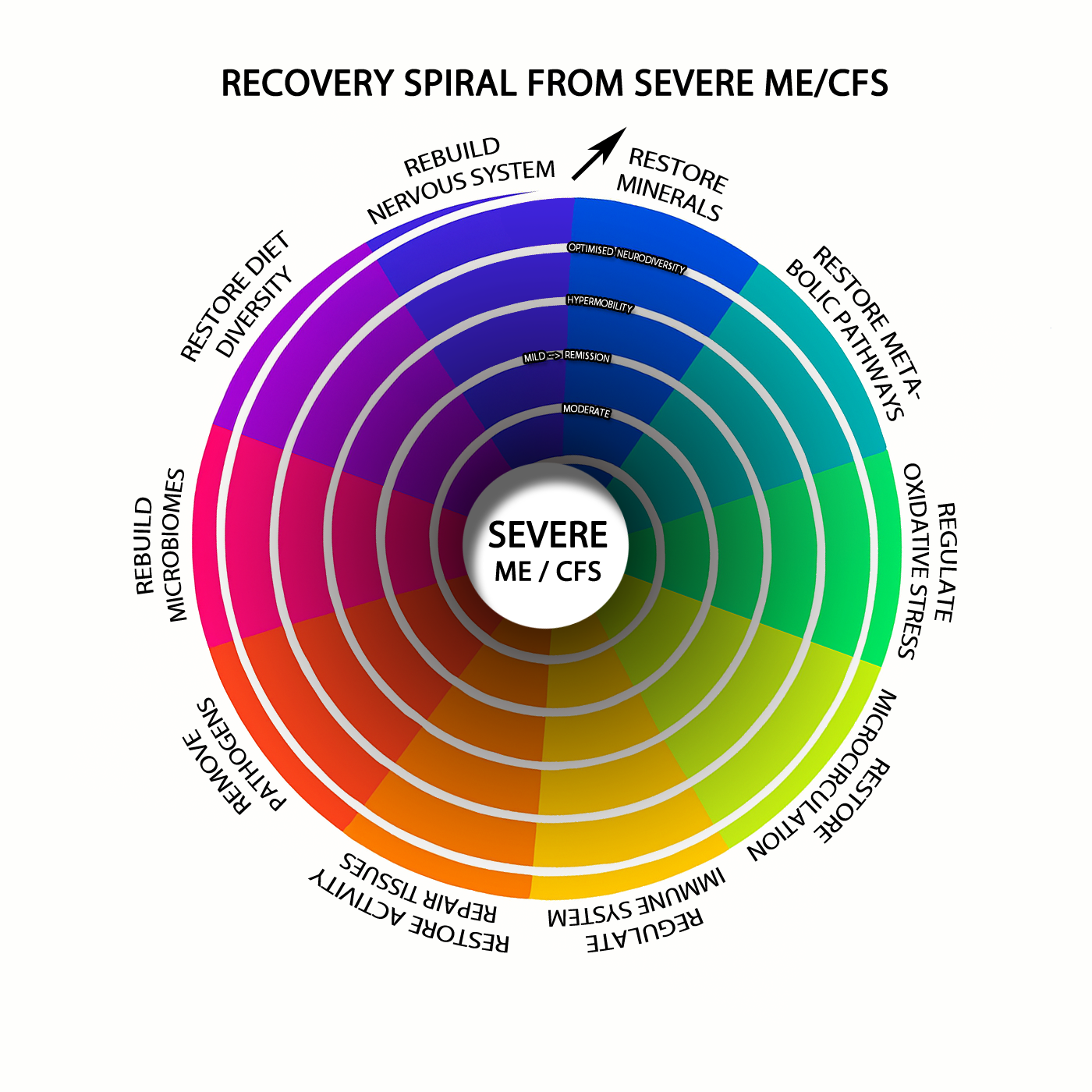
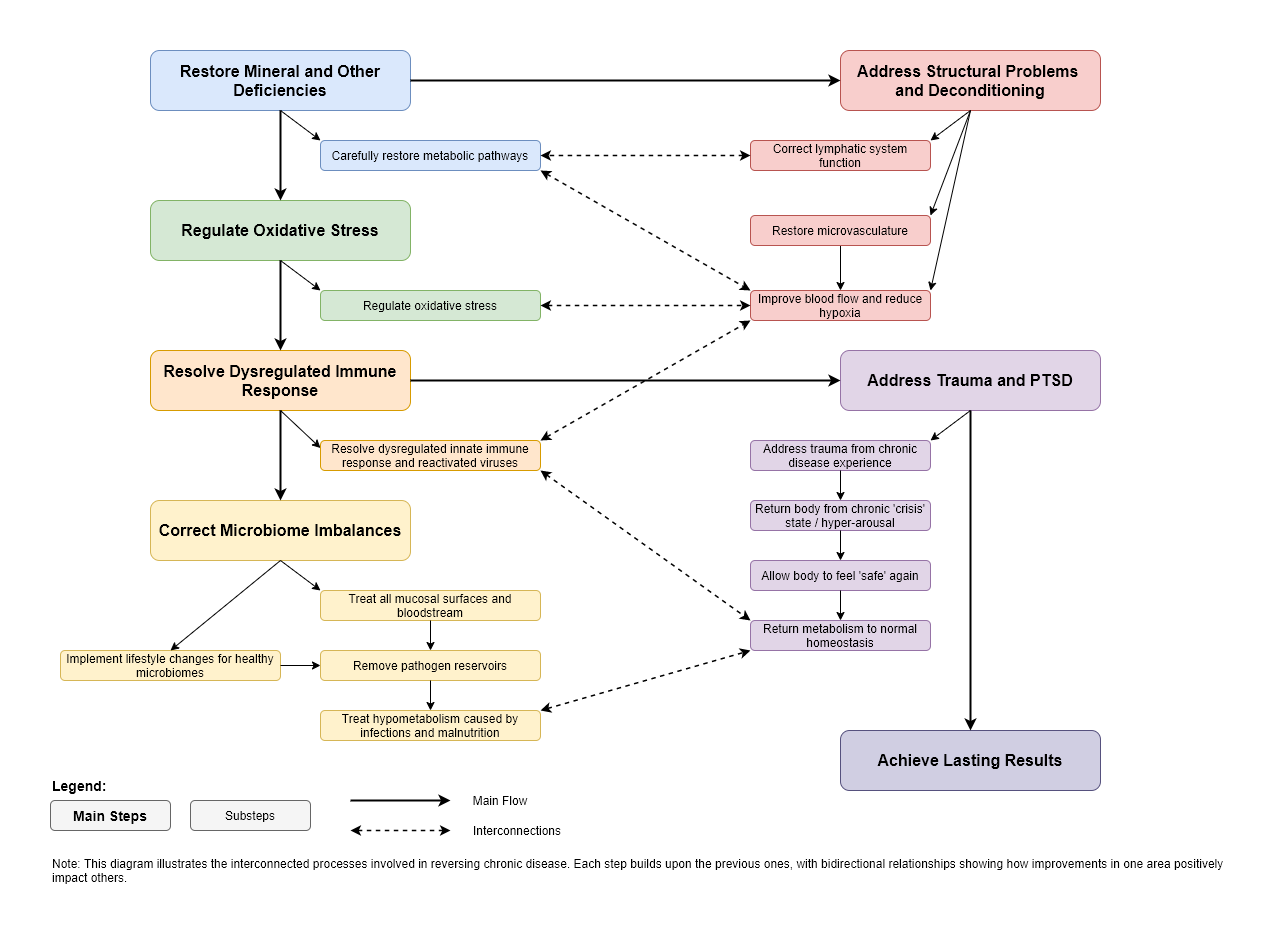
Reversing the Trajectory
To reverse this progression, several key issues need to be addressed:
Fixing mineral and other deficiencies, while removing toxic metals is crucial, as it helps restore energy metabolism pathways, manage oxidative stress, and resolve issues with dysregulated innate immune response pathways, allowing chronic reactivating human herpesviruses, chronic Lyme, T. gondii, etc.
Correcting imbalances in the microbiome, biofilms, and infections by treating all mucosal surfaces and the bloodstream. This removes reservoirs of pathogens and ongoing production of mycotoxins / endotoxins. Employing lifestyle changes which cultivate healthy microbiomes also helps create ongoing resilience against future dysbiosis / infections.
Addressing structural problems involving posture and/or the lymphatic system, plus related structures can improve blood flow and reduce hypoxia.
"Living" with chronic disease understandably creates significant trauma. Dealing with trauma / PTSD imprinting from the daily experience, let alone any medical missteps or gaslighting that may have occurred, AFTER sufficiently treating the hypometabolism and impaired parasympathetic signalling / glycogen metabolism created by the infections and induced malnutrition, is also an essential step for a complete recovery.This allows the body to return from a chronic "crisis" state, thereby removing any limbic system and other influences which also affect neurotransmitters, energy metabolism, and immune activity. While stellate ganglion blocks are a useful example of how we can "hack" autonomic dysregulation, there are better ways to achieve lasting results.
(eg. With an abused animal, it takes some time and nurturing for it to learn to feel "safe" again after experiencing significant trauma and it certainly will not allow itself to feel safe while the abuse is ongoing.
With chronic disease, the "threats" from pathogens and metabolic impairments needs to be sufficiently resolved before you can work on the associated trauma to "feel safe in your own body" again and allow your metabolism to return to normal homeostasis.)
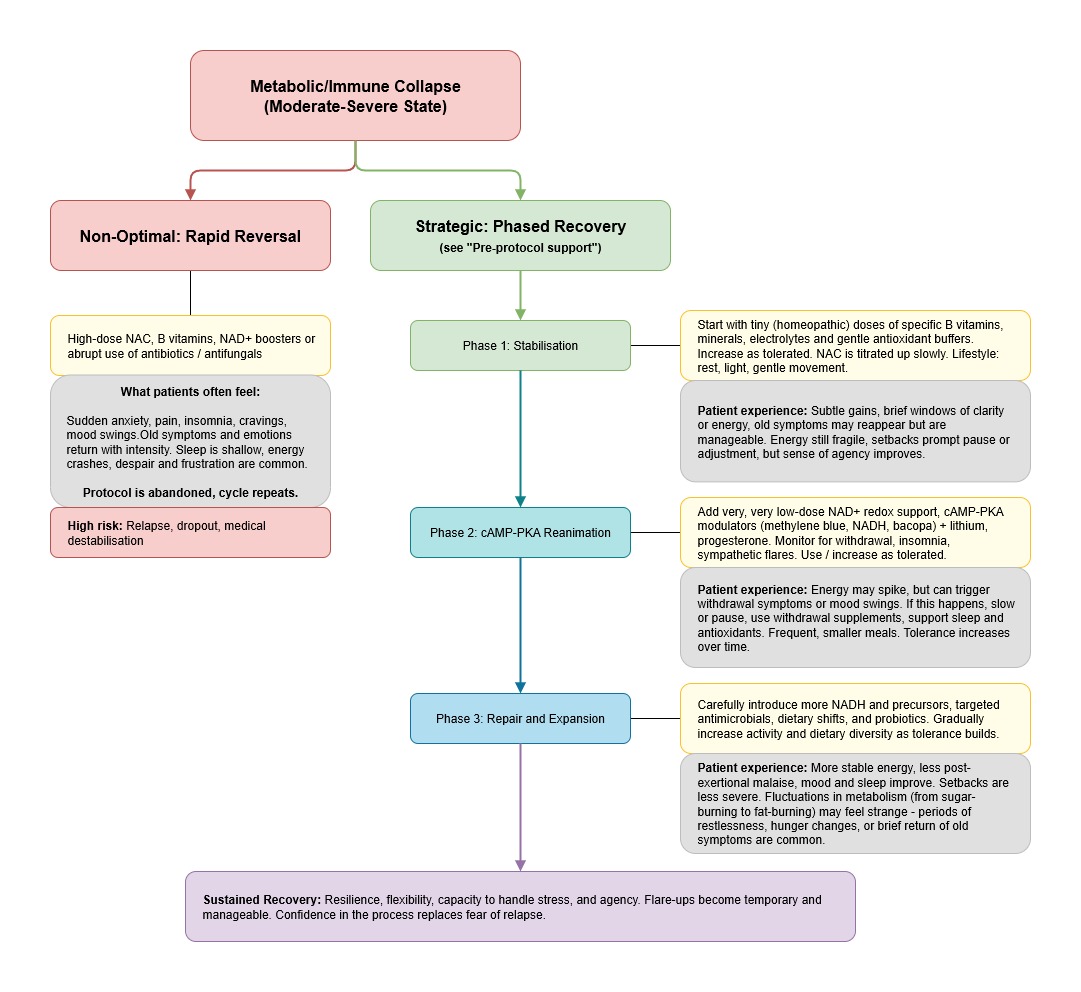
Recovering from severe metabolic and immune collapse
(What it feels like and how to navigate the process)
Emerging from a state of metabolic and immune collapse is one of the most difficult journeys a patient can face. The system has been locked down, in part to prevent further damage, but also as a side effect of depleted resources and chronic acetaldehyde -> endogenous morphine toxicity. Recovery requires not just reversing this shutdown but restoring the underlying machinery that allows for energy, repair, and regulation. In practice, this is rarely a smooth ascent. The process brings with it both physical and psychological challenges, many of which are misunderstood or unexpected. Both patients and clinicians need to understand the risks and manage expectations, since even the best-designed protocol will test patience, adaptability, and resilience.
(The non-optimal approach - rapid reversal, a wall of withdrawal misery and probable failure)
Imagine a patient or clinician, frustrated by stagnation, decides to "break through" the problem with an aggressive protocol. High-dose antioxidants, NAD+ boosters, or acetaldehyde-scavenging agents are started all at once, sometimes with sudden dietary changes or antimicrobial use, causing abrupt withdrawal of microbial alcohol/acetaldehyde. The intention is good, but the system is not ready.
In the first hours or days, the patient may feel a fleeting surge of clarity or energy. This is soon followed by a constellation of severe symptoms. There is often a sense of being "stripped raw" - anxiety, irritability, and insomnia appear, alongside joint pain, sweats, and waves of fatigue that no amount of rest can resolve. Sleep becomes shallow or fragmented. Some experience palpitations, tremors, or a sense of impending doom. The gut may revolt, with loose stools or cramping. Old cravings return, sometimes stronger than ever, as the nervous system grasps for anything to restabilise itself.
Psychologically, this process can be distressing. Emotions that were blunted by the previous metabolic state can re-emerge with intensity. Old traumas may resurface. Some patients feel despair or hopelessness, convinced they are getting worse, not better. The protocol is abandoned, or reversed, and a sense of failure can set in. For many, this pattern repeats, leading to cycles of boom-and-bust or deepening fatigue.
The strategic approach - staged recovery, while maintaining honest expectations
An optimal recovery strategy recognises that the system cannot simply be "switched back on" and the more severe the patient, the more gentle the reversal process needs to be.
It involves a slow, methodical rebuilding, supporting the most fragile processes first before removing the blocks that have accumulated. Recovery starts with the smallest possible doses of exogenous NAD+, active B vitamins, and minerals, in severe cases, much lower than most would expect. Toxic metals are removed. Carbohydrate intakes are usually increased significantly as the metabolism is restored.
Acetaldehyde scavengers like NAC, DHM, Acetium, Z-Biotics or L-carnosine are introduced cautiously, and their doses are only increased if the patient remains stable. Antioxidant buffers are included early on, and lifestyle interventions such as light exposure, gentle movement, and sleep support are prioritised.
During this phase, the patient may notice only subtle changes at first: brief windows of mental clarity, a slight reduction in heaviness, or the return of some appetite. Occasionally, there are small setbacks - a night of poor sleep, muscle aches, or old symptoms resurfacing. These are not failures, but signs that the underlying machinery is coming back online. The protocol is adjusted in response, slowing down or pausing when symptoms flare.
Only after this foundation is established are cAMP-PKA modulators and NAD+ precursors introduced, and always at low doses. The body’s response is closely monitored. If symptoms of withdrawal, anxiety, or immune flares reappear, the approach is paused or scaled back. As the patient tolerates more, the protocol expands to include targeted anti-microbials, more significant dietary shifts, and finally, prebiotics + probiotics to rebuild the microbiome.
Recovery remains non-linear, and setbacks are part of the process. Patients can expect periods of improved energy or mood, followed by plateaus or short-lived regressions. Emotions may feel more "alive" but also less buffered. There is often a phase of emotional thaw, where old memories or unresolved stress emerge. The most important factor is that progress is gradual and symptoms are manageable. Each setback is an opportunity to learn and recalibrate, not a sign of failure.
The patient’s sense of agency grows as they begin to notice and interpret their own responses. Trust in the process is built not on relentless progress, but on the ability to pause, recover, and continue. The clinician’s role is to validate these experiences, explain what is happening, and remind the patient that, while difficult, this approach offers the best chance for genuine, lasting recovery.
Experiencing metabolic recovery - what it feels like as your energy systems recover
During collapse, the body is stuck in emergency mode. Glycolysis is inefficient, fatty acid oxidation is blunted, and lactic acid accumulates quickly with even mild exertion. Most energy comes from "burning sugar poorly," which leaves the patient exhausted after trivial effort. Muscles ache, and small exertions can bring on a disproportionate sense of heaviness or even mild acidosis. After activity, recovery is slow. There may be a background sense of internal "sourness," and sleep does little to replenish energy.
As the protocol progresses and the first cracks appear in this rigid metabolic state, changes can be both subtle and disorienting. When cAMP-PKA tone begins to improve and the first traces of mitochondrial support arrive, the patient might notice short bursts of energy - windows where movement feels lighter or less taxing. This is the nervous system and muscle tissue rediscovering how to use glycolysis more efficiently. Instead of every effort being punished by burning muscles and a leaden fatigue, there are moments when exertion is merely tiring, not overwhelming.
Fatty acid oxidation often lags behind. When it begins to recover, it may be heralded by a curious combination of sensations: steadier background energy, reduced need for snacking or sugar, and a less dramatic crash after activity. For some, this comes with a brief resurgence of "keto flu" symptoms - headache, brain fog, mild nausea, or a peculiar sensation of metabolic unease - as the body relearns how to mobilise and process fats. Old symptoms like mild hypoglycaemia or even transient palpitations can flare, but now they respond more quickly to rest or a small snack.
During this metabolic recalibration, patients may also experience sudden swings between energy systems. A good day might be followed by a day of heaviness, as the system "practices" new flexibility. It is normal for the body to default to the old, rigid state during stress, infection, or after a poor night’s sleep. With patience and support, these fluctuations even out. Activity can be sustained for longer, with less muscle soreness or lactic "burn," and post-exertional malaise becomes less severe and shorter in duration. Carbohydrate intake requirements may rapidly increase.
Sleep also shifts. Early in recovery, sleep may feel light, fractured, or unrefreshing. As mitochondrial and fatty acid pathways revive, sleep deepens, dreams become more vivid, and the feeling upon waking gradually improves. Hunger and satiety cues become clearer. Cravings for sugar or stimulants diminish as the brain and muscles regain access to stored energy.
Throughout, patients should expect this journey to feel unfamiliar. However, the return of metabolic flexibility often means confronting both old symptoms and new sensations. Some will feel bursts of restlessness or drive, as the nervous system recalibrates. Others will notice mood swings or emotional thaw, reflecting not just the lifting of metabolic brakes but the return of a more "awake" brain. These are all signs that the underlying system is no longer stuck, even if the new equilibrium is fragile.
The clinician’s role is to remind patients that each shift - pleasant or uncomfortable - is a signal that the machinery is coming back online. Setbacks are common, and relapses into fatigue or brain fog do not mean the process has failed. Rather, they are cues to adjust pace, optimise rest, and allow for further healing.
Overall, the experience of recovery is one of transition - from a brittle, highly-reactive system to a more robust, flexible network capable of burning both glucose and fat. Progress is not linear, but with patience and appropriate support, the system regains resilience. Each step, even the uncomfortable ones, is a movement toward a more sustainable and adaptable state.