by
Joshua Leisk | (@joshual_tm on X/Twitter)
[Please note, this is a large webpage (>250 printable pages) with dynamic content. A quick-start guide can be found here. Please allow a few moments for all database tables to load.]
What's new?
Here are the 10 most recent changes / updates:For more detailed information, please see Changelog
Please report any bugs / errors.
NB. Whilst efforts have been made to make this information accessible on mobile devices, it is best viewed on a computer.
This is an experimental protocol based on the disease model by Leisk et al., (preview here - https://bornfree.life/learn/) which may be helpful for supporting the unique nutritional and wellness / lifestyle requirements of teenagers and adults with chronic illnesses that share various common features, including mitochrondrial dysfunction, hormone dysregulation, ferritin and other mineral deficiencies, microbiome dysbiosis, biofilms, neurotransmitter dysregulation and immune dysregulation, etc., such as:
| Myalgic Encephalomyelitis / Chronic Fatigue Syndrome (ME/CFS) | Long COVID, Post-Vaccine Syndrome | Viral / Post-Viral Chronic Fatigue |
| Post-Exertional Malaise (PEM) | “Floxed” | Guillain-Barre Syndrome (GBS) |
| Chronic Inflammatory Response Syndrome (CIRS) | Breathlessness | Hypoxia |
| Acidosis / Alkalosis / pH Dysregulation | Dysregulated Cortisol | Dyslipidemia |
| Post Finasteride Syndrome (PFS) | Post SSRI Sexual Dysfunction (PSSD) | Post Accutane Syndrome |
| Small Fibre Peripheral Neuropathy (SFPN) | Mast Cell Activation Syndrome (MCAS) | Diamine Oxidase (DAO) Deficiency |
| Stiff Person Syndrome | Gut Fermentation Syndrome | Glycogen Storage Disease (functional) |
| Histamine intolerance | Brain Fog | Sleep disorders |
| Anxiety | Postural Orthostatic Tachycardia Syndrome (POTS) | Autism Spectrum Disorders (ASD) |
| Fibromyalgia | Dysautonomia | Frequent Urination |
| GI Disorders | “Small Intestinal Bacterial Overgrowth” (SIBO) | Vitamin B6 Toxicity |
| Vitamin A Toxicity | Candidiasis | Aspergillosis |
| Ehlers Danlos Syndrome (EDS) | Joint Pain | Connective Tissue Disorders |
| Macular Degeneration | Multiple Sclerosis (MS) | Parkinson's Disease (PD) |
| Tinnitus | Polycystic Ovary Syndrome (PCOS) | Erectile Dysfunction |
| Elevated Cholesterols / Fasting Glucose / D-Dimer | Hashimotos | Alopecia |
| Major and other types of Depression | Cataracts | Migraines |
Please read the entire protocol documentation before taking any action based on its contents.
This protocol is for research and educational purposes only. Always consult your doctor to determine if this information is appropriate for you, especially if you are taking medications like SNRIs/SSRIs, beta-blockers, MAO inhibitors, or drugs metabolized by CYP2D6 enzymes.
Important Notice:
While we strive to minimize adverse effects, you may experience some temporary symptoms when starting this protocol -
- Paradoxical Effects: As deficiencies are corrected and neurotransmitter balance is restored, you might notice short-term increases in adrenaline and heart rate.
- Copper Deficiency Correction: Addressing a severe copper deficiency may cause temporary kidney pain and nausea.
- Immune Activity Increase: An initial boost in energy availability can heighten immune activity and symptom severity. This might be psychologically challenging and may cause hesitation in continuing the process.
- Herxheimer Reactions: You may experience effects from microbial die-off, such as increased "burning" sensations and headaches.
- Hormonal Changes: Temporary changes in libido or menstrual cycles can occur.
- Inflammation and Flu-like Symptoms: Improvements in immune function might lead to brief periods of inflammation, fever, flu-like symptoms, nausea, and fatigue.
Support:
We host an online discussion and support group on Discord. Feel free to join us:
Monitoring Recommendations:
In addition to the tests used in the protocol, we suggest regular blood tests to monitor:
- D-dimer Levels
- Vitamin B6 Levels
- Cholesterol Levels
- Fasting Glucose Levels
Warning: This documentation contains a significant amount of information and it is expected that you will need multiple read-throughs and a number of hours to absorb and / or action the information.
How to Navigate This Information
There are multiple ways to approach this material:
First Reading: We suggest that you read everything from start to finish in a linear fashion. This will help you become acquainted with all of the concepts.
Guided Navigation: If you decide to act on the information, return here and use the visual navigation tool below to step through the protocol in a logical and structured manner.
- AI-supported (experimental): If you would like AI assistance in understanding the model and/or protocol, Google's NotebookLM is able to perform this function for free. A setup guide is available here - https://bornfree.life/learn/notebooklm-ai/
Overview of the Protocol
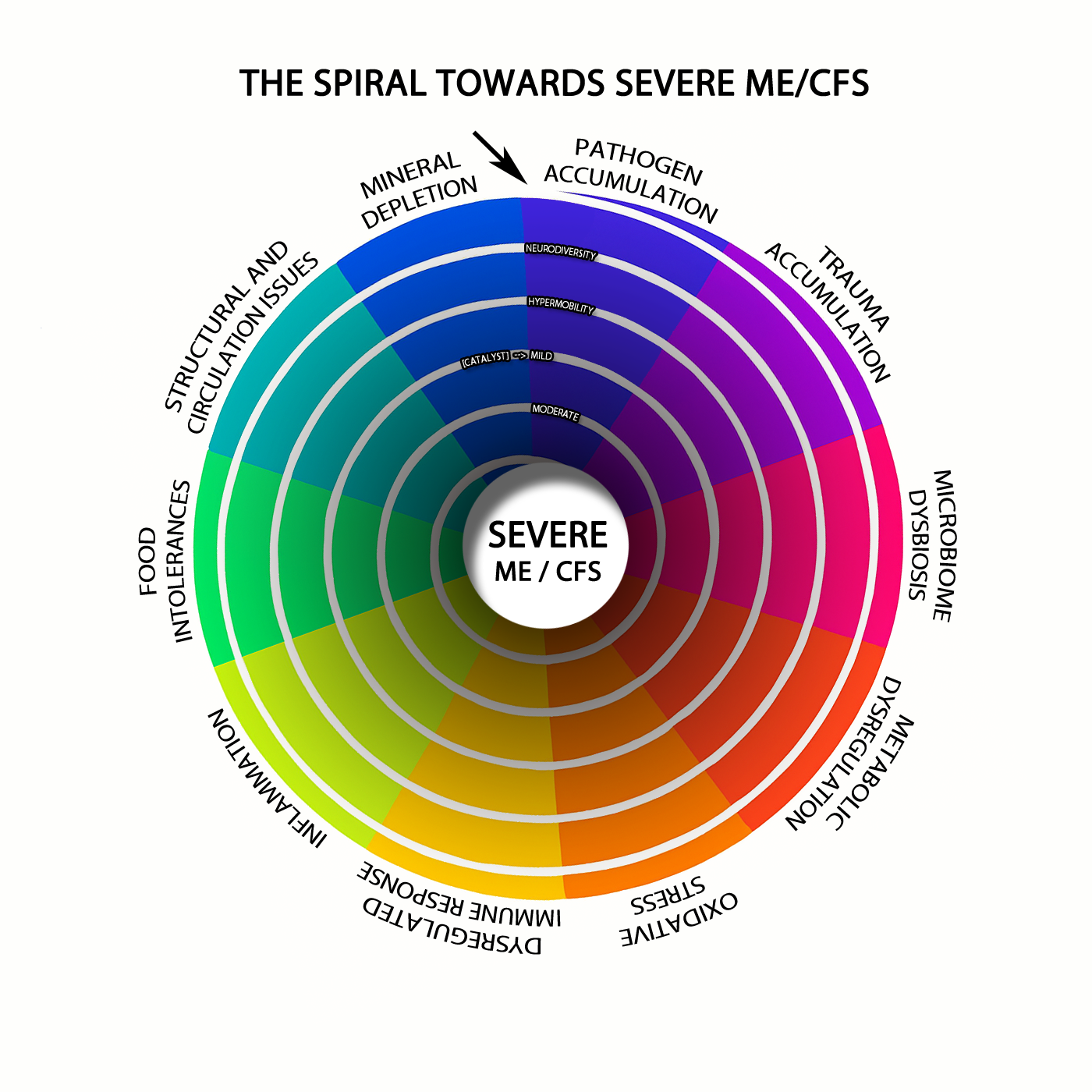
This disease model this protocol is based on describes the downstream effects of various blind spots in our immune system which further explain why some health problems become chronic and/or develop into progressive diseases.
This understanding reveals how some harmful microorganisms can hide within protective shields called "biofilms" throughout our bodies - in places like our nose, mouth, lungs, digestive tract, reproductive organs, and even our bloodstream. (Other microorganisms may also hide in parasitic "cysts" and fibrin "nests".)
These biofilms begin forming during childhood, typically growing slowly over many years. Collected data suggests this gradual buildup might be connected to what we consider as natural aging processes. However, when the immune system faces challenges from infections, medical procedures, medications, injuries, poor nutrition, or ongoing stress, these biofilms can grow much more rapidly.
In a healthy body, the immune system keeps biofilms in check by detecting and attacking pathogenic microorganisms when they venture outside these protected areas. A sufficiency of beneficial "probiotic" species can also degrade biofilms and attack pathogens.
When this defense system becomes compromised, the biofilms can increase their surface area and some of these hidden microorganisms then produce an increasing amount of harmful substances, particularly a toxin called acetaldehyde - the same compound produced when your body processes alcohol. Chronic acetaldehyde production can cause the body to produce morphine, creating further symptoms of tolerance and dependence.
This toxin disrupts cellular energy production and damages both your immune system and the lining of your digestive tract. A damaged gut lining allows more harmful microorganisms to cross this critical barrier, triggering an immune response aimed at eliminating these invaders. The resulting long-term inflammation and hypoxia can transform temporary mineral shortages into serious, system-wide deficiencies that are difficult to detect and correct.
One of the challenges in addressing this condition is its cyclic nature - symptoms often improve and worsen in waves. This pattern, combined with inhibited nutrient absorption in the small intestine, makes it extremely difficult to correct mineral deficiencies through diet or oral supplements alone. Research shows that homeostasis for up to eleven metals may be affected at various times, depending on the state of inflammation.
During chronic inflammation, accurately measuring systemic mineral levels becomes very difficult, because inflammatory signalling changes how minerals move across cell membranes throughout different tissues in the body. Some tissues will store higher amounts of minerals, eg. brain, liver and kidneys, while other tissues will be deficient. Measuring mineral status via serum or red blood cells in this state becomes highly problematic.
Recent studies have uncovered that disruption of key immune regulators, along with ongoing inflammation involving a hormone called hepcidin, disturbs the body's balance of many biologically essential metals. These minerals rely on shared transportation systems in our cells called divalent metal transporter 1 and ferroportin. When the mineral status is disrupted, it creates a cascade of additional problems throughout the body.
In conditions such as ME/CFS, long COVID and post vaccine syndrome, the body’s capacity for cellular energy production is undermined. The underlying problem involves mitochondrial dysfunction, whether due to persistent infection, immune activation, resource insufficiency or accumulated tissue damage. When the mitochondria falter, cells are forced to rely more heavily on glycolysis for energy. This shift leads to chronic lactic acid accumulation and a persistent decrease in blood pH.
In response to ongoing metabolic stress and the resulting acidosis, the body triggers a cascade of immune and neuroendocrine signals. The immune system releases inflammatory cytokines, such as IL-6 and TNF-alpha, which then drive the production of hepcidin by the liver. Hepcidin, a key regulator of mineral metabolism, acts on the gut to limit the absorption of iron and related metals by downregulating importers such as DMT1 and exporters such as ferroportin. As a result, the passage of iron and other divalent metals from the diet into the circulation is reduced, and metals already in the bloodstream become sequestered inside tissues such as the liver, spleen, and brain.
This process is initially a protective strategy. By limiting the availability of key metals, the body restricts resources that pathogens require to thrive. However, in the context of chronic illness where the original threat is not eliminated, this same mechanism persists far beyond its useful window. Over time, a paradox emerges. Blood tests often show low levels of circulating iron, phosphate, and other minerals, while specific tissue stores may remain normal or even elevated. Attempts to supplement minerals can be ineffective, as the transport machinery that moves these nutrients to where they are needed remains switched off or actively reversed.
The ongoing (lactic) acidosis and inflammation also affects the kidneys, which respond by increasing the loss of phosphate, calcium, magnesium, sodium, potassium and zinc in the urine. Since these are required for the synthesis of ATP, its depletion further undermines energy production. The end result is an energy crisis that deepens with each episode of exertion.
Sensing this sustained crisis, the body turns to its last line of defence, the sympathoadrenal system. There is a persistent increase in adrenaline production as the nervous system attempts to compensate for perceived danger. This is experienced as a combination of agitation, racing heart, tremor, and anxiety layered atop profound fatigue. Instead of resolving the energy shortage, these stress signals only amplify the sense of physiological emergency, setting the stage for worsening symptoms after physical or mental activity.
Endogenous morphine signalling and sympathetic drive pull the
cyclic adenosine monophosphate-protein kinase A axis, (cAMP-PKA), in
opposite directions, yet over time they converge on the same
transcription factor, the cAMP response-element binding protein (CREB).
Activation of µ-opioid receptors engages the inhibitory G-protein family
(Gi), suppresses adenylyl cyclase, lowers basal cAMP and reduces PKA
activity. In compensation, neurons and hepatocytes increase expression
of certain cyclase isoforms, of the catalytic sub-unit of PKA and of
CREB itself, gradually restoring throughput despite continuing receptor
inhibition. Sympathetic tone, arriving through β-adrenergic stimulatory
G-proteins (Gs), pushes cAMP the other way; each burst of adrenaline,
also called epinephrine, now strikes tissue that has already multiplied
its signalling hardware.
The result is a primed system that
appears stable while endogenous morphine persists yet stores potential
energy in surplus adenylyl cyclase and poised PKA. Once phosphorylated,
CREB drives transcription of more cyclase, more PKA and, in neurons, of
tyrosine hydroxylase, thereby increasing catecholamine synthesis.
Hepatocytes receiving the same molecular message phosphorylate glycogen
phosphorylase, switch off glycogen synthase and release glucose
immediately. When endogenous morphine production falters or is abruptly
blocked, the Gi restraint disappears, cAMP rises rapidly and the
accumulated PKA is unleashed within minutes. Sympathetic drive, already
high because mitochondrial efficiency is low and hepatic glycogen
scarce, now meets no opposition; adrenaline surges, blood glucose
oscillates and extra-synaptic N-methyl-D-aspartate (NMDA) receptors
become fully phosphorylated, lowering their activation threshold and
producing the familiar excitotoxic features of withdrawal.
Within
this cascade CREB serves as the molecular memory of every prior
fluctuation. Each bout of sympathetic overdrive or transient opioid
deficit leaves behind additional CREB protein and its gene products,
shortening the interval from stimulus to metabolic consequence. The
patient therefore drifts into a state where small changes in endogenous
morphine output, histamine release or catecholamine load provoke
disproportionate swings in glucose availability, heart rate and cortical
excitability—instability that underlies the pacing challenge addressed
in this protocol.
Interventions that reduce cAMP production,
accelerate its breakdown or compete for CREB-dependent transcription
restore margin. The objective is not to abolish sympathetic signalling or CREB
phosphorylation but to shrink their excursions so that hepatic glycogen
can recover, mitochondrial redox can normalise and the system regains
the elasticity lost through repeated compensatory cycles.
Clinically, the primary cycle is seen as persistent fatigue that is unrelieved by rest, recurrent post-exertional crashes, and laboratory findings of low serum iron or phosphate with dysregulated ferritin. Neurological symptoms, such as poor concentration, temperature instability, and orthostatic intolerance, are common. Standard supplementation of iron or other minerals rarely produces sustained benefit because the underlying pattern of restricted absorption and pathological sequestration is not addressed.
The persistence of this state reflects the body’s failure to clear the original insult, whether it is an unresolved infection, ongoing tissue injury, or chronic immune activation. The alarm response that should have been brief and decisive becomes maladaptive, locking the system in a defensive posture that slowly undermines every aspect of metabolism.
This pattern is not the result of psychological weakness or lack of effort. Rather, it is a measurable, predictable, and highly conserved biological response that has become stuck due to the failure to resolve its initiating cause. Effecting recovery requires addressing the source of the ongoing alarm, not simply replacing what is lost downstream.
We have further observed that other minerals become depleted in this disease model. For example, silicon may be lost when it combines with acetaldehyde produced by microorganisms. Zinc is also chelated by acetaldehyde and excreted during acidaemia. Additionally, food intolerances / dietary restrictions and toxins from bacteria or fungi can disrupt zinc and other mineral levels in the body.
When certain minerals become deficient, it affects numerous bodily functions. For instance, shortages of minerals like lithium and rubidium can worsen brain chemistry and kidney function. Impaired kidneys then lead to electrolyte imbalances that disrupt energy production, nerve function, immune activity, and muscle contractions—including those of the heart. This creates a progressive array of cycles which further weaken the immune system and severely disrupts the beneficial microbe communities throughout the body.
The resulting chain reaction affects numerous bodily systems: our immune system becomes dysregulated, brain chemical balances shift, stress hormone levels change, vitamin metabolism alters, cholesterol production fluctuates, and regulation of histamine, hormones, kidney function, and even body temperature becomes compromised.
Early testing of this experimental treatment protocol has shown encouraging results. Some individuals have achieved long-term remission, while others are showing significant improvement on their path to recovery. Formal clinical trials are now being organised to study these effects more systematically.
This pattern of metabolic disruption appears in many infections and chronic health conditions. Associated problems include dysregulated innate immune response, cellular energy production issues, low oxygen levels within cells, nervous system dysfunction, histamine regulation problems, and challenges in producing collagen.
As research continues, we are finding that patterns of deficiencies can help predict various disease features and their severity. This growing understanding is continuously improving treatment approaches, offering new hope for those suffering from these challenging conditions.
The intervention protocol continues to evolve as we uncover more about how these complex systems interact and how homeostasis can be restored more efficiently.
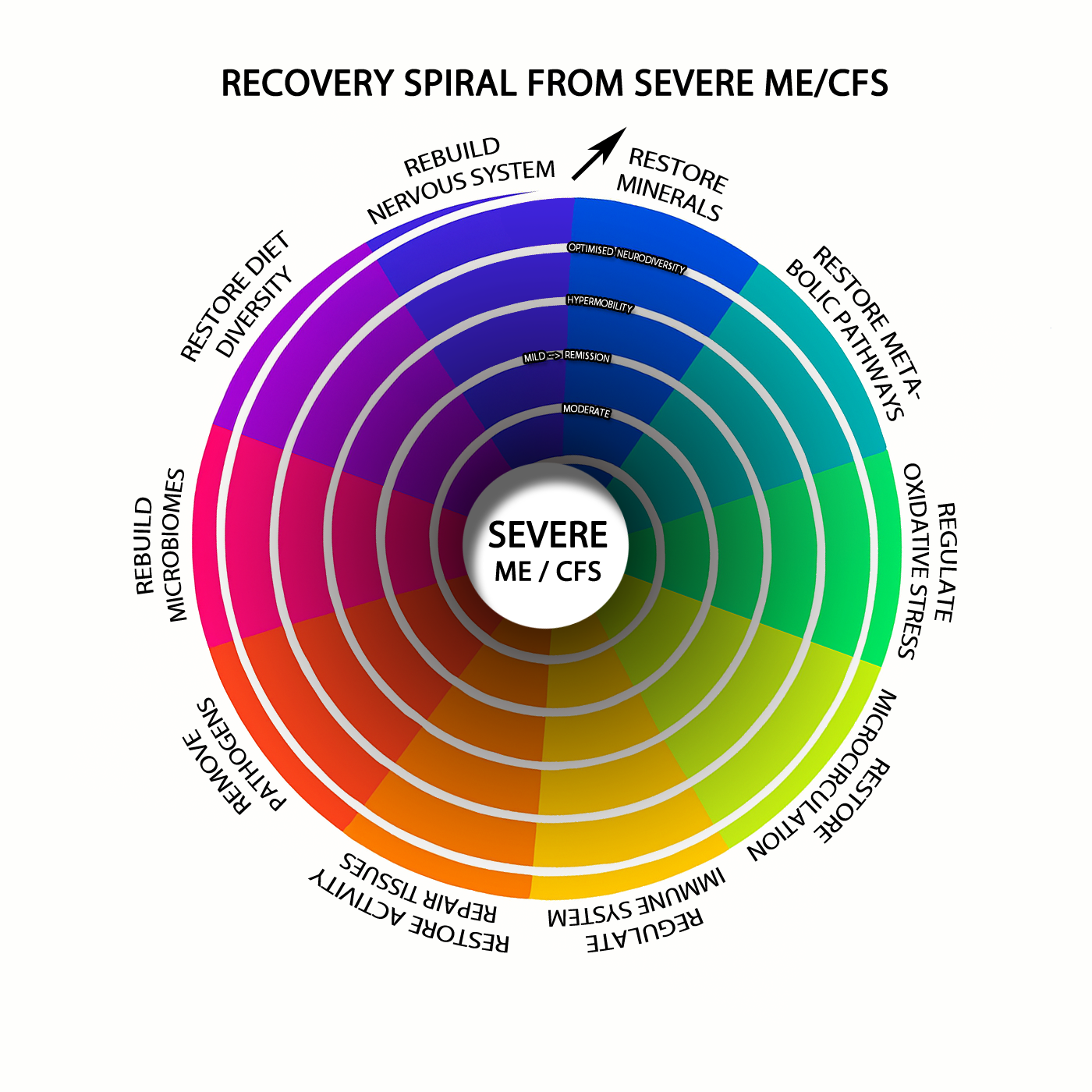
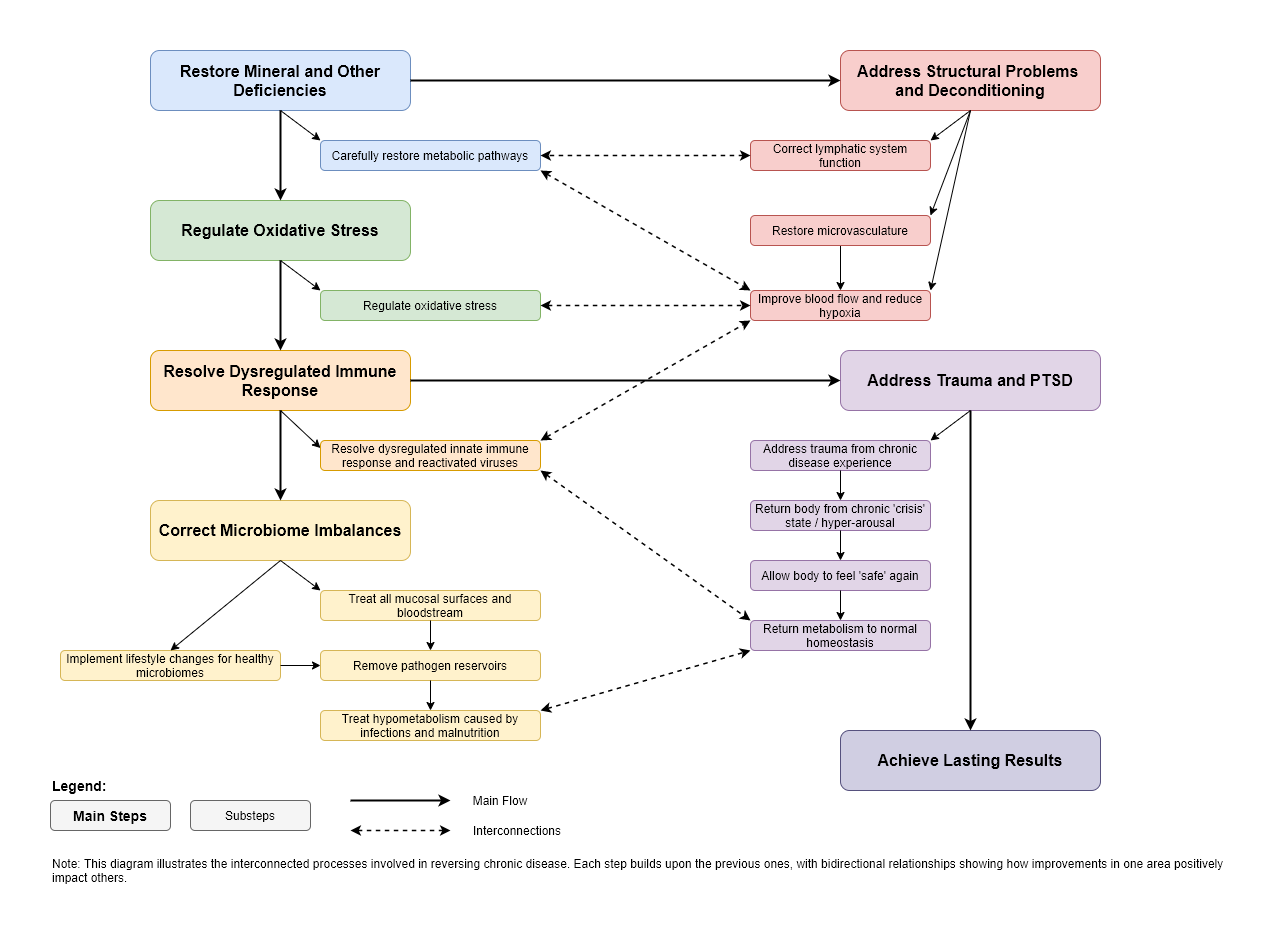
Reversing the Trajectory
To reverse this progression, several key issues need to be addressed:
Fixing mineral and other deficiencies is crucial, as it helps restore energy metabolism pathways, manage oxidative stress, and resolve issues with dysregulated innate immune response pathways, allowing chronic reactivating human herpesviruses, chronic Lyme, T. gondii, etc.
Correcting imbalances in the microbiome, biofilms, and infections by treating all mucosal surfaces and the bloodstream. This removes reservoirs of pathogens and ongoing production of mycotoxins / endotoxins. Employing lifestyle changes which cultivate healthy microbiomes also helps create ongoing resilience against future dysbiosis / infections.
Addressing structural problems involving posture and/or the lymphatic system, plus related structures can improve blood flow and reduce hypoxia.
"Living" with chronic disease understandably creates significant trauma. Dealing with trauma / PTSD imprinting from the daily experience, let alone any medical missteps or gaslighting that may have occurred, AFTER sufficiently treating the hypometabolism created by the infections and induced malnutrition, is also an essential step for a complete recovery.This allows the body to return from a chronic "crisis" state, thereby removing any limbic system and other influences which also affect neurotransmitters, energy metabolism, and immune activity. While stellate ganglion blocks are a useful example of how we can "hack" autonomic dysregulation, there are better ways to achieve lasting results.
(eg. With an abused animal, it takes some time and nurturing for it to learn to feel "safe" again after experiencing significant trauma and it certainly will not allow itself to feel safe while the abuse is ongoing.
With chronic disease, the "threats" from pathogens and metabolic impairments needs to be sufficiently resolved before you can work on the associated trauma to "feel safe in your own body" again and allow your metabolism to return to normal homeostasis.)
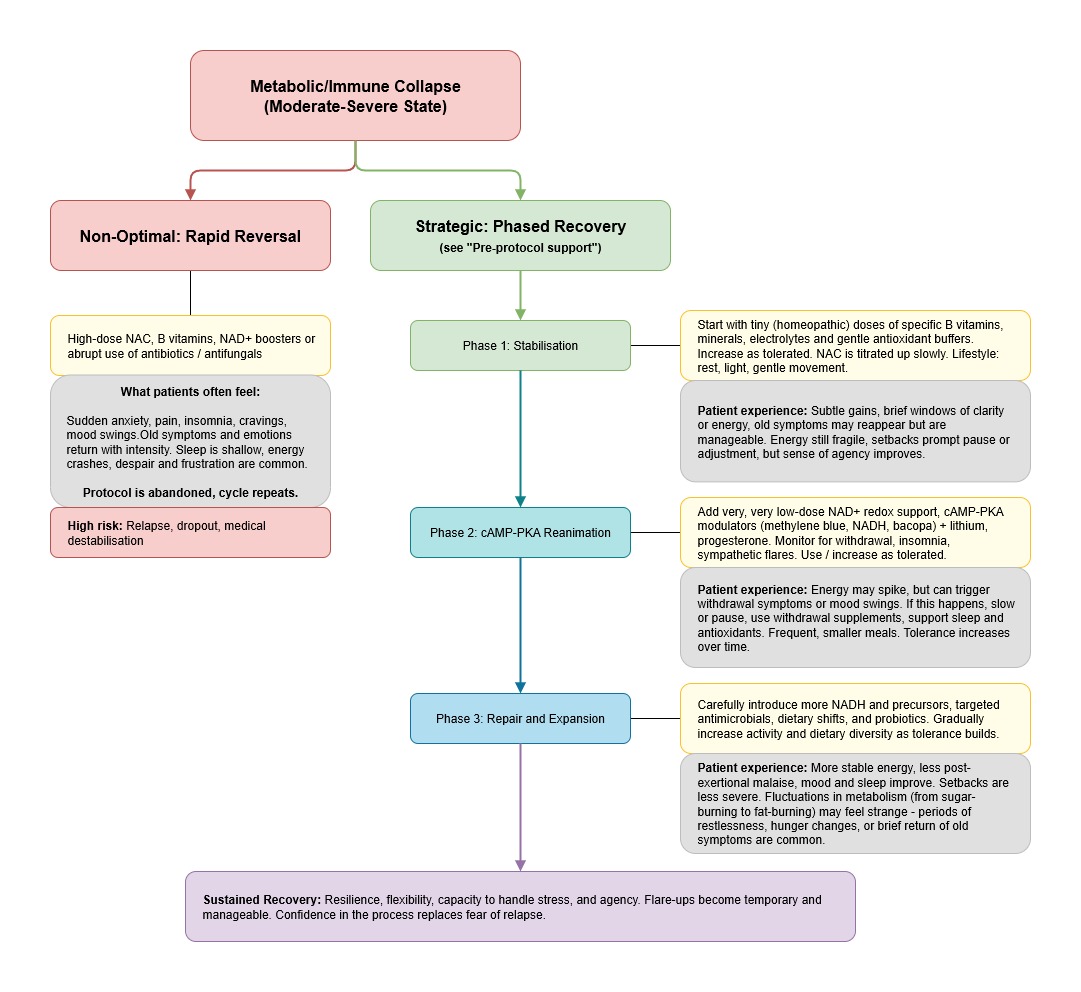
Recovering from severe metabolic and immune collapse
(What it feels like and how to navigate the process)
Emerging from a state of metabolic and immune collapse is one of the most difficult journeys a patient can face. The system has been locked down, in part to prevent further damage, but also as a side effect of depleted resources and chronic acetaldehyde -> endogenous morphine toxicity. Recovery requires not just reversing this shutdown but restoring the underlying machinery that allows for energy, repair, and regulation. In practice, this is rarely a smooth ascent. The process brings with it both physical and psychological challenges, many of which are misunderstood or unexpected. Both patients and clinicians need to understand the risks and manage expectations, since even the best-designed protocol will test patience, adaptability, and resilience.
(The non-optimal approach - rapid reversal, a wall of withdrawal misery and probable failure)
Imagine a patient or clinician, frustrated by stagnation, decides to "break through" the problem with an aggressive protocol. High-dose antioxidants, NAD+ boosters, or acetaldehyde-scavenging agents are started all at once, sometimes with sudden dietary changes or antimicrobial use, causing abrupt withdrawal of microbial alcohol/acetaldehyde. The intention is good, but the system is not ready.
In the first hours or days, the patient may feel a fleeting surge of clarity or energy. This is soon followed by a constellation of severe symptoms. There is often a sense of being "stripped raw" - anxiety, irritability, and insomnia appear, alongside joint pain, sweats, and waves of fatigue that no amount of rest can resolve. Sleep becomes shallow or fragmented. Some experience palpitations, tremors, or a sense of impending doom. The gut may revolt, with loose stools or cramping. Old cravings return, sometimes stronger than ever, as the nervous system grasps for anything to restabilise itself.
Psychologically, this process can be distressing. Emotions that were blunted by the previous metabolic state can re-emerge with intensity. Old traumas may resurface. Some patients feel despair or hopelessness, convinced they are getting worse, not better. The protocol is abandoned, or reversed, and a sense of failure can set in. For many, this pattern repeats, leading to cycles of boom-and-bust or deepening fatigue.
The strategic approach - staged recovery, while maintaining honest expectations
An optimal recovery strategy recognises that the system cannot simply be "switched back on" and the more severe the patient, the more gentle the reversal process needs to be.
It involves a slow, methodical rebuilding, supporting the most fragile processes first before removing the blocks that have accumulated. Recovery starts with the smallest possible doses of exogenous NAD+, active B vitamins, and minerals, in severe cases, much lower than most would expect.
Acetaldehyde scavengers like NAC, DHM, Acetium, Z-Biotics or L-carnosine are introduced cautiously, and their doses are only increased if the patient remains stable. Antioxidant buffers are included early on, and lifestyle interventions such as light exposure, gentle movement, and sleep support are prioritised.
During this phase, the patient may notice only subtle changes at first: brief windows of mental clarity, a slight reduction in heaviness, or the return of some appetite. Occasionally, there are small setbacks - a night of poor sleep, muscle aches, or old symptoms resurfacing. These are not failures, but signs that the underlying machinery is coming back online. The protocol is adjusted in response, slowing down or pausing when symptoms flare.
Only after this foundation is established are cAMP-PKA modulators and NAD+ precursors introduced, and always at low doses. The body’s response is closely monitored. If symptoms of withdrawal, anxiety, or immune flares reappear, the approach is paused or scaled back. As the patient tolerates more, the protocol expands to include targeted anti-microbials, more significant dietary shifts, and finally, prebiotics + probiotics to rebuild the microbiome.
Recovery remains non-linear, and setbacks are part of the process. Patients can expect periods of improved energy or mood, followed by plateaus or short-lived regressions. Emotions may feel more "alive" but also less buffered. There is often a phase of emotional thaw, where old memories or unresolved stress emerge. The most important factor is that progress is gradual and symptoms are manageable. Each setback is an opportunity to learn and recalibrate, not a sign of failure.
The patient’s sense of agency grows as they begin to notice and interpret their own responses. Trust in the process is built not on relentless progress, but on the ability to pause, recover, and continue. The clinician’s role is to validate these experiences, explain what is happening, and remind the patient that, while difficult, this approach offers the best chance for genuine, lasting recovery.
Experiencing metabolic recovery - what it feels like as your energy systems recover
During collapse, the body is stuck in emergency mode. Glycolysis is inefficient, fatty acid oxidation is blunted, and lactic acid accumulates quickly with even mild exertion. Most energy comes from "burning sugar poorly," which leaves the patient exhausted after trivial effort. Muscles ache, and small exertions can bring on a disproportionate sense of heaviness or even mild acidosis. After activity, recovery is slow. There may be a background sense of internal "sourness," and sleep does little to replenish energy.
As the protocol progresses and the first cracks appear in this rigid metabolic state, changes can be both subtle and disorienting. When cAMP-PKA tone begins to improve and the first traces of mitochondrial support arrive, the patient might notice short bursts of energy - windows where movement feels lighter or less taxing. This is the nervous system and muscle tissue rediscovering how to use glycolysis more efficiently. Instead of every effort being punished by burning muscles and a leaden fatigue, there are moments when exertion is merely tiring, not overwhelming.
Fatty acid oxidation often lags behind. When it begins to recover, it may be heralded by a curious combination of sensations: steadier background energy, reduced need for snacking or sugar, and a less dramatic crash after activity. For some, this comes with a brief resurgence of "keto flu" symptoms - headache, brain fog, mild nausea, or a peculiar sensation of metabolic unease - as the body relearns how to mobilise and process fats. Old symptoms like mild hypoglycaemia or even transient palpitations can flare, but now they respond more quickly to rest or a small snack.
During this metabolic recalibration, patients may also experience sudden swings between energy systems. A good day might be followed by a day of heaviness, as the system "practices" new flexibility. It is normal for the body to default to the old, rigid state during stress, infection, or after a poor night’s sleep. With patience and support, these fluctuations even out. Activity can be sustained for longer, with less muscle soreness or lactic "burn," and post-exertional malaise becomes less severe and shorter in duration.
Sleep also shifts. Early in recovery, sleep may feel light, fractured, or unrefreshing. As mitochondrial and fatty acid pathways revive, sleep deepens, dreams become more vivid, and the feeling upon waking gradually improves. Hunger and satiety cues become clearer. Cravings for sugar or stimulants diminish as the brain and muscles regain access to stored energy.
Throughout, patients should expect this journey to feel unfamiliar. However, the return of metabolic flexibility often means confronting both old symptoms and new sensations. Some will feel bursts of restlessness or drive, as the nervous system recalibrates. Others will notice mood swings or emotional thaw, reflecting not just the lifting of metabolic brakes but the return of a more "awake" brain. These are all signs that the underlying system is no longer stuck, even if the new equilibrium is fragile.
The clinician’s role is to remind patients that each shift - pleasant or uncomfortable - is a signal that the machinery is coming back online. Setbacks are common, and relapses into fatigue or brain fog do not mean the process has failed. Rather, they are cues to adjust pace, optimise rest, and allow for further healing.
Overall, the experience of recovery is one of transition - from a brittle, highly-reactive system to a more robust, flexible network capable of burning both glucose and fat. Progress is not linear, but with patience and appropriate support, the system regains resilience. Each step, even the uncomfortable ones, is a movement toward a more sustainable and adaptable state.
This protocol involves several steps that require multiple tests and a wide range of important supplements. While the expected results are unlikely to be realized without completing all these steps, efforts have been made to simplify them as much as possible. The steps are as follows:
- Collect your data
- (Optional) Pre-protocol support
- Lifestyle changes, plus ongoing transition from sympathetic overdrive -> parasympathetic balance, as the metabolism allows
- Stage 1: Remineralisation, increasing collagen synthesis rates, and performing a controlled initial “die-off” (at least two weeks)
- Stage 2: Enhanced gastrointestinal and mucosal interventions (at least two weeks)
- Stage 3: Stimulate and support a strong immune response while breaking (circulating) biofilms (at least four weeks)
- Optional follow-up
- Ongoing preventative maintenance
"Be thankful for your triggers, for they show where you are not free."
We fully anticipate that individuals exploring this protocol may be highly sensitive to supplements. The reasons for this sensitivity are detailed in the disease model and have been accounted for within the protocol. The sensitivity to supplements and foods is expected to resolve as part of the protocol.
One of the most important lessons learned through this process is that ultimately, whenever a basic, essential nutrient triggers an initial reaction - either good or bad - you need it, although you may also unmask other deficiencies / compensations in the process of correcting one.
That stated, blindly charging your way through barriers is not a sensible way to achieve success, and there is a structured process to follow which makes nutrient repletion much more tolerable.
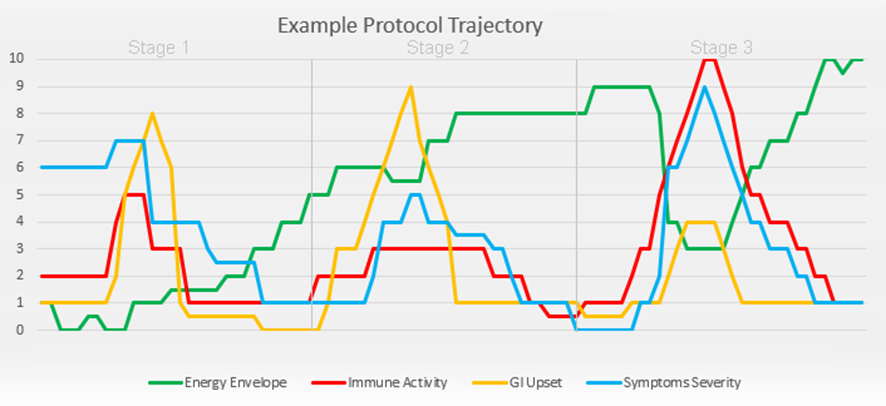
This protocol is designed to stimulate immune activity and may produce a “J-curve” trajectory, meaning you might feel progressively "quite sick" at the beginning of each stage. Increasing energy availability allows for heightened immune activity, which prioritizes energy metabolism toward these goals and can temporarily intensify symptoms. Carefully maintaining levels of electrolytes, copper, zinc, iron, manganese, selenium, glycogen, and B vitamins may help prevent severe symptoms and post-exertional malaise (PEM) or "crashing."
Your individual experience may vary based on factors such as the pace of protocol implementation, the pathogens involved, your initial baseline condition, and the consistency and accuracy of your daily participation. Avoiding or delaying parts of the protocol can hinder progress and potentially lead to unnecessary discomfort. Support is available through our Discord discussion group.
Before beginning, assess your lymphatic system as described in the “2.2.2 Lymphatic Maintenance” section. Note any tissues that have been or continue to be sore, stiff, or inflamed—these areas are expected to flare during increased immune activity and may be adjacent to other infected tissues.
To help reduce expected symptoms when correcting deficiencies and experiencing Herxheimer reactions (microbial die-off effects) due to improved immune activity, a recommended starting sequence has been provided.
The "die-off effect" can cause a range of temporary but highly debilitating symptoms, including headaches, nausea, additional fatigue, dizziness, swollen glands, bloating, gas, constipation or diarrhea, joint or muscle pain, tachycardia, chills, cold hands or feet, itchiness, rashes, sweating, and fever resembling the "disulfiram effect."
A schedule of specific products is available, with vendor website links provided for different regions (see “5. Ordering Products”). These are not affiliate marketing links. With the exception of the Oxalobacter.com
website (which was created out of necessity to address worldwide supply issues for
"Oxalobacter formigenes" probiotics and is not intended as a for-profit
endeavor), there are no financial incentives or benefits from providing links to products or tests. If you encounter supply shortages, please try to find the same product from another vendor or ask for help in the online Discord discussion group.
Deviating from the recommended starting order or substituting products may lead to avoidable and unpleasant symptoms or may simply be ineffective. You can space out the stages further if needed. Despite the extensive list of supplements—aside from one or two items included to make your experience more tolerable—all are necessary. Attempts to create a "lite" version of this protocol by swapping or omitting items have consistently resulted in failure.
Stage 1 focuses on delivering missing minerals and other nutrients to the body, sometimes via non-oral routes, to resolve measurable deficiencies caused by inhibited oral absorption of these micronutrients at levels typically found in foods. While this helps restore normal metabolism, these nutrients are also accessible to the microorganisms inhabiting your body. Therefore, an additional goal of selectivity is required, targeted by a combination of probiotics and antimicrobial interventions. Some of these interventions are included in Stage 1, while others are introduced in Stages 2 and 3.
It is not advisable to take the Stage 1 metabolic support supplements for an extended period without progressing to the parts of the protocol that address microbiome dysbiosis, such as dietary optimisation. Otherwise, you may feel increasingly better at first, but over time this may lead to amplification of existing microbiome issues. Nutrients that benefit your cells also benefit microorganisms that depend on you, and vice versa.
Fulvic acid is used extensively in Stage 3 of the protocol. Due to its potent ability to "liberate" and recirculate metals sequestered during chronic inflammation; it is recommended to test your response to a single drop of Good State Ionic Man (fulvic acid multi-mineral) diluted in a glass of water during Stage 2. Increase the dosage slowly. Fulvic acid is also a potent biofilm breaker. If you experience any unpleasant effects, take a few days to gradually increase from a smaller dose—for example, place a drop in a bottle of water, mix it, and then transfer a drop from this first dilution into another glass of water—until you can consume a standard serving without adverse effects.
If you have nasal inflammation or notice any airway resistance or restriction when breathing, it may be appropriate to perform a nasal microbiome test and investigate for environmental mould issues. Unwanted microorganisms such as Candida, Aspergillus, Streptococcus, Staphylococcus, and Klebsiella species are sometimes found in the nasopharynx. These tests may also indicate the susceptibility of detected strains to interventions like fluconazole, itraconazole, voriconazole, or amoxicillin.
If your levels of magnesium, zinc, molybdenum, selenium, iron, iodine, or calcium are low, you may experience additional symptoms related to aldehyde metabolism insufficiency. These symptoms can be exacerbated by consuming excess alcohol, histamine, polyethylene glycol (PEG), vitamin A, or vitamin B6.
Issues with neurotransmitter metabolism, histamine regulation, and gut function are common and to be expected.
Correcting severe electrolyte deficiencies can temporarily create paradoxical effects, including increased metabolism rates and heart rate. Consuming certain minerals like copper or zinc on an empty stomach can easily induce nausea.
If taurine or magnesium affects your sleep or causes palpitations, tremors, or if you feel worse upon starting them, this may indicate a calcium deficiency. Adding 1–2 grams of elemental calcium per day, along with vitamin D3 and vitamin K2 MK-7, may help correct this. Be aware that addressing a calcium deficiency can initiate the process of oxalate dumping, which is necessary but may cause muscle pain. Low calcium levels may coincide with strontium and phosphorus deficiencies. The tests included in this protocol will help identify these issues. Low strontium levels in hair testing may serve as a proxy indication for calcium deficiency.
Correcting an iodine deficiency is likely to temporarily increase anti-thyroid peroxidase antibodies (anti-TPO) and Thyroid Stimulating Hormone (TSH), enhancing the activity of the sodium-iodide symporter (NIS) while improving levels of triiodothyronine (T3) and thyroxine (T4).
We recognise that the extensive list of individual supplements required for this protocol presents a new challenge. We are collaborating with compounding pharmacies to simplify this process - transforming most of Stage 1 into sublingual lozenges (troches) or DMSO-based multivitamin, and a tub or bag of premixed powder. A DIY powder recipe is also included for those who prefer to mix their own.
Consuming mixed inositols will signal your cells to increase glucose uptake and glycogen synthesis, promoting glycolysis over other energy pathways. Inositol inhibits catalase, which may decrease your capacity to handle oxidative stress during immune activity, necessitating additional antioxidant support. If your liver and muscle glycogen stores are low - which is expected - you may initially feel extremely hungry or experience hypoglycemic symptoms such as dizziness, depression, and extreme fatigue. Consuming up to 500 grams of additional net carbohydrates and water over two to three days to replenish glycogen stores should help you feel significantly better. Glycogen binds with water at a 1:3 ratio, so your total body mass may increase by around 2 kilograms. Note that inositol can be problematic if you are following a ketogenic diet. D-chiro-inositol should be started at approximately 2.5 mg and very slowly increased as tolerated.
(Optional) Pre-protocol support
Remineralisation Will Alter (Restore) Neurotransmitter Homeostasis or "Managing Transitional Neuropsychiatric Symptoms"
It's critical to note that most of the enzymes responsible for synthesising, degrading, or recycling neurotransmitters are B-vitamin dependent, and their active forms, such as FMN, FAD, TPP, P5P, and methylcobalamin, are functionally deficient in the data of people with chronic illness. This is not always due to dietary inadequacy, even relative to general population requirements. The applied data shows this is due to cofactor bottlenecks, impaired enzymatic activation, oxidative degradation, and zinc- / magnesium-dependent enzyme instability.
This is evident, for example, in the metabolism of vitamin B6. As shown in this detailed diagram of B6 metabolism, converting dietary B6 into its active form P5P involves a cascade of steps: alkaline phosphatase (ALP) activity outside the cell, membrane transport, and intracellular phosphorylation via pyridoxal kinase (PK). Each of these steps is dependent on magnesium and zinc, and many are redox-sensitive. Acetaldehyde, chronic inflammation, and low ATP all interfere. It's no surprise, then, that functional P5P levels are low, even when blood levels of pyridoxine or pyridoxal appear normal or highly elevated.
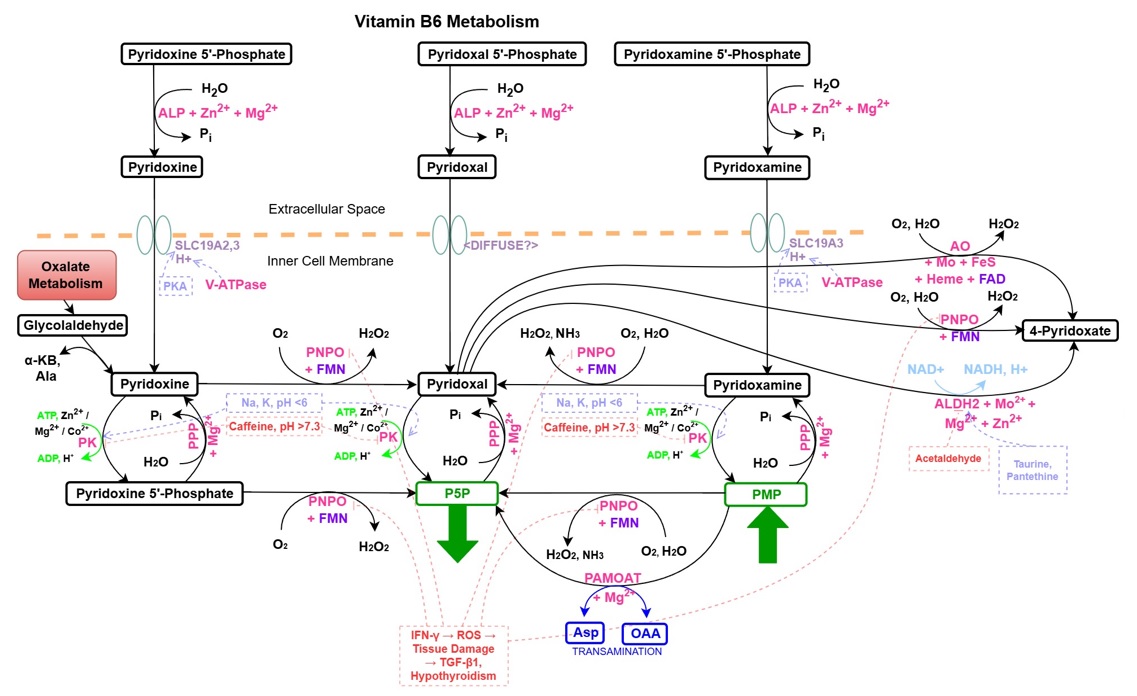
However, this problem isn’t limited to Vitamin B6.
eg. Riboflavin must be converted to FMN and FAD, a process impaired by low ATP, oxidative stress, zinc or magnesium loss. Thyroid synthesis and related minerals, substrates also influence this.

Thiamine must become TPP via thiamine pyrophosphokinase. B12 must be converted to methylcobalamin, a zinc- and glutathione-sensitive step. These are often affected by chronic acetaldehyde, either directly or indirectly.
Acetaldehyde burden affects not only ALDH directly, but also indirectly interferes with zinc-dependent enzymes, magnesium availability, and redox-sensitive pathways throughout this entire cascade. It also stimulates mast cell activation, promoting histamine release, while simultaneously impairing histamine degradation through inhibition of ALDH and depletion of cofactors like P5P and copper. This can disrupt the balance of neurotransmitters by overactivating histamine receptors, and indirectly suppressing dopamine synthesis via H₃-mediated inhibition of tyrosine hydroxylase. It acts as both a primary disruptor and a multiplier of vulnerability in neurotransmitter and cofactor systems.
The result is that small efforts to stimulate or correct neurotransmitter production can trigger paradoxical responses, including overshooting, agitation, anxiety, "brain on fire", insomnia, sedation, getting "stoned" / "high", or what many patients call a “weird” or “off” feeling.
Onboarding
The fix isn’t to push harder, it’s to intervene smarter - a staged approach works better.
For severe cases / people with elevated susceptibility to (neuropsychiatric) symptoms from supplements, etc., a very gentle ramp up with tiny doses of non-methylated B vitamins can be very helpful, before moving to the compounded multi-mineral products. Metabolics (UK) produce a range of liquid B vitamins which are ideal for these purposes, although they don't carry all products and some other vendors are required.
You can find these in the "Onboarding (Severe)" category in product lists below.
A schedule of "essential" products and dosing can be found below, in "Getting started".
Use non-oral routes to bypass known bottlenecks. Transdermal, sublingual, or parenteral delivery helps sidestep transporter saturation, liver metabolism, or dysregulated GI environments. Dissolving nutrients in DMSO is another useful strategy.
P5P in DMSO is one example of an advanced strategy - dissolving P5P in a DMSO solution bypasses multiple upstream steps: it does not rely on ALP, avoids compromised membrane transporters, and skips over PK activation. This makes it ideal in states where P5P is known to be low despite B6 repletion. It may also enter intracellular compartments more efficiently, including mitochondria. The same effect applies to most compounds needing to be absorbed and distributed systemically.
In this context, neurotransmitter restoration is more about kinetics, cofactor availability, and redox context. A patient may be taking all the right nutrients, but if those nutrients are stuck upstream, degraded by peroxynitrite, or unable to bind to their target enzymes due to low zinc, the net effect is failure. Worse, poorly timed repletion can destabilise the system further.
The half-life of each vitamin is frequently overlooked. Dosing vitamins 2-4 times per day is often necessary to achieve sufficient benefit and this is reflected in the schedule.
eg. Vitamins B1, B2, B3, B5, B6, B7/H, B8, B9, B12 and C are taken 2-3x/day, often sublingually.
In the context of restoring severe deficiencies, strategic sequencing matters. B vitamins are powerful, especially in active forms, however they also act as signals in a complex control system. If introduced out of order or in isolation, they may trigger compensatory reactions that mimic toxicity, when in fact they are just unmasking hidden dysfunction.
Many of these mechanisms may also help explain why certain neuropsychiatric conditions appear during chronic illness and how they can act as precursor states to systemic collapse.
ADHD, for instance, is often characterised by signs of noradrenaline and dopamine dysregulation, impaired impulse control, and chronic restlessness, traits which may reflect an early-stage compensation for failing neurotransmitter recycling or low-grade redox and metabolic dysfunction, downstream of chronic endogenous acetaldehyde and opioid synthesis. If these compensations begin to fail, especially under stress, infection, or prolonged nutritional depletion downstream of chronic lactic acid metabolism and mineral transporter alterations, the system may tip into a more energy-conserving, downregulated state, as observed in ME/CFS, long COVID, post vaccination syndrome, etc.
Bipolar disorder may reflect a different kind of instability, one in which neurotransmitter tone swings between overcompensation and collapse, and this too may be compounded by aldehyde load, especially acetaldehyde, which inhibits ALDH enzymes responsible for clearing dopamine breakdown products like DOPAL.
Dietary contributions to acetaldehyde burden, such as excessive intake of alcohol, sugar, or fermentable carbohydrates, can further amplify this inhibition by fuelling microbial overgrowth and endogenous ethanol production in the gut. When ALDH function is compromised, neurotoxic intermediates accumulate, further impairing redox balance and downstream dopamine synthesis. Over time, this may shift the system toward an oscillatory or collapsing state, where any attempt to stabilise mood or energy is undermined by bottlenecks in detoxification and neurotransmitter recycling These cycles could, in part, emerge from fluctuating availability of critical cofactors like P5P, B2, or SAMe, or episodic redox crashes that disrupt normal mood-regulating feedback.
However, the protocol also spans over 250 printable pages - so it's also completely understandable if you find yourself feeling a bit overwhelmed by the volume of new information needing to be absorbed.. likely while still battling brain fog and energy envelope issues, chronic feelings of fight/flight and other challenges.
Removing some or all of these debilitating issues should help improve the absorption and retention of new information. The focus of this section is to order and integrate JUST the essential items needed to get started on stabilising the key metabolic pathways. You can integrate them using the order described below, also noted in the daily schedules / run-sheets provided at the end of this section, along with a product ordering spreadsheet.
Ideally after sending off your baseline tests, you may help stabilise critical parts of the metabolism and help avoid unwanted MCAS + other symptoms by;
Notes:
i) Failure to maintain lymphatic flow can result in compartment-specific pressure buildup, eg. intracranial pressure.
ii) For severe patients, this may need to be actioned by carers and/or professionals. Sensitivity to touch may initially prevent performing this necessary step, however it should be actioned as soon as possible.
Notes:
i) Eat strategically to ensure glycogen stores are being appropriately supported - this may easily be >150-180g of net carbohydrates / day, as insulin sensitivity / glycogen synthesis improves - absorbed over 3-6 meals / snacks. Carbohydrate needs reflect (immune) activity levels and other factors. A number of the supplements included below will help glycogen homeostasis.
ii) The initial goal is a low-inflammatory, low-histamine, low-oxalate diet - ideally, one that avoids triggering foods - however this doesn't need to be "perfect", just "good enough". This will later expand to include a wide array of plants, their helpful polyphenols, microbiome nourishing fibres / starches and numerous other useful compounds, whilst accompanying targeted, staged probiotics that focus on butyrate production and epithelial integrity, before repopulating lactobacillus, bifidobacterium, oxalobacter and other helpful species.
4. Stabilise the redox and mineral terrain. This includes VERY SLOWLY introducing :
a) electrolytes (see 4.1 Electrolytes), taken slowly over the day, by making a daily / weekly recipe of
specific electrolytes and amino acids to put in a 500ml drink bottle
and slowly sip / pour a "shot" into a glass, top up with water and drink
between meals (see 4.3 DIY "sipper / shots").
You can start at eg. 1/8 daily doses and slowly increase.
The daily targets for each electrolyte compound used are (these are also listed in the daily schedules at the end of this page). These allow for minimal dietary intakes and can be further adjusted around consistent dietary norms, using this calculator tool:
Magnesium Aspartate - 5.5g total powder (440mg elemental magnesium) / day.
Monocalcium Phosphate - 5g total powder (850mg elemental calcium & 1300mg elemental phosphorous) / day.
Potassium Citrate - 13g total powder (4940mg elemental potassium) / day.
Sodium Bicarbonate - 5g total powder (1350mg elemental sodium & 3650mg bicarbonate) / day.
Sodium Chloride - 5-7g total powder (2730mg elemental sodium & 4270mg chloride) / day.
Resveratrol can be slowly added here (taken separately) 3x/day - initially starting at 50mg and increasing to 500mg per dose, to help protect against additional lactic acid being created by unblocking bottlenecks in glycolysis (correcting phosphate, magnesium, etc) while the TCA cycle is less efficient.
Liberally applying the magnesium gel after showering, can be highly effective for magnesium absorption and is included in the schedule.
Notes:
i) Consuming too much at once may cause diarrhoea, headaches, nausea, water retention and/or rapid urination.
ii) Calcium and to a lesser extent, potassium may temporarily
increase adreneric / glutaminergic sensitivity and need to be increased
more slowly than others. Calcium
sensitivity needs to be tested and managed carefully. Adrenergic, dopaminergic and related auto-antibodies predict sensitivity and delay calcium repletion. Sodium phosphate can be used as an alternate phosphate source during careful calcium titration. (see 4.1 Electrolytes)
iii) Starting magnesium and/or phosphate can improve glucose uptake and glycogen synthesis. Experiencing symptoms that resemble hypoglycaemic events or diabetic "hangry" mood alterations may indicate more dietary carbohydrates are needed.
iv) This recipe can also be combined with eg. green or other tea, lemon juice, lime juice, acai, berry, etc for flavour.
v) Shake before each use.
b) antioxidants and mitochondrial cofactors (Vitamin C, Vitamin E, R-ALA, CoQ10, GSH donors like NAC), taken 2-3x/day.
Notes:
i) These may need TINY doses, initially, eg. 50mg of Vitamin C, NAC and CoQ10. Introduce these individually.
ii) Vitamin E and R-ALA are normally less sensitive. R-ALA may increase insulin sensitivity.
c) (usually less slowly) L-carnitine / acetyl L-carnitine, creatine (for fatty acid transport and ATP-PC pathway), uridine monophosphate (sublingually - ramping up from 10, to typically 50-100mg, 2x/day) and similar slowly ramp up of D-ribose, starting at 500mg, to 10g, added to the daily DIY "sipper/shot" recipe. SLOWLY titrate a morning sublingual dose of inosine from 50-100mg (weeks 1-2 or until ready for an immune activity phase) to 500mg.
Notes:
i) Expect insulin sensitivity and glycogen synthesis to increase with uridine, D-ribose and inosine - be prepared to increase intakes of carbohydrates to facilitate glycogen synthesis and potentially sodium + other electrolytes, towards their daily targets.
ii) Inosine is also an immune stimulant, and may trigger some initial immune activity - keep the dose low, eg. 50-100mg for the first 1-2 weeks, or until metabolically stable enough to sustain a phase of initial immune activity.
d) Adding mineral cofactors like zinc, copper, iron, manganese, selenium, iodine, lithium, rubidium, cobalt, boron, and molybdenum, etc. This helps balance the neurotransmitter synthesis pathway (and precursors), lowers the burden on ALDH and MAO pathways and reduces oxidative stress, allowing safer processing of neurotransmitter metabolites. (see 2.3.2 Remineralisation).
Notes:
i) Many of the minerals require non-standard routes for absorption, eg. sublingual, liposomal, DMSO-carrier.
ii) Remineralisation will be severely limited if acidaemia / acidosis is still present.
e) Introducing vitamins B1 and B2 in active or near-active forms - such as TPP / cocarboxylase and FMN / R5P. These support mitochondrial redox balance, glycolysis, and the Pentose Phosphate Pathway. Depending on the severity of dysbiosis / acetaldehyde burden, the total daily B1 dosing can range from 50-600mg of the active form, cocarboxylase (not to be confused with eg. thiamine or thiamine HCL which would require much higher doses), starting from a low dose.
Notes:
i) Compounded nutrients are available (see 4.2 Compounded nutrients) and replace a wide range of individual supplements. The compounded nutrients are potent, therefore starting at eg. 1/8th doses,
may be helpful to soften / slow the metabolic shift when restoring
severe deficiencies.
ii) B vitamin titration options for patients with severe
neuropsychiatric sensitivity are also discussed.
iii) Additional B1, in any form, can be added for further
acetaldehyde adduct-forming and detoxification support, later - noting the impact of rapid removal of acetaldehyde -> endogenous morphine. (see 2.3.4 Rapid withdrawal, hypo/hypermetabolism)
iv) Adding B1 can increase B9 transporter activity and SAMe availability,
allowing some adrenergic signalling increase unless B2 and NAD+ are
restored in balance - start slowly.
f) Slowly layer in vitamins B5, B6 (as P5P), biotin, D-chiro inositol, B9 and B12 (as methylcobalamin or
hydroxocobalamin) only after upstream redox stress is under better control.
Notes:
i) B1, B9 and B12 can increase methylation -> SAMe availability, unblocking epinephrine synthesis at PNMT and also COMT activity, leading to hyper-adrenergic signalling if TOO MUCH is introduced quickly, ie. without sufficient B2 for MAO and NAD+ (and redox) for ALDH.
ii) In
the context of unresolved aldehyde or monoamine overload, these can also be
disruptive (unless P5P is eg. dissolved in DMSO, bypassing impaired alkaline phosphatase (ALP) and pyridoxal kinase (PK) steps) and BH4 synthesis (dietary queuine - see "Vitamin Q deficiency").
NB. Reducing acetaldehyde and/or restoring NAD+:NADH status corrects a wide array of impaired metabolism, including the pathway issue which promotes endogenous morphine synthesis.
Stay keenly observant for rapid withdrawal symptoms and manage them proactively.
Then;
g) Introducing NAD+ pool support (apigenin - P38
inhibitor), NAD+:NADH redox support (0.05-0.3mg of methylene blue, once per day), and
Notes:
i) Start at 0.05mg (50mcg) of methylene blue per day and slowly increase every 2-3 days until ANY metabolic shift is observed. Hold at that dose and look to decrease towards 50mcg, when appropriate.
ii) "MORE IS NOT MORE." THE MITOCHONDRIAL SUPPORTING EFFECT OF METHYLENE BLUE IS LOST AT HIGHER DOSE RANGES.
iii) Expect and watch for alcohol / opioid withdrawal symptoms. Manage them proactively.
h) Adding active vitamin B3, as sublingual NAD+ / NADH (NOT precursors - niacin, nicotinamide / niacinamide, nicotinamide riboside / mononucleotide) at 5-10mg doses, 2x/day and increase to 20-40mg 2x/day.
Notes:
i) Expect and watch for alcohol / opioid withdrawal symptoms. Manage them proactively. (see 2.3.4 Rapid withdrawal, hypo / hyper metabolism)
6. Start working on identifying and addressing any/all other influences affecting histamine and/or sympathetic overdrive (see 2.2.6 Cortisol, limbic system, glycogen and IFN-γ).
Notes:
i) Unrestricted, deep nasal breathing without localised inflammation is a basic requirement for parasympathetic signalling (see also 2.2.3 Living without chronic dysbiosis - Nasopharynx).
"Starter" daily schedule / run-sheet
Once you have sufficiently stabilised, you can continue onboarding and progressing through Stages 1, 2 and 3. The daily schedule options for the full protocol can be found in 2.3 Daily supplement schedule.
However, to keep things more manageable for now - you can also download and print a simpler / more focused daily "starter" schedule / run-sheet - and there are two versions available:
You can choose this version (opens on a new page) if you intend on using the compounded nutrients,
OR
you can choose this version (opens on a new page) if you intend on using separate store-bought supplements.
"Starter" product ordering links
If you are already committed to completing the whole protocol, the product ordering links for the primary pathway of the full protocol can be found in 5 Ordering products. However, you can also download a time-and-money saving spreadsheet of the starter items ONLY, before committing to the whole process:
For starter product ordering, you can simply choose your shipping region from the drop-down box and click on the Excel or CSV icon to download a spreadsheet of some starter items, with product ordering links and relevant information for preparation of time/effort-saving weekly recipes. This particular table is too complex to fit onto a webpage and easily manipulate, however works well in eg. Excel or Google Sheets, etc.
This protocol begins with a data collection process that helps you to identify specific deficiencies and microbial influences relevant to your metabolism.
There are multiple tests required to collect this data and the protocol is unlikely to succeed without them.
Testing blood is a helpful way to understand specific aspects of immune activity and metabolism. Minimally, it’s useful to have markers for blood group (needed for Oligoscan), red blood cell (RBC) and white blood cell (WBC) counts, comprehensive metabolic panel (CMP) and lipids, LDH isoenzymes, iron studies (iron, transferrin, transferrin saturation %, ferritin), vitamin B6 and vitamin D (inactive form). Your doctor is usually the best person to assist you with these, however private lab services are also available in many countries, should these be helpful.
USA
Australia
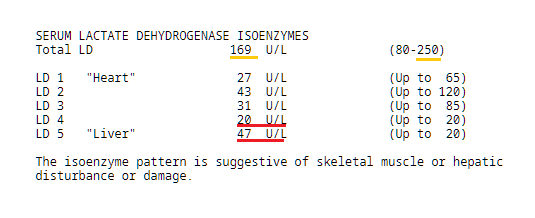
Lactate dehydrogenase (LDH) isoenzymes
Lactate dehydrogenase (LDH) is an enzyme primarily involved in converting pyruvate to lactate (and vice versa). It has five isoenzymes (LDH-1 to LDH-5), each consisting of different combinations of two subunits: H (heart) and M (muscle). Further, there are individual LDH isoforms - LDH-A/B/C which make up these isoenzymes. These isoforms have specific roles / functions. LDH is also a metalloenzyme, affected by zinc status and NAD+:NADH ratio. LDH isoenzymes are distributed across various tissues based on their metabolic needs.
The terms "H" (heart) and "M" (muscle) subunits were historically named based on the tissues where these subunits were first observed in high concentrations. The H (heart) subunit was first identified in cardiac tissue, which relies on aerobic metabolism. The M (muscle) subunit was discovered in skeletal muscle, which often utilizes anaerobic glycolysis, especially during high activity.
This test allows you to see if an elevation of a specific isoenzyme or pattern of elevations is present, further suggesting if a particular tissue is experiencing energy metabolism dysregulation, and/or upstream influences affecting energy metabolism.
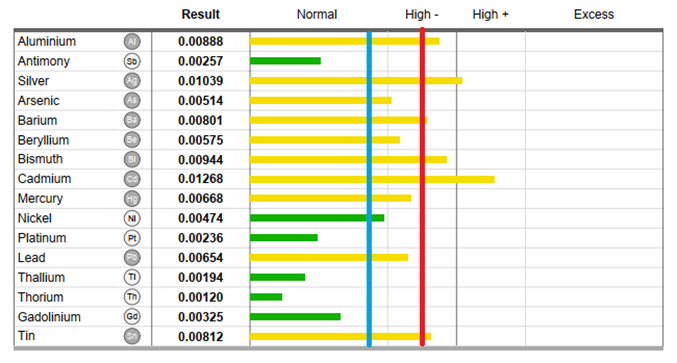
eg. If LDH-4 and LDH-5 (which contain more M subunits, characteristic of anaerobic glycolysis) are elevated, it can be indicative of reduced oxygen availability or prolyl hydroxylase inhibition for other reasons (oxidative stress, low Fe/Si, low Zn, low alpha-ketoglutarate, elevated succinate). These isoenzymes are more prevalent in tissues that rely on anaerobic metabolism, such as skeletal muscle and liver, and their elevation suggests a shift towards lactate production due to reduced oxygen, a common feature of hypoxic conditions and / or various issues which inhibit prolyl hydroxylase activity (see Figure 1).
Standard LDH testing only measures TOTAL LDH. The individual isoenzymes are combined into a single figure, easily obscuring any anomalies in an individual tissue. This makes standard LDH testing highly unreliable and easily provides another false negative result, upsetting diagnostics efforts by clinicians.
eg.
Use at least one of the following two testing methods (hair mineral testing no longer supported for measuring most deficiencies due to unavoidable limitations in the methodology).
There are limitations to any testing methodology and potential ways for errors in sampling to occur. Some of these problems can be identified and avoided. Others can relate to eg. unpredictable sample transport delays.
To identify potential data errors, best practice is to triangulate and validate markers, deficiencies and issues from multiple data sources, eg. direct measurements of minerals and patterns in metabolites of enzymatic reactions which rely on these minerals.
White blood cells (WBC)
Currently, there are 3 competing laboratories which specialise in measuring the intracellular nutrient status inside WBCs - Cell Science Systems CMA (part of their CNA offering), SpectraCell Micronutrients and Vibrant America Micronutrients.
WBCs are used as a proxy to infer the nutrient status of other cell types, eg. brain, muscle, liver, etc. This data is very different to what is reported in serum (data sourced from outside the cells and any/all related mineral transporter function) or red blood cells, which lack mitochondria and therefore have very different metabolism. Vibrant America Micronutrients test does an excellent job of highlighting this issue in their report. It's frankly astonishing that serum testing is still considered the "gold standard" by public health systems, in light of these issues. However, this also highlights why chronic diseases have been difficult to research and solve.
Although all of these laboratories measure WBC nutrients, each of these tests has a different methodology and different array of included markers. Therefore, the advantages and disadvantages for each have been carefully considered. Primarily due to the expansive array of markers more closely matching our requirements, Cell Science Systems CMA is used by this protocol. However, there are limitations to accommodate. In a more perfect world, we would have a test that uses the SpectraCell or Vibrant America methodology, with the CMA scope of markers.
By checking OAT results before ordering the CMA test, you can help identify if you have the hypoxia / acidemia patterns and are likely to have issues:
1. If you see elevated lactic acid (22), relative to pyruvic acid (23), elevated oxalic acid (21), and/or low phosphorus (76), this pattern is suggestive of excessive anaerobic glycolysis / lactic acid metabolism, metabolic acidemia and renal phosphate dumping.
2. A relative drop from citric acid (29) to aconitic acid (28), with similarly low 2-oxoglutaric acid (27) may indicate severe deficiency of magnesium.
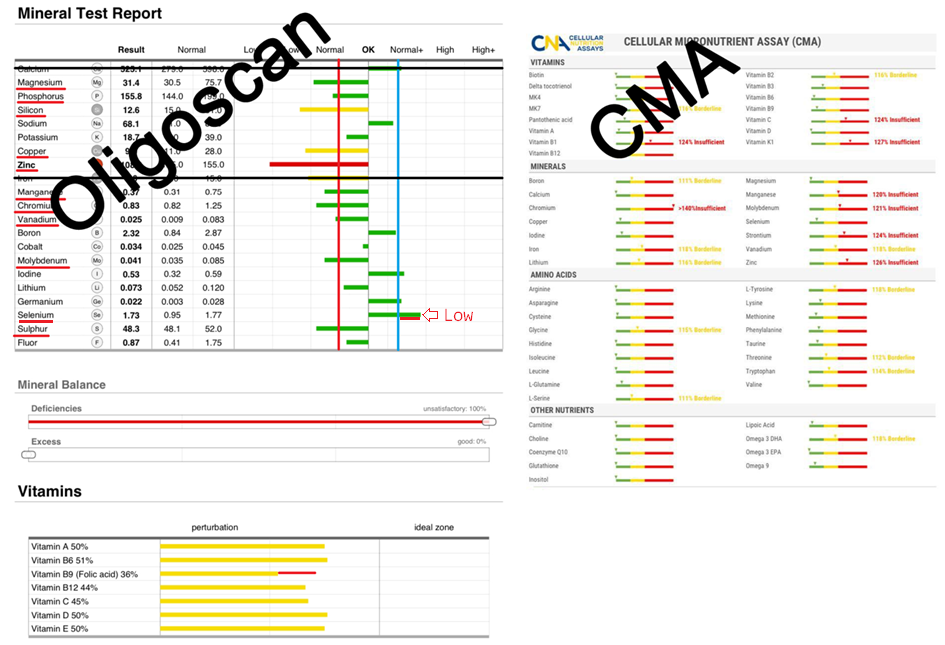
The Getting started section may be helpful in stabilsing the baseline metabolism enough to perform the CMA test without issues. Alternatively, you could use the Oligoscan test discussed below, without this limitation.
However, if you receive a CMA report which is verifiably affected by this issue, you may be able to partially salvage the results by reinterpreting the markers as follows:
1. Any marker not all the way to the left, yet still green is re-interpreted as yellow.
2. Any marker that is yellow is re-interpreted as red.
3. Any marker that is red is re-interpreted as severely deficient.
Advantages:
1. Directly actionable data from an accredited laboratory.
2. Significant array of markers included.
3. Data is considered a snapshot of "current status", without any lag.
4. Blood sample can be collected at home, using a mobile phlebotomist.
Limitations:
1. 8–12 hours fasting is required.
2. Does not include fluorine, sulphur, silicon, various toxic metals, and some of the electrolytes – phosphorus, sodium and potassium
3. Does not indicate excess nutrient data, although this hasn't been a concern.
4. Transport of the sample needs to be rapid, to accommodate eg. cytokine half-life and nutrient transporter behaviour in the cellular membrane, otherwise report sensitivity can be lost. For non-US citizens, an express FedEx courier service is supplied by the laboratory (with an additional cost), along with any import/export clearance paperwork needed for getting blood samples through border security.
5. Sensitivity in the reporting appears to be significantly impacted by hypoxia, phosphate, sulphur and other deficiencies.
6. Intracellular iron status does not capture systemic iron status data, as 75% of iron is circulating in RBC and serum. A separate test is required.
This comprehensive test is available internationally from a US laboratory. The test normally costs USD$239 - 264, plus express FedEx shipping (usually quoted / invoiced separately, shortly after purchase) and any phlebotomist costs.
Ordering: (International, via USA)
Low iodine may be used to infer high fluorine.
Phosphorus data from the Organic Acids Test (OAT) can infer phosphorus status, although there are some differences, being urine / excretory data.
The protocol uses daily targets for electrolytes, however you won’t have an understanding of the baselines for these markers.
Skin
Research suggests that an Oligoscan, So/Check or Zell-Check report can provide an approximation of your ACTUAL mineral status, using the skin of your hand as a data source. Note that “OligoLab” / “OligoHealth” / “Scantest” branded reports are currently not supported. This is normally an in-clinic test and a local practitioner will be required.Your blood type, age, height and weight affect the sample calibration used to generate this report, so this information will be requested when you visit a clinic. Any inaccuracies can dramatically alter your results.
NEW: An Oligoscan report analysis tool can be found here.
While not happy with the level of published evidence currently supporting this emerging methodology, our testing showed a clear pattern of deficiencies in ME/CFS, Long Covid and Post Vaccine Syndrome, with minor variability, which was not observed in controls.
Follow up Oligoscan reports have also matched supplements taken and previous results. The array of elemental markers collected is almost the same as the Doctors Data HTMA reports, however it also includes silicon and usually fluorine. Unfortunately, it does not show rubidium or strontium markers.
1. As over 75% of systemic iron is circulating, Oligoscan / skin data for iron will be an unreliable proxy for systemic levels – blood tests for serum iron studies (iron, transferrin, tsat% and ferritin) would be needed via your doctor or private lab testing.
Low manganese may also provide a hint for low iron, unless IV iron has recently been administered.
2. Calcium markers in skin data will be similarly unreliable – 99% of calcium is stored in skeletal tissue. This also makes serum calcium insensitive. As strontium and calcium can potentially substitute for each other in biological processes, using the “strontium” marker from the hair test as a proxy to indicate systemic calcium may be possible, but needs further study. Tremors and/or heart palpitations, especially in response to taurine or magnesium could indicate low calcium, also. Low phosphorus may indicate low calcium.
3. Copper and zinc appear to be over-estimated in some cases.
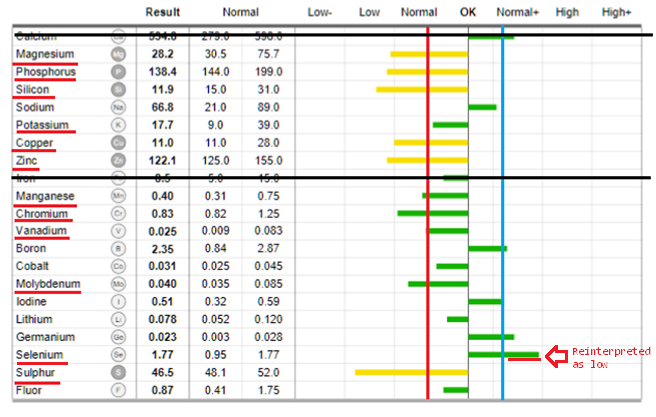
4. Due to an unusual quirk in methodology / reporting, highly elevated minerals need to be re-interpreted as highly deficient.
5. Highly elevated zinc in skin tissue may also indicate low protein / histidine intake and mask an actual zinc deficiency.
Oligoscan and CMA results are not known to be directly affected by the inflammatory cascade, meaning that these reports provide an actionable set of objective markers to use when choosing most mineral supplements to address deficiencies. (HTMA data can be referenced to help supplementation planning for rubidium and strontium, also inferring calcium).
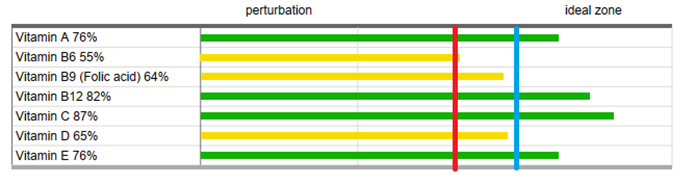
For more information about the effects of specific mineral deficiencies, see the “Rationale for protocol inclusions and general notes” section. The Oligoscan and SO/Check reports include a number of vitamin markers, which appear to track relatively well with other data. A good general target for these is to exceed 55%.
You can search for your nearest provider using our "Find an Oligoscan Practitioner" tool.
If you have a good (or bad) experience with an Oligoscan practitioner, please share details with our community Discord group in the #oligoscan-providers channel.
For Oligoscan, you can also find local practitioners here: https://www.theoligoscan.com/nearest-provider
or try using Google and run individual searches for each company / technology and your suburb (4 separate searches, rather than 1):
eg.
Oligoscan | Oligocheck | So-Check | ZellCheck <your suburb>
Broadly speaking, Oligocheck, So-Check and ZellCheck are more commonly found in and around Europe. Oligoscan is more commonly found in USA, Australia and UK.
Hair minerals (deprecated / limited use)
Research suggests that a Hair Toxin Mineral Analysis (HTMA) may provide an approximation of your functional mineral status, averaged over the period of follicle growth, sampled adjacent to the transporter alterations from inflammation – where circulating minerals can be sequestered inside various brain, liver and kidney cells and consequently low in other cells. It cannot accurately report on the intracellular levels or systemic levels, as sequestered minerals are not shown in this excretory data.
The results obtained from the HTMA data may be used to infer averaged intracellular mineral availability, downstream of any chronic inflammation, for the period of time in which the hair follicles grew, in a similar way to read HbA1C for glucose metabolism. This mechanism is largely relevant to the eleven elements transported by DMT-1 and ferroportin.
A list of vendors offering a compatible list of markers and reference ranges is provided below. Doctors Data and other compatible laboratories
| US | https://www.walkinlab.com/products/view/dd-hair-elements-profile-doctors-data (not available in NY/ NYC and other areas.) |
| AU | https://www.toxno.com.au/articles/heavy-metals/hair-tissue-mineral-analysis-hma-or-htma-in-australia/ (can manually add rubidium) |
| EU / UK | https://regeneruslabs.com/products/hair-toxic-essential-elements-1 |
| EU | https://www.biocoherence.eu/en/shop/htma/ (doesn't include rubidium) |
| EU | https://www.lifelinediag.eu/en/product/eha-standard-en/#products (doesn't include rubidium) |
| NZ | https://www.houseofhealth.co.nz/product/hair-toxic-mineral-analysis/ |
| PL | https://analizawlosa.com.pl/produkt/analiza-wlosa/ |
| UK / some EU | https://www.lauristonlabs.co.uk/product/hair-elements-doctors-data/ |
- Ignore any conflicting vendor-specific instructions.
- The hair needs to be clean, well-rinsed, dry, untreated and uncoloured. Unwashed hair may provide false (elevated) data for sodium and potassium, from dried sweat. Use gloves.
- Select suitable areas of sideburn, scalp and/or neck hair. If the hair is longer than 2.5cm / 1", first trim the sample area to this maximum length with clean stainless steel scissors. By using shorter hair, the report data relates to a more recent period of time.
- Cut the (remaining) hair to be sampled as close to the skin as possible. Do not use clippers or an electric razor – metal contamination from tungsten blades may occur. Collect at least two heaped tablespoons worth of hair, or approximately 250mg, or the sample may be rejected.
- Place the hair sample in the sample kit envelope provided, or in a clean, clearly labelled envelope or sachet. Whilst Trace Elements Inc says not to use resealable plastic bags as apparently hair “sweats” and the sample may be rejected, whereas Doctors Data supplies plastic bags in their kit.
A Mosaic Diagnostics (Mosaic DX, formerly Great Plains) Organic Acids Test (OAT) is a comprehensive report on urine metabolites.
While there are various OAT vendors, eg. Genova Diagnostics, Vibrant, Nutripath, etc., the preferred vendor for this protocol is Mosaic DX, for reasons of reliability, results consistency and marker inclusion.
This test is available through local vendors, or these websites:
International - https://mosaicdxinternational.com/products/mx-organic-acids-test-oat
US -
1) https://www.integrativepsychiatry.net/shop/the-great-plains-laboratory/urine-organic-acids-test/
2) https://empowerednutrition.health/store/Mosaic-Diagnostics-Organic-Acid-Test-p523785023/ (US only)
UK - https://smartnutrition.co.uk/shop/great-plains-oat-organic-acids-test/
UK/EU - https://app.omnos.me/shop/tests/oat-organic-acid-test (needs practitioner)
EU - https://nordiclabs.com/EDetail.aspx?id=2878 (needs practitioner)
AU - via a RN Labs registered practitioner
NZ - https://store.stephenroigard.com/products/organic-acids-test
Note: if there is a pattern of “left shift” or “suspiciously
low” microbial markers on page 1 of the OAT results, it’s possible the
sample has thawed in transit and the integrity compromised, AND/OR the concentration of the sample was out of range (hydration levels). You may need
to repeat the test.
For best results a very short shipping time is
needed and creatinine levels (marker 77) should ideally be between 80-180 mg/dL.
Mosiac DX automatically scale the report markers against the creatinine levels, which can induce a false LEFT-shift with very high concentrations and RIGHT-shift with very low-concentrations. Overall, it's something I think the lab could improve on.
In addition to allowing interpretation of metabolic impairment from the patterns observed in these markers, page 1 of the report shows various markers for microbial interference. The remaining pages show your metabolic impairments from infection and malnutrition. Elevation of yeast, bacterial and fungal metabolites in OAT results have been seen consistently in our collected data, with matching symptoms. A further MycoTOX test may provide further clarity on species and expected metabolic impairments, if required.
Earlier example manual interpretations of these reports can also be found on our Discord online discussion group.
A basic OAT interpretation guide for the purposes of supplement selection can be found in 4 Calculating supplement doses.
Mosaic DX TOXDetect (optional, recommended)
Mosaic DX also provides another urine metabolites test called "TOXDetect Profile", which allows you to quantify the burden of various toxins. Of particular note, 2-Hydroxyethyl Mercapturic Acid (HEMA) in urine appears to be a useful indicator for acetaldehyde, either from exogenous alcohol consumption or fermentation syndrome. However, it is confounded by ethylene oxide and PVC. The metabolism also requires sufficient glutathione for HEMA to be produced. A more direct way to quantify this in urine may be available in the near future.
This test is a little more expensive than the OAT, however can be helpful in monitoring microbiome remediation progress and/or hidden environmental toxins.
This test is available through local vendors, or these websites:
AU - https://www.australianbiologics.com.au/pages/mosaic-diagnostics-test-range
INTL - https://mosaicdxinternational.com/products/toxdetect-profile
NZ - https://store.stephenroigard.com/products/toxic-non-metal-chemical-profile
UK/EU - https://smartnutrition.co.uk/shop/toxdetect-environmental-toxins/
US -
1) https://www.rupahealth.com/lab-tests/mosaic-diagnostics-organic-acids-oat
2) https://mylabsforlife.com/lab-test/toxdetect-profile-urine/
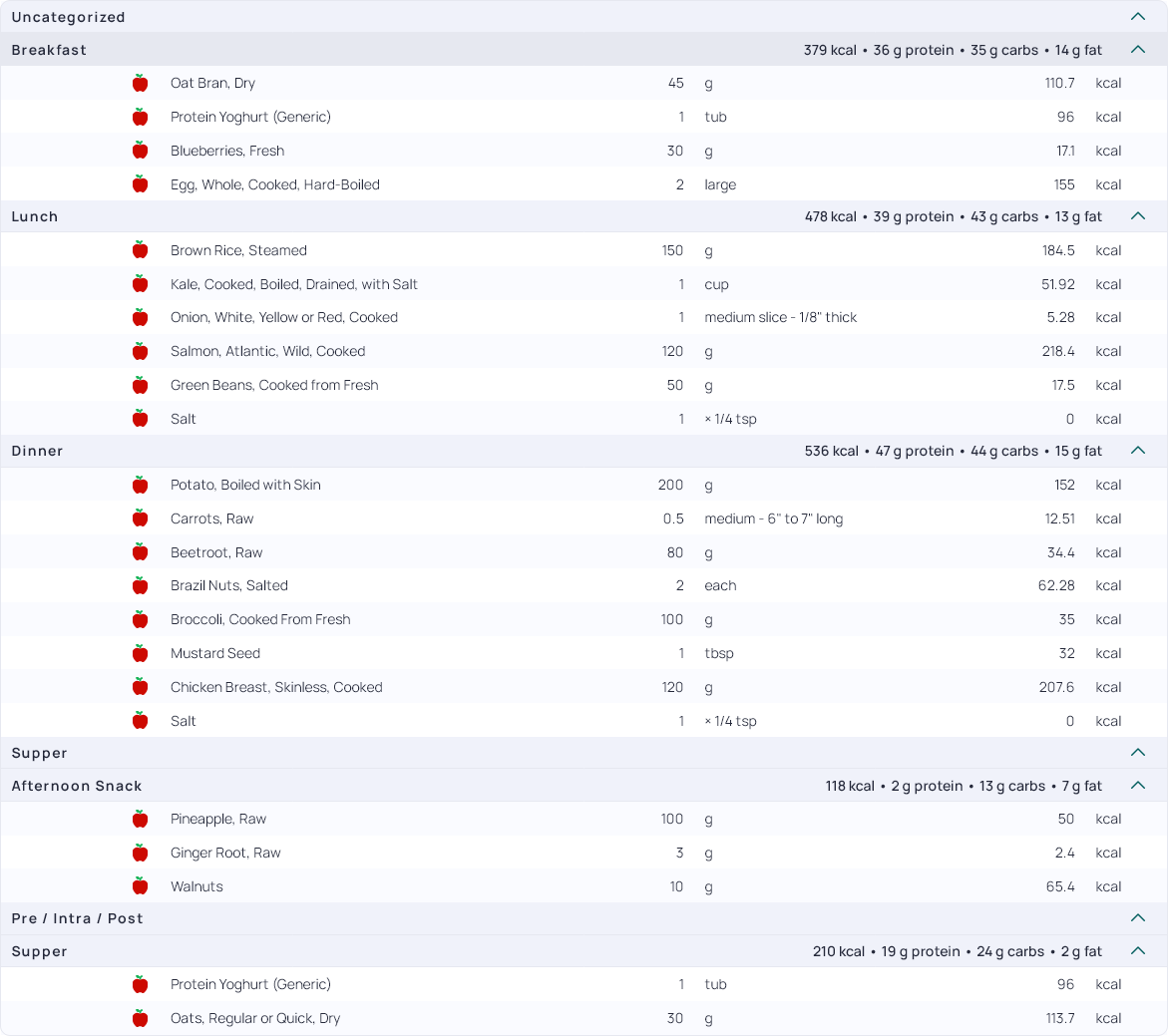
Cronometer (https://cronometer.com) is a freemium online app which can visualise the performance of your current eating strategy / habits / restrictions and allow you to make positive changes. It has a mobile app for data collection and basic reporting. Using a desktop / laptop allows access to richer reporting options and diary view.
Logging at least two days of eating in Cronometer would be very helpful for identifying problems and also help you rebuild / restore your relationship with food, especially as any sensitivities are reduced / resolved over the duration of the protocol. (see “2.2.1 Diet”)
People usually find this process eye-opening.
When selecting food items to enter into the virtual diary, choosing NCCDB or USDA listed food items will provide more micronutrient data. CRDB (user-entered, moderated entries) only contain information displayed on the product labels rather than laboratory identified data.
An example day of eating, with nutritional report:


Dysbiosis and biofilms in the various microbiomes sits at the root of this disease model. Given the implications and progression described in the disease model,
reviewing your medical history, from early childhood forward would be
suggested. A common progression would be an early childhood infection /
biofilm formation in the ears/nose/throat/sinuses that progresses to the
gut (and sometimes lungs), before translocating to sex organs and
urinary tract. Skin microbiome dysbiosis - eczema, acne, dandruff,
fungal nails, etc is also common.
Gut microbiome
Certain gut microbiome tests are useful in getting a rough understanding of the species present in your GI tract (with a focus on the large intestine), along with the metabolites they consume / produce and if any of these are toxic / relevant to your metabolic alterations. Currently there is no single "perfect" microbiome test available. There are a range of tests with strengths and weaknesses. For upper GI data, endoscopic biopsy / aspirate is currently the method-of-choice. Safer, easier and non-invasive methods for collecting upper GI data are desperately needed.
As the stool specimens are not homogenised, very different counts of species can be obtained from different parts of the same specimen. False negatives are common. This can create confusion for anyone who is used to interpreting various reports at face value. Any species counts need to be interpreted with low confidence.
However, the “overall trends” of species diversity and overgrowth can be useful in making decisions around changes to eating habits, supplements and other interventions, for example, consuming bismuth compounds and / or codonopsis / Dang Shen tea for inhibiting sulphur reducing bacteria and promoting bifidobacteria, or taking Akkermansia probiotics and/or pomegranate, if low or missing, along with a supportive diet.
Biomesight
For diversity / abundance testing and recommendations around dietary changes, Biomesight provide some useful reports and importantly, allows record-level data export to CSV for further detailed analysis, which can be used with the information here to make decisions around interventions. NB. fungal species are not reported.
Our Biomesight interpretation tool can be found here: https://bornfree.life/learn/biomesight-tool/
Biomesight are offering a discounted test, thanks to our ongoing collaboration with Remission Biome:
https://shop.biomesight.com/collections/frontpage/products/gut-microbiome-test-snapshot
(Use discount code RemissionBiome for 50% off)
GI-MAP
For enhanced pathogen testing, also including parasites, along with reporting on GI related markers, a GI-MAP report provides more information, however the report lacks the detailed species diversity information provided by eg. Biomesight.
USA vendors:
https://www.dhalab.com/shop/gi-map-gi-microbial-assay-plus/
https://labtestshop.com/tests/gi-map-stool-test/
AU vendors:
https://healthandharmony.net.au/shop/gi-map-test-kit-gut-microbiome-stool-sample
https://elementalhealthandnutrition.com.au/product/gi-map-diagnostic-solutions/
UK, EU vendors:
https://smartnutrition.co.uk/shop/comprehensive-stool-test-gi-map-pathogen-plus-uk-and-europe-igimap/
https://www.ibsclinics.co.uk/product/gi-map/
https://ifu-wolfhagen.de/shop/stuhl-test/stuhl-und-verdauungsanalyse-pilze-gr-parasitologie-bakterien-bauchspeicheldruese-entzuendungsparameter/
IN vendors:
https://www.ithrive.shop/products/gi-map-stool-analysis-offered-by-diagnostic-solution-laboratory-us?variant=44135044612310
Other – sinuses, oral, lung, urinary tract and sex organ microbiome
If you have a known or suspected infection in any mucosal tissue, then combining qPCR and Next Generation Sequencing (NGS) 16S methodology can help identify the species present and help with decision-making processes around remediation. Reviewing your entire medical history since birth and highlighting / testing tissues with recurring issues would be highly appropriate.
They normally supply a "Level 1" report (targeted qPCR), followed by a "Level 2" report (NGS), a few days later. It's common that the Level 1 report results will be less than helpful.
MicrogenDX offer a range of different testing and reports, for different tissues. These are available to US, EU and international customers.
USA / International:
https://microgendx.com/patients/microgendx-patient-test-service-dm-intl
EU:
https://microgendx.eu/products
Limitations:
1. Does not show Lyme species.
Circulating microorganisms - tick-borne, systemic infections
As anyone who has spent time around Lyme disease and tick-borne infections will tell you, getting good data on circulating and intracellular microorganisms is traditionally very, very difficult. Even if you have access to quality testing, the lifecycle of these species can make many of them difficult and expensive to quantify. However, Legionella and Rickettsia species frequently show up in Biomesight and other microbiome reports.
If you have a reason to suspect intracellular species are going to be included in your collection of pathogens:
MicrogenDX can provide "shotgun" metagenomic sequencing of samples to
US customers for "research only" purposes and an extra fee, if your
doctor contacts them.
ArminLabs EliSpot and TickPlex tests are able to detect a wide range of pathogenic species - https://arminlabs.com/en/tests/elispot
MDL can provide comprehensive data via their OneSwab test - https://www.mdlab.com/testing/vector-borne/
Vibrant Wellness Tick-borne test has a wide range of inclusions and uses multiple methodologies -
US / Worldwide: https://shop.drjabanmoore.com/products/copy-of-vibrant-wellness-tickeborne-complete-1-0
US / Worldwide: https://labtestshop.com/tests/vibrant-tickborne2_panel/
Similarly, elimination of intracellular species has additional challenges to other microorganisms. Getting the immune system restored to normal functionality and ongoing use of circulating biofilm breakers is a key part of resolving these infections. Specific anti-microbials can be used to manage and accelerate this process.
Fermenting species identification
Once you have collected accurate microbiome data, you can use it to identify overgrowth of any species which produce alcohol and/or acetaldehyde using this table.
The Biomesight data analysis tool will quickly interpret exported
Biomesight CSV files against this table.
https://bornfree.life/learn/biomesight-tool/
However, manual or AI processing of other microbiome reports is still required.
Notes and considerations:
1. Some species produce alcohol from carbohydrates or lactic acid.
2. Other species produce acetaldehyde when provided with alcohol and may otherwise be harmless.
3. Some produce both.
4. Some probiotic species are also included for accuracy, however these are not considered problematic under normal circumstances.
5. Some species found outside the gut that only produce acetaldehyde may benefit from alcohol produced in the gut or from dietary intake. Therefore, you may have difficulties remediating overgrowth of these species in other tissues until moderate - severe fermentation by the gut microbiome is remediated.
6. This list is comprehensive, but not exhaustive. It will be added to as a comprehensive literature review is completed and GenBank entries processed.
7. It's a very interesting observation that all of the species known to be causal for common issues like acne and dandruff to various cancers are found in this list.
8. Many microorganisms possess at least some capacity to degrade proteins (e.g., to obtain nutrients), but not all are well‐known or clinically significant for their proteolytic activity. The table below highlights species commonly cited in the literature for notable or well‐characterized proteolysis.
Reversing the trajectory of chronic disease means understanding the relevant variables and influences for each unique journey and addressing them.
This section discusses aspects of our daily lives which influence key outcomes, how to quantify them and how to address them.

Planning and consuming an appropriate / strategic diet are complex topics for most people, even without a chronic disease.
A new Meal Planner tool has been added to help you reach targets safely.
For those with a chronic disease, it's significantly more complex. One common challenge is selectivity - trying to ensure that your cells
are receiving these dietary nutrients, while avoiding feeding them to certain
microorganisms residing in your GI tract - which then produce endotoxins
/ mycotoxins that poison your energy metabolism and neurotransmitter
pathways. Acetaldehyde is one of the toxins discussed heavily in the disease model, as part of Gut Fermentation Syndrome (GFS).
Failure to adapt your diet around your personalised microbiome dysbiosis and chronic disease metabolism will invariably lead to "getting stuck" or even back-sliding. Unlike minerals deficiencies, which are normally slow to develop and slow to resolve, microbiome dysbiosis can rapidly shift during immune activity or by feeding the wrong microorganisms over a number of weeks. What you eat determines which microorganisms get promoted or inhibited.
Diet plays a pivotal role in chronic disease by influencing substrate availability for fermenting microbes and shaping the gut microbiota composition. High-carbohydrate diets provide ample fuel for microbial fermentation, exacerbating acetaldehyde production and metabolic disruptions. Conversely, low-carbohydrate diets can reduce substrate availability, potentially decreasing microbial fermentation and acetaldehyde levels, however these can also exacerbate glycogen storage issues and contribute to various symptoms like POTS, fatigue, depression and other neurological symptoms. This has been labelled by some as “low carb limbo”.
Depending on the functionality of different energy pathways, while first starting this protocol, you may also find you respond better to certain type of macronutrients, ie. carbohydrates, fats and proteins than others.
The performance of your diet can be predicted in the Organic Acids Test (OAT) results, by looking at the relevant pathways for metabolites of each macronutrient, eg. glycolysis, fatty acids, amino acids. Some of the adjacent pathway markers, such as ketogenesis, lactic acid and oxalate metabolism are also helpful in identifying impaired pathways, indirectly.
Therefore, before we go into detailing specific foods and their attributes, it helps to understand a little more about the different energy pathways and how dietary macronutrients can be turned into energy.
Feeding energy pathways
You need different energy substrates for different purposes and loads. Those pathways need fuels, cofactors and signalling to work correctly. Let's review them:
Instant / burst energy (muscle tissue)
ATP-PC (Phosphocreatine) System
Where: Not used in liver and adipose tissue.
Substrates: Phosphocreatine (PC) stored in muscles.
Requirements: Dietary creatine. Creatine produced from the urea cycle, using dietary protein. Dietary phosphorus intake. Promoted by sex and thyroid hormones.
Uses: High-intensity, short-duration activities (e.g., sprinting, weightlifting).
Availability / Duration: 10-15 second bursts.
Trigger/Signaling: Immediate energy demand; catecholamines increase utilization.
High intensity energy demands
Glycolysis
Where: Not used in red blood cells (RBCs), as they rely entirely on anaerobic glycolysis, and white adipose tissue prefers fatty acid metabolism.
Substrates: Glucose or glycogen.
Requirements: Dietary carbohydrate intake or gluconeogenesis. Phosphorus. Biotin. Vitamin B3 (as NAD+). Zinc. Magnesium / Manganese. Potassium. Chromium. Vanadium. Thyroxine (calcium, iodine, selenium, heme, tyrosine). Vitamin B1 (as TPP). Lipoamide. Promoted by sex and thyroid hormones.
Uses: Brain activity. Moderate to high-intensity activities (eg., walking / running upstairs, thinking).
Availability / Duration: Muscles - up to 2-3 minute bursts, subject to glycogen reserves.
Trigger/Signaling: Increased ADP levels; catecholamines enhance glucose availability via cAMP-PKA signaling, inhibiting glycogen synthase and activating glycogen phosphorylase.
Glutaminolysis (anaplerosis)
Where: Not used in red blood cells due to lack of mitochondria and adipose tissue due to limited metabolic flexibility.
Substrates: Glutamine.
Requirements: Dietary glutamine, or glutamine created from citric acid cycle activity. Vitamin B3 (as NAD+). Zinc. Magnesium / Manganese. Promoted by sex hormones.
Uses: Rapid cellular proliferation (eg., immune response) and intense brain activity.
Duration: Continuous during demand.
Trigger/Signaling: Stress-induced catecholamine elevation may indirectly upregulate this pathway.
Sustained energy demands
Fatty Acid Oxidation
Where: Not used in brain cells due to fatty acids not crossing the blood-brain barrier, nor red blood cells due to lack of mitochondria.
Substrates: Fatty acids
Requirements: Dietary fats or lipolysis. Carnitine for the carnitine shuttle. Vitamin B2 (as FAD). Vitamin B3 (as NAD+). Vitamin B5 + cysteine (as Coenzyme-A). CoQ10. Lymphatic system is used to transport dietary fats.
Uses: Basal daily metabolism. Low to moderate-intensity activities (eg., walking, endurance sports).
Duration: Indefinite.
Trigger/Signaling: Prolonged energy demand; catecholamines promote lipolysis, increasing free fatty acids for oxidation.
Branched Chain Amino Acid (BCAA) Catabolism
Where: Low activity in the smooth muscle, brain and liver. Primarily used in skeletal muscle, heart, and kidney tissues.
Substrates: Leucine, isoleucine, valine.
Requirements: Dietary protein intake. Vitamin B1 (as TPP). Vitamin B2 (as FAD). Vitamin B3 (as NAD+). Lipoic acid (as lipoamide). Biotin. Vitamin B12 (as adenosylcobalamin). Vitamin B6 (as P5P). Vitamin B5 + cysteine (as Coenzyme-A). CoQ10. Potassium. Magnesium.
Uses: Prolonged exertion, especially with low glycogen.
Duration: Sustained.
Trigger/Signaling: Catecholamines promote protein breakdown, increasing BCAA availability.
Backup energy pathways for excessive load and various mitochondrial dysfunction
Anaerobic Glycolysis / Lactic Acid Metabolism
Where: Not used in liver (under normal conditions) and heart (prefers aerobic metabolism). Promotes neurogenesis and myogenesis.
Substrates: Glucose.
Requirements: Dietary carbohydrate intake or gluconeogenesis, NAD+, Zn, Mg, Biotin.
Uses: High-intensity activities with limited oxygen.
Duration: Short bursts, up to 2-3 minutes.
Trigger/Signaling: High ADP/ATP ratio, catecholamines enhance lactate production through glycogenolysis.
Astrocyte-Neuron Lactate Shuttle (ANLS)
Where: Found in the brain. Lactate can also circulate and participate in the Cori Cycle.
Substrates: Glucose (astrocytes), lactate (neurons).
Requirements: Dietary carbohydrate intake or gluconeogenesis.TBC.
Uses: Neural activity, intense cognitive tasks where glycolysis is insufficient.
Duration: Continuous during brain function.
Trigger/Signaling: IFN-gamma, others. Norepinephrine enhances glucose uptake in astrocytes, promoting lactate production for neurons, similar to an intra-brain Cori cycle.
Cori Cycle / Lactic Acid Cycle
Where: Systemic
Substrates: Lactate (from muscles, brain).
Requirements: Dietary carbohydrate intake or gluconeogenesis. TBC.
Uses: High-intensity exertion / mitochondrial dysfunction.
Duration: Normally short-term, during recovery.
Trigger/Signaling: Epinephrine increases lactate production, fueling the Cori cycle.
Ketogenesis + Ketosis
Where: Ketones are generated in the liver, but not used by it. Red blood cells cannot use ketones due to lack of mitochondria.
Substrates: Fatty acids.
Requirements: Dietary fats and/or lipolysis. TBC.
Uses: Prolonged fasting, low carbohydrate intake / impaired glycolysis, or low liver glycogen.
Duration: Sustained during glycogen depletion.
Trigger/Signaling: Catecholamines promote lipolysis, increasing fatty acids for ketone body production.
Examples of some less utilised pathways, which may be promoted / abused when primary pathways fail
Tyrosine Catabolism
Where: Not used in red blood cells and adipose tissue due to limited enzymatic activity for this pathway.
Substrates: Tyrosine.
Requirements: Dietary intake of tyrosine and/or microbiome synthesis. P5P. Ferritin. Calcium. Magnesium.
Uses: Various, including stress, mitochondrial dysfunction.
Duration: Continuous, where tyrosine exists.
Trigger/Signaling: Catecholamines do not directly regulate but are derived from tyrosine.
GABA Shunt
Where: Not used in liver and skeletal muscle as they are not involved in neurotransmitter metabolism.
Substrates: GABA via glutamate or polyamine metabolism.
Requirements: P5P, magnesium.
Uses: Neural activity, especially during TCA cycle impairment and oxidative stress.
Duration: Continuous.
Trigger/Signaling: Catecholamines influence neurotransmitter release but do not directly regulate GABA metabolism.
Urea Cycle (Argininosuccinate)
Where: Not used in brain and muscle tissue since the urea cycle is primarily hepatic.
Substrates: Amino acids (arginine).
Requirements: Dietary protein intake. Aspartate.
Uses: Ammonia elevation, protein metabolism / high protein intake.
Duration: Continuous.
Trigger/Signaling: Catecholamines indirectly increase ammonia load, requiring urea cycle activity.
Food Intolerances
You also may have already developed a number of food intolerances.
Some of these intolerances are "simply" endotoxins being produced by overgrowth of unwanted microbial species living in biofilms inside your GI tract, consequently being sustained by your intake of various dietary carbohydrates and/or other nutrients, such as sulfur-rich compounds These endotoxins can inhibit energy metabolism, neurotransmitter homeostasis, histamine degradation and various other pathways.
Standard mixed diets vs ketogenic diets
"Sometimes the easiest way to solve a problem is to stop participating in the problem." - Unknown
(In this context, "You cannot efficiently eliminate or reduce overgrown species while you're also feeding them.")
Standard mixed diet
A standard mixed diet typically includes a balanced intake
of carbohydrates, proteins, and fats. In the context of the disease model, this diet may
inadvertently contribute to increased fermentation and unwanted biofilm development. The high carbohydrate
content fuels microbial ethanol and acetaldehyde production, leading to
continued impairment of energy pathways due to elevated acetaldehyde. Symptoms
such as fatigue, cognitive impairment, and metabolic abnormalities may persist
or worsen under this dietary regimen.
Depending on the species and locations of the biofilms
containing these microbial species, you may have more success avoiding
symptoms by consuming different types of carbohydrates.
eg.
a.
Simple carbohydrates / sugars may feed any existing microbial
overgrowth in the mouth / throat / oesophagus / stomach / small
intestine. In the absence of dysbiosis in those tissues, simple
carbohydrates can also be readily absorbed in the small intestine,
before reaching any dysbiosis in the large intestine, should it exist.
b.
Complex carbohydrates may not be broken down until further along the GI
tract and may skip feeding some of the populations residing in biofilms
in the small intestine.
c. Different types of dietary fibres and starches may selectively feed some species and not others. (see "2.2.3 -- Prebiotics"")
d.
Gliadin in gluten may generate an immune response due to molecular
mimicry of the protein in the "hook" of Candida's hyphae form. Gliadin
is also used by a particular pathogenic strain of Streptococcus
salivarus to produce an antigen that punches holes in enterocytes,
leading to gut barrier degradation, immune response and inflammation. Giardia infections are also known to create gluten intolerance.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4368562/
https://pubmed.ncbi.nlm.nih.gov/22617359/
In some types of more severe dysbiosis (and where your B vitamin and mineral status also supports this), you may find swapping more carbohydrates for
protein can be helpful in avoiding endotoxemia symptoms such as
nausea, bloating, diarrhoea, histamine reactions, tachycardia,
headaches, etc. These will resemble die-off symptoms, as the same toxins
are involved (see: 2.3.1-Herxheimer / die-off / acetaldehyde-support).
Here is an example 2000kcal mixed-diet, visualised in Cronometer:

Ketogenic diet
The ketogenic diet, characterized by high fat, moderate
protein, and very low carbohydrate intake, offers a contrasting approach to
a standard mixed diet or a low carbohydrate diet.It also avoids "low carb limbo" by promoting generation of ketone bodies in the liver.
In extreme gut microbiome dysbiosis cases, changing to a
ketogenic diet for a period of time can also be very helpful in reducing
fermenting species, however will require commitment to endure an often
unpleasant induction (1 week) and then adaptation phase (2 weeks). If
your OAT results already show elevated ketone markers, this is much
easier. Studies suggest the acute effects of a ketogenic diet on your
gut microbiome will last around 12 weeks, before the microbiome adapts.
Combining this window of opportunity with other interventions in this protocol can allow
you to break the existing cycle with lasting results.
By significantly reducing carbohydrate consumption, this diet limits the
substrates available for microbial fermentation. As a result, endogenous
ethanol and acetaldehyde production may decrease significantly in response to food
intake, alleviating some of the metabolic disruptions caused by GFS.
However, circulating acetaldehyde and other endotoxins will still be
experienced, making the first 1-2 weeks of a ketogenic (the induction phase)
more unpleasant than it would be for someone without GFS.
A key point of difference is that the ketogenic diet promotes fatty acid oxidation and ketone body production as alternative energy sources. Ketone bodies can cross the blood-brain barrier and provide energy to the brain (much more efficiently after weeks of being on a ketogenic diet), potentially improving cognitive function and reducing fatigue. Additionally, this diet may alter the gut microbiota significantly, reducing fermenting microbial populations and promoting a healthier balance.
Mechanisms of Ketogenic Diet's Impact on GFS
Carbohydrate Restriction
Limiting carbohydrate intake directly reduces the amount of glucose and other fermentable sugars in the gut. This reduction in substrates can lead to decreased microbial fermentation activity, resulting in lower ethanol and acetaldehyde production. With less acetaldehyde burden, the inhibitory effects on metabolic enzymes are alleviated, helping to restore the cellular redox balance and improve the function of gluconeogenesis and fatty acid oxidation pathways.
Fatty Acid Oxidation and Ketogenesis
The ketogenic diet's high-fat composition encourages the body to utilize fats as the primary energy source. This shift promotes the production of ketone bodies in the liver through a process called ketogenesis. Ketone bodies serve as an efficient alternative energy source for various tissues, including the brain and muscles. By providing a consistent energy supply, the diet addresses the energy deficits caused by acetaldehyde-induced metabolic disruptions. Additionally, relying less on impaired glucose production pathways reduces the risk of hypoglycaemia.
Benefits of a Ketogenic Diet in GFS
Implementing a ketogenic diet in GFS management offers
several potential benefits. By reducing acetaldehyde levels, the diet can help
restore normal metabolic functions, improving energy production and overall
well-being. The provision of ketone bodies as an alternative energy source may
alleviate symptoms such as fatigue and cognitive impairments. Furthermore, the
reduction in carbohydrate intake may lead to favourable shifts in gut
microbiota composition, decreasing the population of fermenting microbes
responsible for excessive acetaldehyde production.
Potential Challenges
Despite its potential advantages, the ketogenic diet
presents challenges that must be carefully considered. The restrictive nature
of the diet can make long-term adherence difficult for some people. There is
also a risk of nutrient deficiencies, particularly in electrolytes, fibre,
vitamins, and minerals, if the diet is not properly managed. Monitoring thyroid
function is also helpful, as very low carbohydrate intake can sometimes reduce
T3 levels, potentially affecting metabolic rate. Additionally, high-fat diets
can impact beneficial gut bacteria, necessitating careful planning to maintain
gut health.
A manganese deficiency will significantly impact hepatic gluconeogenesis, as will zinc and magnesium deficiencies.
These should be somewhat addressed before attempting keto induction.
NB. The reduction in glucose availability may affect cognitive function where neural hypoxia exists - due to eg. structural issues, coagulation and/or transport issues, severe iron deficiency, and also blocked lymph nodes in the neck and/or nasopharynx (usually relating to localised infection). The reduced glucose affects lactic acid metabolism involved in the Astrocyte-Neuron Lactate Shuttle and ultimately energy availability in neurons. This can also be a cell danger response trigger.
Strategic Implementation
Successful implementation of a ketogenic diet for GFS
requires proper planning to ensure safety and efficacy. A personalised
nutritional plan tailored to individual needs and tolerances can enhance
adherence and effectiveness. Cronometer
is very helpful in planning and visualising a successful day. Setting expectations ahead of time will help allow you to "keep calm and keto on" during unpleasantness.
Supplementation with essential electrolytes, vitamins, minerals, and probiotics
like the ones in this protocol may be necessary to address deficiencies and
support gut health.
A gradual transition into the diet, by slowly reducing carbohydrate intake, prolongs
keto adaptation and exacerbates energy crisis symptoms. It is not recommended.
A rapid transition normally creates temporary symptoms of "keto flu",
which can be managed by using GoBHB exogenous ketone supplements and essential
amino acids (EAAs) during the dietary transition.
Strictly restricting carbohydrate intake is paramount to the
diet, which involves eliminating sugars and refined carbohydrates like
sweets, sugary drinks, white bread, and pastries. Removing starchy foods
such as potatoes, rice, pasta, and grains is also necessary. Instead, consuming
non-starchy vegetables like broccoli, cauliflower, kale, and bell peppers (capsicum)
provides essential nutrients with minimal carbohydrates. The target daily net
carbohydrate (total carbohydrates, minus fibre) upper limit is 25g.
Increasing the intake of healthy fats supports the
ketogenic approach. This includes consuming monounsaturated fats found in olive
oil, avocados, and nuts, as well as omega-3 fatty acids from fatty fish such as
salmon and mackerel. Saturated fats from sources like coconut oil and butter
can be included. Butter is also a good source of butyrate, which may trigger rapid,
beneficial changes to the microbiome and energy metabolism, however, this will also trigger die-off
symptoms and potentially induce rapid alcohol withdrawal symptoms.
Protein intake is important for essential amino acids and to
allow the liver to perform hepatic gluconeogenesis for brain and other tissues.
Balancing protein intake is important because excessive protein can be
converted into glucose, potentially triggering an insulin response that
inhibits keto induction / adaptation, while also fuelling microbial fermentation,
depending on the location of the biofilms. The longer the protein take to
digest, the further along the GI tract it will be before potentially feeding
the microbiome.
Keto induction is easier with more fats than protein, initially.
For example,
During keto induction, you could consume:
170g fat @ 1530 kcal +
100g protein @ 400 kcal
= 1930kcal
After keto induction, you can transition to consuming roughly 1:1 of fat:protein, on a per-gram
basis:
150g fat x9 = 1350kcal
150g protein x4 = 600kcal.
= 1950kcal.
(Scale this by your calorific needs.)
High-quality protein sources such as lean meats, poultry, eggs (a great source of
lecithin for phosphatidylcholine), and plant-based proteins like nuts (good
mineral sources) and tofu (some people may have tolerance issues) are
recommended.
Maintaining proper hydration and electrolyte balance is
essential. Adequate water intake supports detoxification and metabolic
processes, while sufficient electrolytes help prevent imbalances that will
reliably occur during the initial stages of a ketogenic diet, as glycogen
stores are intentionally depleted.
Here is an example 2000kcal ketogenic diet, visualised in Cronometer:
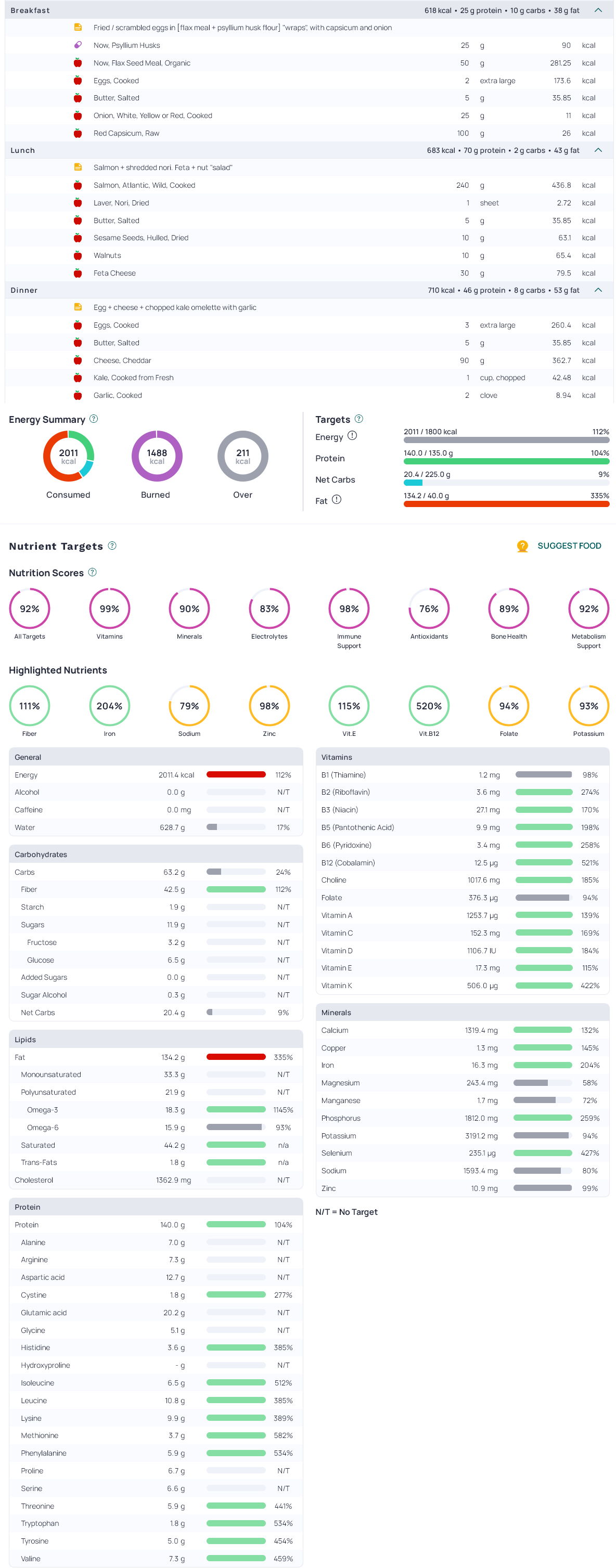
Inflammation and/or gut membrane permeability issues due to microbiome dysbiosis and related immune activity often leads to further histamine elevation and temporary IgG antibodies being produced. This is normal behaviour in response to complete foreign proteins getting through the barrier and triggering an immune response. In this state, foods which trigger mast cell activation and histamine release should be avoided for 6-8 weeks before reintroducing them, preferably after the barrier dysfunction has been sufficiently improved / resolved.
Due to metabolic impairments being described in this disease model, other food intolerance issues are entirely expected. The disease model and collected data shows that aldehyde toxicity / impaired aldehyde metabolism leads to elevations of serum Vitamin B6, creates issues metabolising "inactive" forms of Vitamin A into the active forms, creates issues degrading histamine and separately, other issues promoting lactic acid metabolism also elevate endogenous biosynthesis of oxalate.
In this state, additional intakes of these nutrients / compounds may exacerbate existing symptoms. These issues are targeted in Stage 1 of the protocol and allows dietary intakes to become more flexible. Overall, foods need to be carefully managed and reintroduced as the related
metabolic impairments and barrier function issues are resolved.
Active Vitamin A deficiency
Vitamin A isn't a single molecule, but rather a chain of metabolic conversions that transform dietary precursors into active signalling compounds. The story begins with retinyl esters, the storage form found in the liver and other tissues. When needed, these are converted into retinol, a transportable alcohol that circulates through the bloodstream and enters cells as required. (see Figure 8)
Inside the cell, retinol takes on a more active role. It's oxidised into retinaldehyde (often shortened to retinal) and then further into retinoic acid, the bioactive form that influences gene expression. These transformations are not spontaneous. They are mediated by specific enzymes, and each one depends on particular cofactors and cellular conditions.
There are several isomers involved in this process. The most common is all-trans-retinol, which feeds into the production of all-trans-retinoic acid (atRA). But there are also 9-cis and 11-cis forms of both retinol and retinal, each with their own signalling roles. The final step - the irreversible conversion of retinal into retinoic acid - is catalysed by the aldehyde dehydrogenase enzymes: primarily ALDH1A1, with ALDH1A2 and ALDH1A3 playing secondary roles depending on the tissue. This is the same enzyme responsible for degrading neurotransmitters.
This is where problems begin to surface. ALDH1A1 is a fragile enzyme. It requires NAD⁺ to function, which makes it vulnerable in states of redox imbalance. Conditions that lower NAD⁺, such as mitochondrial dysfunction, acetaldehyde excess, inflammation, or chronic infection-can slow the enzyme down. Worse, acetaldehyde, a byproduct of both alcohol metabolism and microbial fermentation, also directly inhibits ALDH1A1. Add in common deficiencies of zinc and magnesium, or a cellular environment overloaded with oxidative stress, and the enzyme’s activity may be effectively crippled.
When ALDH1A1 fails, the metabolic pathway clogs. Retinal cannot be converted into retinoic acid. As this step is irreversible, there’s no workaround within the body. Retinol supplements won't help - in fact, retinol can build up to apparently toxic levels. Carotenoids won't help. The machinery is blocked downstream, and the most critical signals simply don’t arrive.
Retinoic acid itself exists in several forms. All-trans-retinoic acid activates retinoic acid receptors (RARs) that regulate genes responsible for epithelial integrity, preventing hyperkeratosis (KLK pathway), immune regulation, detoxification, and neurodevelopment. Meanwhile, 9-cis-retinoic acid is required to activate retinoid X receptors (RXRs). RXRs are the central dimerisation partners for many other nuclear receptors, including PPARs, LXR, FXR, VDR, TR, and others. Without 9-cis-retinoic acid, these systems cannot operate at full capacity.
The consequences of low 9-cis-RA reach far beyond vitamin A metabolism. RXR-PPAR dimers, which govern fatty acid oxidation, ketogenesis, lipoprotein metabolism, adipogenesis, insulin sensitivity, inflammation resolution, energy expenditure, muscle metabolism and neuroprotection become hypoactive.
RXR-LXR dimers, essential for cholesterol transport and immune homeostasis, stall. Even RXR-VDR complexes, which modulate calcium and vitamin D responses, lose efficacy. FXR heterodimers regulating bile acid synthesis inhibition, plus lipid & glucose metabolism start fail to perform.
The deficiency of this one vitamin's metabolites sends a ripple through every metabolic and endocrine axis it touches.
When this problem is recognised, the logical therapeutic step, while correcting the upstream influences, would be to provide retinoic acid directly, bypassing the broken ALDH enzymatic activity. However, rather than being available as a dietary supplement, all-trans-retinoic acid is sold as a drug under the name Tretinoin. It’s used clinically for certain types of acne, photoaging, and acute promyelocytic leukaemia. But it is also a prescription-only, regulated substance, patented and restricted, despite being identical to a molecule the body produces endogenously.. when it can.
Your doctor may provide a prescription for off-label use of a tretinoin cream (not to be mistake for isotretinoin / 13-cis retinoic acid), which can be used inside a mucosal tissue targeting a daily dose of around 1mg, which might be an amount of cream resembling something like the "size of a pea", twice per day, depending on the concentration of the cream (typically 0.05 - 0.1%). For 0.1% concentration, 1g of cream = 1mg of all-trans retinoic acid.
It would be best to implement tretinoin after any pre-protocol support / basic stage 1 onboarding has completed.
Unlike other forms of vitamin A, all-trans retinoic acid does NOT accumulate / store and has a very short half-life of under 1 hour.
Very large (non-nutritional, eg. 700x) doses of all-trans retinoic acid inhibits Hypoxia Inducible Factors (HIF) and are therefore being explored in early cancer research. In (often infected) tissues relying Warburg metabolism, this can trigger cellular apoptosis / necrosis, by inhibiting the metabolic sensor downstream of prolyl hydroxylase activity, that signals for cells to switch to lactic acid metabolism / anaerobic glycolysis for survival.
There’s something quite peculiar about how a key developmental and repair vitamin which determines the behaviour of epithelial cells, immune tolerance, and even neural differentiation is, for most people, functionally inaccessible unless they're being treated for a specific, medically recognised condition. Its dietary replacement has been patented, monetised, and regulated as acne medication or an ingredient for therapeutic skin care products.
In situations where ALDH1A1 is impaired-through eg. chronic alcohol exposure, microbial fermentation, or long-term metabolic damage-this silent blockade may contribute to a breakdown in tissue maintenance, mucosal immunity, and metabolic feedback. It is a central mechanism, rarely measured, yet fundamental to the organism's capacity to respond to stress, repair damage, and regulate its own biochemistry.
Meal composition and timing is also important when energy metabolism is impaired. Part of the metabolic cascade includes type-2 diabetes and metabolic syndrome, so the dietary strategies will look very similar.
In the context of the disease model including glucose uptake and glycogen storage issues, the BCAA content of dietary protein intake may be very helpful in refilling glycogen stores via an alternate route, depending on your manganese, zinc, magnesium, biotin, B1, B2, B3, P5P and B12 status. In addition to general energy availability improvements, the model shows this is helpful for preventing PEM and crashes, providing oxidative stress and coagulation is being managed.
Vitamin Q deficiency
A healthy microbiome normally produces queuine or "Vitamin Q", which has been identified as an essential nutrient (our bodies can't make it). Vitamin Q is needed for maintaining BH4, aspartic acid, asparagine, histidine, and tyrosine. It's required for mitochondrial metabolism, blood-flow and neurotransmitter homeostasis. Vitamin Q also promotes lactobacillus species. RAW coconut water is a surprisingly rich source (heat treating destroys it, so choose carefully). Milk and particularly wheat germ (gluten source) are also rich sources.
Strategic foods
A table of microbiome transforming foods is provided in 2.2.3 -- Prebiotics and should be considered a required part of the protocol and any strategic diet.
The concept of "roughage" and its role in helping to disrupt and remove mucous + biofilms, especially when combined with additional biofilm breaking food items / compounds is often underappreciated in meal planning.
Foods to generally consume as part of the protocol (as tolerance allows / increases):
Foods to consume cautiously (or in some cases, avoid) as your aldehyde metabolism, etc normalises (monitor serum cholesterols, B6, beta-carotene):
In the tables below, you'll find food items and their relevant attributes, which you can use to help you get started building meals.
These tables are best viewed on a computer or tablet. On mobile devices, some columns will be hidden to fit the screen.
The columns can be sorted and cautions or elevations of potentially inappropriate nutrients in foods items when getting started have been highlighted in red.
These tables are not intended to replace https://cronometer.com, which is incredibly helpful in visualising and planning your dietary strategy.
Protein sources:
Carbohydrate sources:
Micronutrient sources:
The lymphatic system is a network which spans the majority of the human body. Until quite recently, it was not known that this also included the brain.
The lymphatic system has a number of important roles in immunity and circulation. Lymphoid organs are the source of B and T lymphocytes. The system transports dietary fats and collects extracellular fluid and metabolites from tissues, returning them via lymphatic vessels to the bloodstream, preventing lymphoedema or catastrophic fluid build-up, pressure / pain and metabolic backlog.
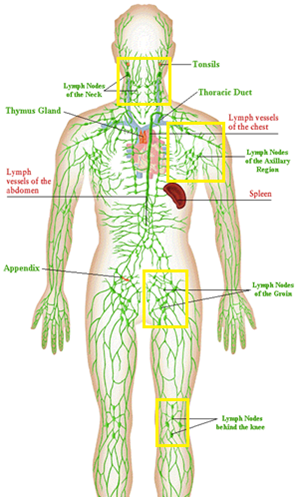
A friendly primer on the lymphatic system can be found here: https://www.britannica.com/science/lymphatic-system
The lymphatic system relies on breathing and muscle contractions to maintain healthy circulation and waste excretion. Calendula creams can also help move lymph.
In any disease where movement is being restricted, this creates additional difficulties for maintaining immune function, fat transport and metabolite circulation. The lymphatic system can become blocked. This may be observed as being stiff, or having sore swollen tissues that
can feature enlarged lymph nodes, such as in the neck, groin and/or
armpits, relative to adjacent infections. Failure to maintain the lymphatic system may create a serious roadblock to recovery.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5954877/
A session with a massage therapist who specialises in lymphatic drainage may help you assess and remediate any recurring lymphatic blockages. There are also some helpful videos online with comprehensive instructions.
A daily regimen to maintain any problematic areas by hand or
vibrating massage gun (used on a glancing angle), may also assist
unlocking functional gains and preventing pain in chronic illnesses /
infections.
https://youtu.be/ccV24hCOe5A
https://youtu.be/dDrJajg2ZII
Localised pressure / oedema, numbness, hypoxia, impaired
blood flow, "burning" sensations, pain and lactic acidemia can be expected when lymph nodes
become blocked from nearby immune activity.
eg.
Intracranial pressure is regulated by nasopharyngeal, occipital and cervical lymph nodes in the face and neck. If these lymph nodes become blocked, crippling head pressure can be experienced. This is especially noticeable if immune activity increases from eg. improved energy metabolism / resolving deficiencies. Intracranial pressure can be a blocking issue to making any forward progress, if left unresolved. Chronic intracranial pressure issues and nasal / sinus inflammation are commonly found where environmental mould issues are unresolved, see 2.2.3 Living without chronic dysbiosis.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10808075/
https://www.nih.gov/news-events/nih-research-matters/lymphatic-vessels-discovered-central-nervous-system
NB.
The nasopharyngeal lymph nodes are largely inaccessible via manual manipulation, although a soft attachment and glancing angle with a vibrating massage tool on either side of the nose may help. Resolving infections in the nasopharynx reduce load on those lymphatic vessels. The occipital and cervical lymph nodes are much easier to access and clear.
https://bornfree.life/images/neck-lymphatic.mov
Face and sinuses can become acutely painful if related lymph nodes are blocked. These nodes are usually very easy to access with your fingers or a vibrating massage tool.
Here is a diagram you can follow to help improve lymphatic flow, by dragging your fingers in the same locations and directions of the arrows. Areas with multiple arrows side by side may benefit from using multiple fingers:
Hands and arms can be significantly affected by blocked lymph nodes in the neck and armpits. These nodes are usually very easy to access with your fingers or a vibrating massage tool.
Feet and legs
can be significantly affected by blocked lymph nodes either side of the groin and backs of
the knees. These nodes are also easy to access with your fingers or
vibrating massage tools.
NB.Most lymphatic drainage / massage specialists will skip the groin nodes due to being intimate areas, however these are commonly blocked, presumably from immune activity in the gut and/or sex organs.
A strong paradoxical effect may be felt the first time a blockage is cleared.
Yeasts, moulds and fungi are found everywhere in nature and have an important role. They decompose animals, plants and other organisms, recycling their elements and other nutrients, thereby continuing the circle of life.
Usually, these decomposing animals are not alive, however when an organism’s immune response is incapable of maintaining a defence against the normal daily background level of fungal challenge, the living organism will become food for yeast, mould and/or fungi. Various lifestyle influences contribute positively and negatively to maintaining this daily defence.
Lack of exposure to sunlight, lack of sufficient activity to maintain a specific immune function and/or lack of a balanced, protective microbiome can also contribute to an organism being more susceptible to mould. It has been previously said “we don’t grow old, we mould!”
Antibiotics are powerful tools in controlling bacterial infections, however they are also broadly indiscriminate in their effects and are overused in food production + minor infections, leading to a loss of microbiome diversity and also the development of drug-resistant strains. Acute use of them decreases systemic levels of both "good" and "bad" bacteria, creating opportunities for opportunistic fungal overgrowth. Without paying careful attention to diet, probiotics, prebiotics and host metabolism, using broadly destructive interventions against your microbiome can have deleterious effects on your health and happiness.
eg. If you pour weedkiller all over your garden, killing almost all of the flora and then don't replant and cultivate the garden again afterwards, you'll find that over a short time, the plant life now growing back is made up of the most hardy, versatile, adaptable species either left behind or reintroduced by natural processes. These are often the species of weeds you were trying to remove in the first place.
Growing a beautiful garden means making space for what you want to flourish, planting the seeds and then feeding the species you want to keep, so they can out-compete the others. Selective weeding is also helpful. Some fertilisers are selective for species, also. These will be discussed in the Probiotics and Prebiotics sections below.

Maintaining a protective gut microbiome in modern times has a number of challenges due to the germicidal effects of stomach acid, metabolic acidemia and chronic disconnection from our natural source of probiotics via our industrialised food chain / use of preservatives and general preference for cooked food.
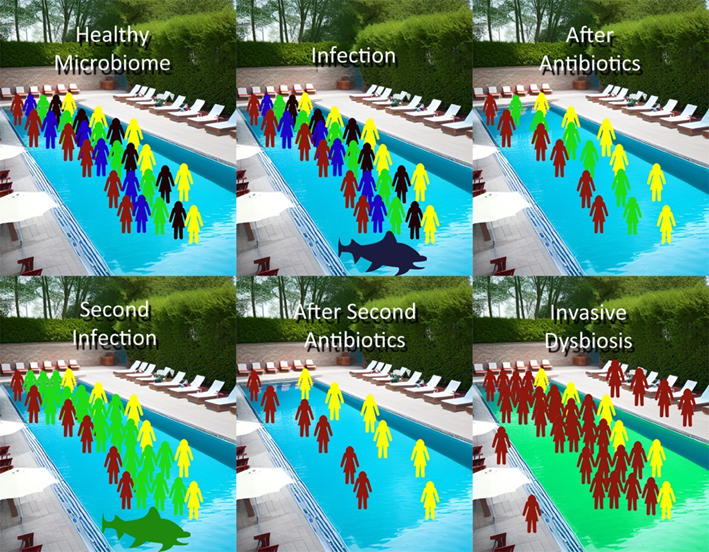
The barrier function of the skin and mucosal layers play an important part in resilience against pathogens. Unfortunately, the human body has a number of tissues that are opportunistic for yeast / mould / fungal and bacterial infections to thrive with minimal interference from direct immune activity, thanks to their ability to form biofilms.
https://www.sciencedirect.com/science/article/pii/S0016508524050546
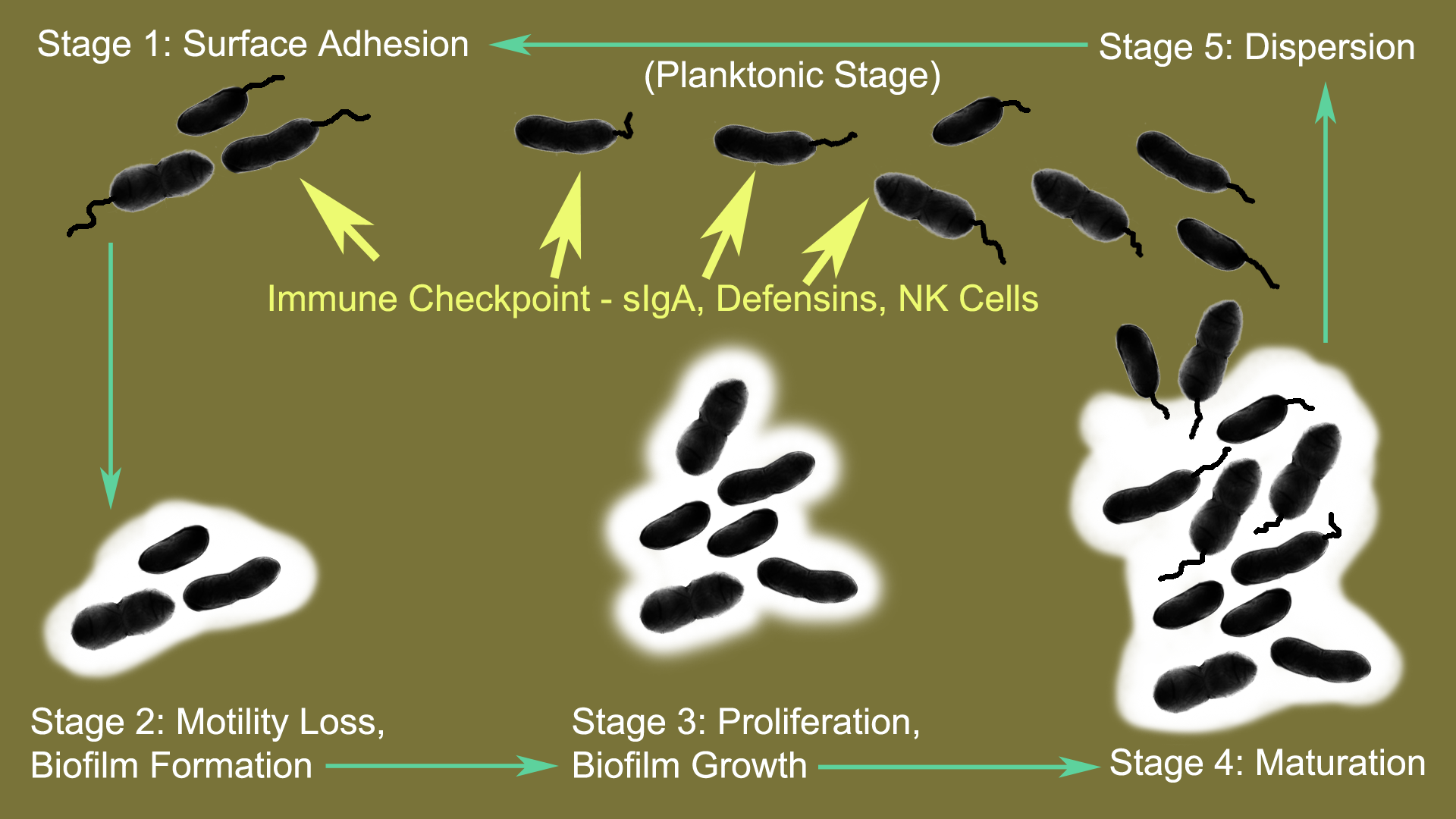
Subgrouping for ME/CFS, PFS, PSSD and other patients may have a
relationship with the locations of infected tissues. Localised
pathogenic biofilm accumulation and chronic innate immune activation.
Nasopharnyx
One example for possible subgrouping relates to the nasopharynx (and surrounding areas), which have a direct route to the central nervous system and also potentially prevents critical signalling from normal nasal breathing, which creates a balanced parasympathetic : sympathetic tone. (see "2.2.6 Cortisol, limbic system, glycogen and IFN-γ - Sympathetic overdrive")
Swollen / enlarged lymph nodes can often be found nearby infected tissues. If these blocked lymph nodes include the nasopharyngeal, occipital and cervical vessels in the neck and face, then crippling intracranial pressure can also be expected, as these nodes regulate intracranial pressure. This can cause debilitating pain, also creating a blocking issue / preventing remineralisation unless resolved beforehand. You can read more about this topic in 2.2.2 Lymphatic maintenance.
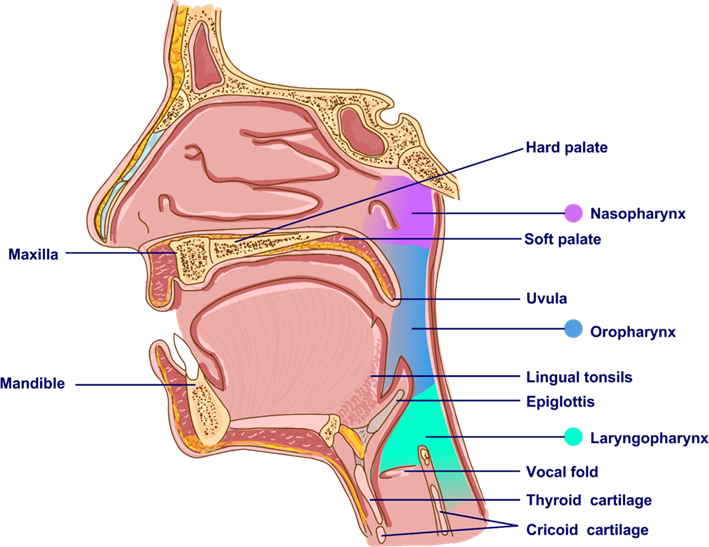
Do you have a history of cracked lips / ears / toes / feet / rectum,
flaking skin, severe acne, dandruff, hair loss, red / inflamed skin patches / rashes,
eczema, psoriasis, nasal inflammation, tonsillitis, sleep breathing
disorder, gut pain / issues, cystitis, prostatitis, mastitis,
epididymitis, white or green/black film on tongue or discharge?
These are strong indicators for potentially invasive microbiome dysbiosis. The extent / severity of the invasiveness of these microbes has a direct correlation with the intensity and duration for activation of chronic innate immune response pathways. These alter energy metabolism towards specific immune functions and generate predictable symptoms, such as neurotransmitter and endocrine dysregulation, POTS, dysautonomia, elevated cholesterols, insomnia, frequent urination, etc., especially where coenzyme or mineral deficiencies are also present.
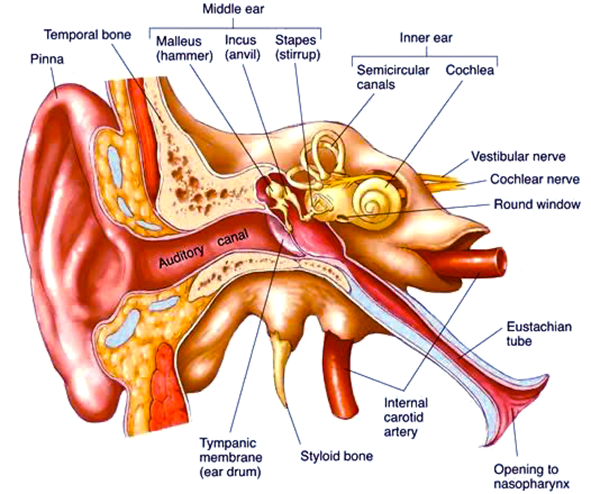
Orifices and tissues such as the nasopharynx, sinuses, throat, Eustachian tubes, ears, GI tract, rectum, vagina, feet, toes are areas which are not regularly exposed to direct sunlight. This list might well include all tissues, where someone is bed-bound or house-bound. These tissues provide “safe spaces” for any pathogenic microorganisms to colonise, create biofilms and thrive, without appropriate immune surveillance.
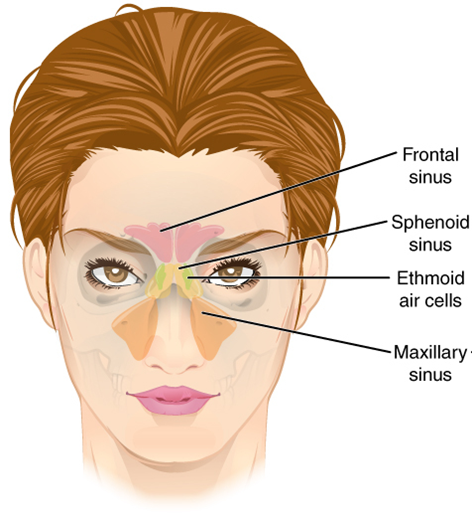
{kind=link}
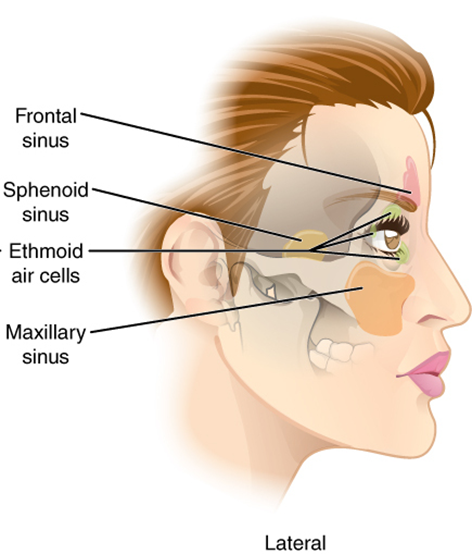
{kind=link}
Gastrointestinal biofilms and pathogens
In the case of a GI tract infection, this may also
affect dietary absorption efficiency and cause endotoxemia, sometimes
leading to gastroparesis, nausea / vomiting in response to food
consumption, along with other potential systemic impairments.
The timing of symptoms onset, in relation to meals may be helpful in identifying the location of unhelpful biofilms / colonies and also which interventions may be the most appropriate. Generally, the shorter the duration between meals and symptom onset, the closer the biofilm / overgrowth is to the stomach.
Upper GI / small intestine dysbiosis / overgrowth may benefit from oral dosing of specific biofilm breakers and related interventions, whereas lower GI / large intestine dysbiosis / overgrowth can be more easily targeted by administration of eg. robusta coffee enemas.
Similarly, upper GI microorganism colonies bloom in response to dietary intakes of simple sugars, BCAAs, etc., whereas colonies in the large intestine benefit more from more complex carbohydrates and proteins, which break down into simple sugars and BCAAs further along the digestion journey.
Upper GI biofilms containing overgrowth of fermenting species can produce toxic gases that are known to cause inflammation, epithelial damage and sphincter dysfunction, which is further connected to reflux / GERD.
Vitamin U (some example supplements - [AU] | [US] | [EU]) also known as S-methylmethionine or DL-methylmethionine, specifically as cabbage juice for bioavailability in the upper GI) was the primary treatment for reflux prior to proton pump inhibitors - primarily as a tissue-restorative intervention and arguably better.
https://pubmed.ncbi.nlm.nih.gov/12671885/
https://pmc.ncbi.nlm.nih.gov/articles/PMC12133511/
Different strategies are needed for different parts of the GI tract.

[adapted from source: https://in.pinterest.com/pin/640355640799063911/]
This protocol currently includes a number of staged interventions to address biofilms and pathogens in different locations inside the GI tract, such as Candex, Biofilm Phase 2 Advanced, NAC, spirulina, curcumin, fulvic acid, prebiotics, targeted probiotics, biofilm flushes, dietary interventions and water-fasting, with an aim of not unduly circulating endotoxins / acetaldehyde in the process of eliminating them, if at all possible. These strategies have been testing well and we are always exploring ways to improve on this process (please join the Discord online community to join the discussion).
Professional endoscopic biofilm removal is possible, however there appears to be a significant problem with general awareness of biofilm issues amongst gastoenterologists, so finding a willing clinician is currently challenging. A paper and video of removal here - https://x.com/joshual_tm/status/1825355958568304834
One of the key challenges is that invasive microorganisms which breach the (mucosal) barrier function can trigger an IFN-γ response, which causes collateral damage and inflammation to infected tissues in the process of oxidising pathogens, using reactive oxygen species.
If the rate of collateral oxidative damage + pathogenic damage exceeds the regenerative capacity of the tissue, this could further compromise the barrier function and dysregulate IFN-γ activity, leading to a “deadlocked” cycle / state. External indicators for insufficient collagen synthesis rates may include hEDS symptoms, poor skin texture, chronic cranial instability, slipped rib syndrome, thoracic outlet syndrome, etc.
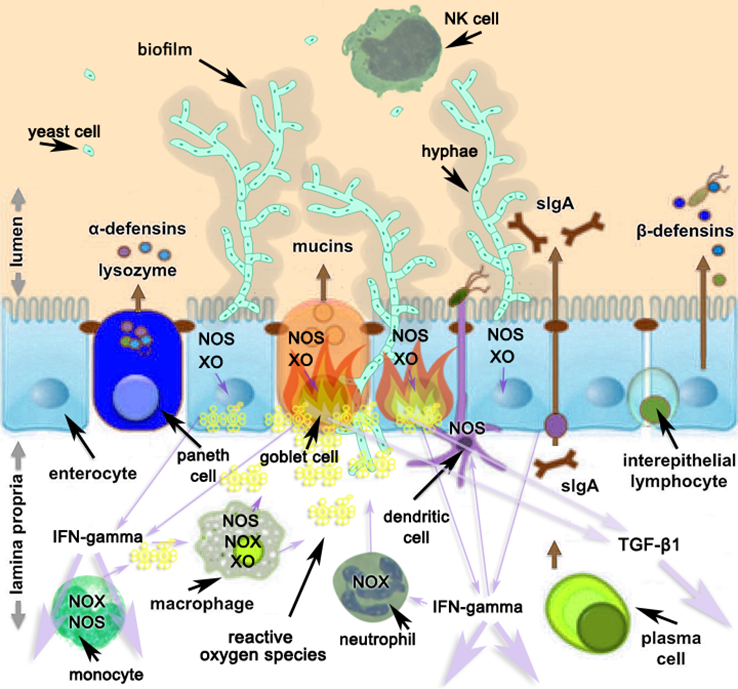
A healthy microbiome appears to play a very important role in providing protection against invasive bacterial, yeast, mould and fungal infections.
Chronic illnesses, including Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) and various inflammatory or metabolic diseases, are frequently associated with gut dysbiosis. A key feature of this dysbiosis is often the reduction of butyrate-producing bacteria and an increase in fermentative species.
https://pmc.ncbi.nlm.nih.gov/articles/PMC12564589/
This loss of butyrate producing species appears to have a strong relationship with (lactic) acidaemia / acidosis and pH drop in the lumen.
Although there is human clinical data showing a 2-3 fold increase of rectal luminal lactate in settings like cardiopulmonary bypass and severe sepsis, this is largely discussed as reflecting mucosal metabolic dysfunction/ischemia (local production and barrier dysfunction), rather than “lactate being intentionally transported into the gut for disposal” and the exact mechanism is unclear.
https://pubmed.ncbi.nlm.nih.gov/16199418/
https://pubmed.ncbi.nlm.nih.gov/17116255/
Normally, lactate is discussed in the other direction of gut-derived lactate entering the system. Mechanistically, lactate is absolutely transportable across gut epithelium. Monocarboxylate transporters, eg. MCT1, SLC16A1 are proton-coupled and are reported as being located on both lumen-facing and basolateral membranes in intestinal epithelium, meaning the flux direction depends on concentration gradients and the local pH gradient.
https://pmc.ncbi.nlm.nih.gov/articles/PMC11748985/
https://pmc.ncbi.nlm.nih.gov/articles/PMC2835396/
https://pmc.ncbi.nlm.nih.gov/articles/PMC6019286/
For lumen pH - the GI tract is already running strong pH control via acid secretion (stomach) and bicarbonate secretion/transport (small intestine, colon). Papers on intestinal bicarbonate transport describe that these processes regulate luminal pH (and the epithelial surface microclimate in particular).
https://pmc.ncbi.nlm.nih.gov/articles/PMC11006743/
https://journals.physiology.org/doi/full/10.1152/ajpgi.00341.2014
The baseline luminal pH varies quite a lot by segment in the GI tract - roughly 6.5 in the proximal small bowel rising toward 7.5 by ileum, dropping near the caecum (fermentation acids), then rising again toward the rectum. This might provide the theoretical gradient in specific sections under the right circumstances and needs more study.
However, there’s also decent evidence that systemic acid-base status changes colonic mucosal intracellular pH and bicarbonate-related handling, and that systemic pH (and bicarbonate/PCO2) can modulate colonic transport processes. This is also a route by which systemic acidosis could indirectly shift luminal pH near the mucosa, even if the bulk lumen is buffered by diet, secretions, and microbial metabolites.
https://pubmed.ncbi.nlm.nih.gov/3925792/
https://journals.physiology.org/doi/abs/10.1152/ajpgi.1983.245.2.G230
https://gastrojournal.org/article/S0016-5085%2896%2900459-3/pdf
Overall, “more study is needed” around how this mechanism works.
Butyrate is a short-chain fatty acid (SCFA) produced by specific gut microbes through the fermentation of dietary fibers. It serves as a primary energy source for colonocytes, contributes to the integrity of the gut barrier, and exhibits anti-inflammatory properties. A decline in butyrate-producing species can compromise the gut lining and increase systemic inflammation. Butyrate influences various pathways to support gut health, including fortifying epithelial tight junctions, inducing regulatory immune cells, and affecting metabolism and the nervous system. Adequate butyrate also aids in stabilising hypoxia-inducible factor (HIF) to promote mucosal healing. The loss of these organisms is linked to reduced fecal butyrate concentrations and worsened intestinal inflammation and permeability in chronic disorders.
Key butyrate-producing species primarily belong to the Firmicutes phylum (Clostridiales order) and include Faecalibacterium prausnitzii, Roseburia spp. (e.g., Roseburia hominis), and Eubacterium rectale. These species collectively contribute significantly to colonic butyrate production. In conditions like ulcerative colitis, irritable bowel syndrome (IBS), and ME/CFS, a reduction in these butyrate-producers is consistently observed.
Conversely, an overgrowth of fermenting species often occurs. These microbes ferment carbohydrates into substances such as lactate, ethanol, hydrogen, and carbon dioxide, which can exacerbate bloating, D-lactic acidosis, and gastrointestinal discomfort. Common fermenters include D-lactic acid bacteria like Enterococcus and Streptococcus, which can produce substantial amounts of lactic acid. Prevotella spp., while capable of fermenting fiber, primarily produce acetate and propionate rather than butyrate, and their overgrowth alongside reduced butyrate-producers may indicate an inefficient cross-feeding network. Proteobacteria (eg. Escherichia, Klebsiella, Enterobacter) can also expand during dysbiosis, potentially driving inflammation and endotoxin release. Yeasts, such as Candida, can also ferment sugars to alcohol and gas, contributing to dysbiosis. There is a large table of fermenting species in the microbiome testing section and a tool to analyse Biomesight report data.
https://link.springer.com/article/10.1186/s12866-025-04650-9
Apart from generating gaseous toxins, ethanol and acetaldehyde -
depleting silicon and other metals in compensation, many yeasts / mould /
fungi and bacteria can cause dramatic metabolic alterations. They have
an ability to break through our skin / epithelial tissue / mucosal
barrier function from immune-evasive biofilms and cause recurring /
chronic immune activation during the invasion. This immune activation
inhibits specific mitochondrial metabolism and reconfigures a number of
other metabolic pathways toward combating these pathogens. However,
while ultimately beneficial, these alterations can be quite
debilitating, under certain conditions.
Consequences of fermenter overgrowth include small intestinal bacterial overgrowth (SIBO), leading to bloating, gas, and malabsorption in the upper gut. In the colon, lactate accumulation can excessively acidify the lumen, inhibiting beneficial species and potentially causing mucosal injury. Metabolic by-products from an over-fermenting microbiome, such as ethanol and ammonia, can burden the liver and impair cognitive function. Normal cross-feeding, where lactate and acetate from fermenters like Bifidobacteria or Lactobacilli are used by butyrate-producers, is disrupted, leading to the accumulation of intermediate metabolites.
A multifaceted approach is necessary to rebalance the microbiome in chronically ill patients, focusing on reintroducing or stimulating butyrate-producing species, providing appropriate substrates, potentially supplementing beneficial metabolites, and reducing fermentative overgrowth.
A phased approach for rebuilding the gut microbiome typically involves:
Phase 1 - “Clean Slate” (1-4 weeks)
If significant dysbiosis is suspected or quantified, measures to reduce pathogenic and fermentative load are initiated. After onboarding the standard protocol interventions to stabilise the metabolism, this may include a 7-14-day course of rifaximin or nifuroxazide for SIBO and/or 4+ weeks of herbal antimicrobials. Bacteriophages can be very helpful. A gentle, gut-friendly diet (e.g., low-FODMAP temporarily) is implemented concurrently to reduce fermentable substrates. Bowel regularity should be ensured.
Phase 2 - Reseeding and Feeding (Weeks 2-12)
This phase introduces probiotics and prebiotics. A high-quality multi-strain probiotic is started once antibiotics are completed, or concurrently if using antibiotic-resistant strains like S. boulardii. Prebiotic fibers, such as partially hydrolysed guar gum (PHGG), are introduced gently and increased gradually, aiming for 10-15 grams daily through diet or supplements. Oral butyrate supplements can also be slowly started and once well-tolerated, replaced with butyrate producing probiotics. The diet transitions to a more diverse, fiber-rich pattern, incorporating fermented foods cautiously. By the end of 3 months, some improvements are expected, but sustained effort may be needed for deeper shifts.
Phase 3 - Maintenance and Monitoring (3 months and beyond)
The focus shifts to maintaining healthy habits and potentially tapering supplements. A high-fiber, diverse diet should be continued indefinitely. Probiotics may be continued for 3-6 months or longer, possibly at lower maintenance doses. Butyrate supplementation and foods can be continued if beneficial. Objective markers like fecal butyrate levels and keystone microbial species, along with subjective improvements in stool form, bloating, energy, and cognitive function, are monitored. Setbacks due to new infections or medications are managed by temporarily adjusting the protocol.
Realistic expectations are important, as rebuilding the microbiome is a gradual process. Initial improvements in digestive comfort may be felt within 2-4 weeks. More robust changes, such as stabilised stool patterns and improving energy, are expected by 8-12 weeks. Long-term remodeling can take 6-12 months, potentially leading to increased activity levels and overall resilience. While not all core chronic illness symptoms may fully resolve, most patients can achieve improvements in gastrointestinal symptoms and nutritional status.
More information on each intervention can be found in related sections below.
Tailoring gut microbiome therapies for frail, home-bound patients is critical. Here are some of the key considerations:
#1 - Start Low and Slow
Introducing fibers, probiotics, or any supplement gradually (e.g., ¼ of the intended dose, increasing every few days) helps the gut adjust and prevents symptom exacerbation.
#2 - Hydration and Diet Texture
Adequate water intake is essential with increased fiber. Fibers can be incorporated into soups, purees, or powders for easier consumption if chewing or digestion is impaired.
#3 - Monitoring Nutritional Status
Repleting nutrient deficiencies (e.g., vitamin D, B12, magnesium, protein) before starting is critical for gut healing.
#4 - Contraindications
High-fiber diets should introduced slowly in cases of intestinal obstruction or stricture. Probiotics should be used cautiously and with medical clearance in severely immunocompromised patients or those recently post-surgery.
#5 - Herxheimer-like Reactions
Patients will likely experience transient "die-off" symptoms (fatigue, headaches, rashes) when the microbiome shifts. Slowing down the intervention or using supportive measures like binders may be helpful.
#6 - Bed-bound Logistics
Administering supplements (powders, open capsules) and enemas may require caregiver assistance and planning.
#7 - Medication Interactions
Be aware that medications like antibiotics, acid blockers, and opiates can affect the gut microbiome. Probiotics like Saccharomyces boulardii can be used during antibiotic courses.
Mammary glands and lactiferous ducts are present in both male and female anatomy. A less well-known fact is that males
are also capable of lactating under unusual circumstances that involve
low dopamine and elevated prolactin. These tissues are also another common area for microbial
biofilm formation.When diagnosed with an infection, this is known as
non-lactational mastitis.
Collecting any data on this microbiome is rather difficult when not lactating. It's possible that repurposing eg. MicroGenDX's WoundKEY panel could be useful, if a sample can be obtained.
For women, where biofilms in these microbiomes contain pathogenic species, it is expected that immune activity and inflammation in these (and any other infected) tissues will ramp up during oestradiol elevation, by allowing more IFN-gamma activity.
This immune activity elevation occurs as a short spike during pre-ovulation and for a range of days during the second half of the luteal phase, pre-menses. (see "2.2.7 Reproductive-health")
Sore and bumpy breasts during these times are common and inflammation may be observed in both the mammary glands and lactiferous ducts, with or without accompanying swollen inframammary, anterior axillary and parasternal lymph nodes.
While traditionally, many women have received advice about reducing oestradiol levels to prevent these symptoms, this logically leads to persistence of the infection.
Working with the body's natural signalling, while helping to manage the localised biofilm, oxidative stress and pathogens may help you break out of this unpleasant monthly cycle.
Topical use of 70% DMSO / 30% water (or 30% aloe vera gel), as a transport enhancer, combined with various biofilm breakers and anti-microbial interventions listed in this protocol may be an effective way to shorten this journey. This intervention can also be used with other tissues.
NB. DMSO is expected to create a localised histamine response when applied to skin, which will feel itchy for a short period. It's best applied with clean hands or gloves.
[source: Human Anatomy Atlas, by Visible Body.]
Parasites
Co-infections of flesh-eating parasites such as worms, flukes, amoebas, etc.,
can temporarily induce severe ME/CFS symptoms by directly attacking the
epithelial layer and allowing opportunistic invasion by any/all
microbial species.
Any of these can become systemic and create a chronic, recurring immune response in different tissues.
If you suspect you have a parasitic infection, over-the-counter
and/or prescription pharmaceutical interventions such as ivermectin,
fenbendazole, mebendazole, albendazole, methylene blue and pyrantel may be appropriate.
Some of these anti-parasitics also have anti-fungal and other
properties. This often applies vice-versa, too. These are commonly taken as either a single or multi-dose
intervention by all inhabitants of a household, per your pharmacist’s or
doctor’s advice.
For other species, such as amoebas, paromomycin and similar prescription drugs can be highly appropriate. Additionally, various herbal products based on black walnut, cloves and wormwood have also shown as highly effective, eg.
https://www.australianhealthfoods.com/product/ppc-herbs-herbal-tri-plex
The GI-Synergy product in Stage 2 already includes many of these ingredients.
(WIP: This section is being actively worked on to improve interventions for Bartonella, Borrelia, Babesia, Toxoplasma and some other species. Updates are coming.)
Profile: Toxoplasma gondii
Toxoplasma gondii is a protozoan parasite notable for its capacity to establish lifelong latent infection, often within neural and muscle tissues. Studies suggest over 50% of the population is infected. In immunocompetent hosts, it typically remains subclinical; however, its persistence in the central nervous system has drawn increasing attention due to its association with measurable alterations in behaviour and neurochemistry. Rather than eliciting overt pathology, the organism maintains a long-term presence through intracellular cysts, accompanied by a sustained, low-grade immune response that may itself become a source of chronic neuroinflammatory stress.
The host immune response is predominantly mediated by interferon-gamma (IFN-γ), which activates several downstream pathways, including the induction of indoleamine 2,3-dioxygenase (IDO) and tryptophan 2,3-dioxygenase (TDO). These enzymes degrade tryptophan, limiting parasite proliferation but also reducing serotonin synthesis and increasing production of neuroactive kynurenine metabolites. Microglial activation, mitochondrial dysfunction, and disruption of glutamate homeostasis have all been documented in chronic T. gondii infection, with potential consequences for synaptic regulation, oxidative stress, and overall neurotransmitter balance. Additionally, the parasite encodes tyrosine hydroxylase-like enzymes, enabling it to influence local dopamine synthesis directly within host tissue.
While the behavioural implications remain under investigation, multiple studies have identified correlations between latent T. gondii infection and alterations in fear processing, impulsivity, sexual behaviour, affective disorders, and suicidality in humans. These associations appear to be mediated by both direct biochemical interference and immune-driven changes in neurophysiology. Although causality is not uniformly established, T. gondii serves as a representative example of how persistent intracellular pathogens may exert long-term, system-wide influence on neuroimmune and metabolic function, particularly in people with existing co-infections and mineral deficiencies.
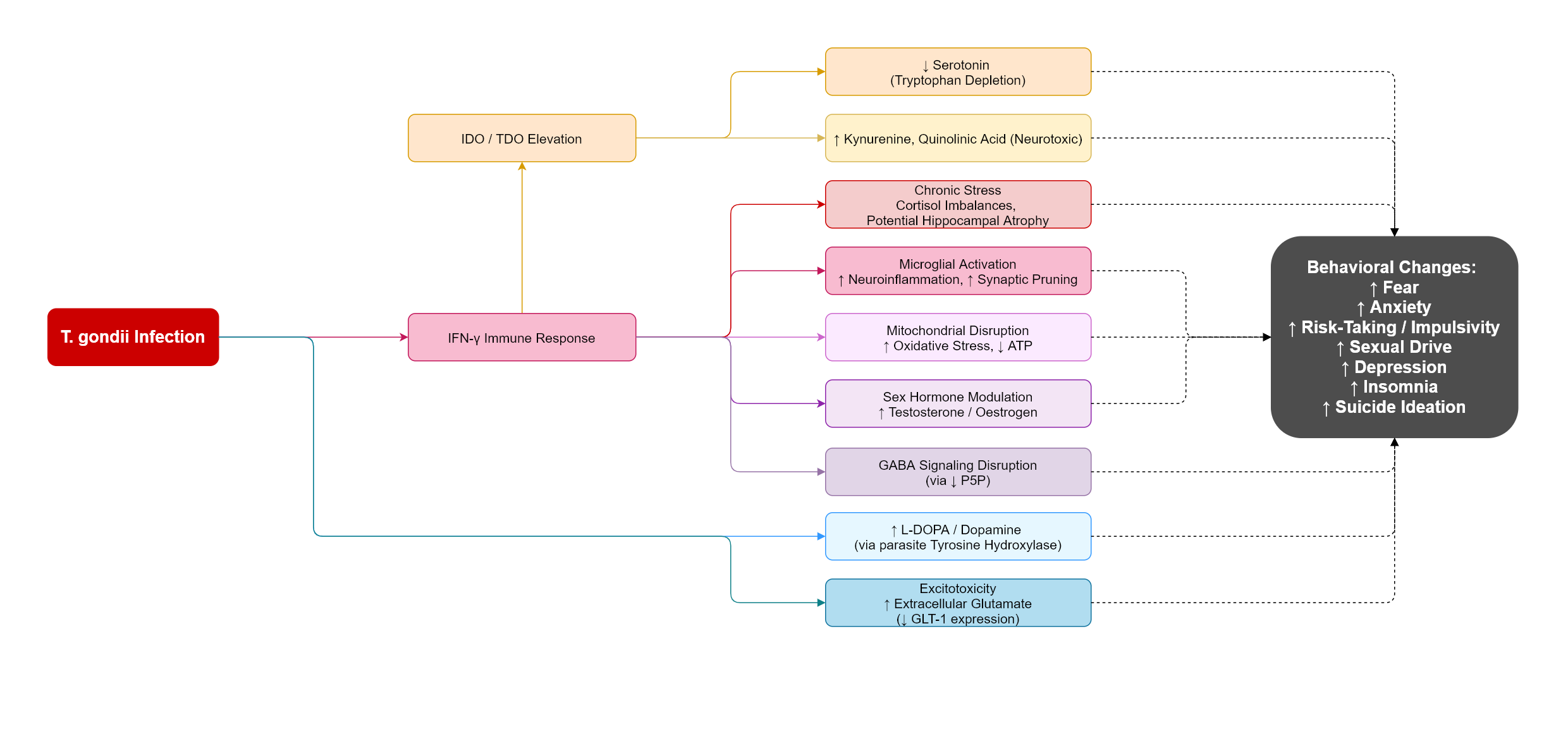
T. gondii infections in immunocompromised people may benefit from specific combinations of antimicrobials that target stategic parasitic proteins at different stages of the parasite's lifecycle - cysts, bradyzoites and tachyzoites. Some of these interventions may need to be rotated on a 3-5 day schedule to prevent parasitic adaptation.
NB. At this time, outside of correcting IFN-γ dysregulation, this parasite is not directly targeted by this protocol and is being actively investigated. There are some recent, encouraging studies using off-label medicines and various plant compounds which show high efficacy against some of the more difficult stages of the lifecycle.
Glycocalyx
The glycocalyx is a delicate, gel-like layer that coats the inner lining of blood vessels, forming a vital interface between circulating blood and the vessel walls. Though invisible to the naked eye, it plays an essential role in maintaining vascular health by regulating fluid balance, preventing the unnecessary leakage of substances, reducing friction between blood and vessels, and acting as a communication hub for immune signals. The integrity of this layer is critical for protecting the inner lining of blood vessels and supporting healthy organ function.
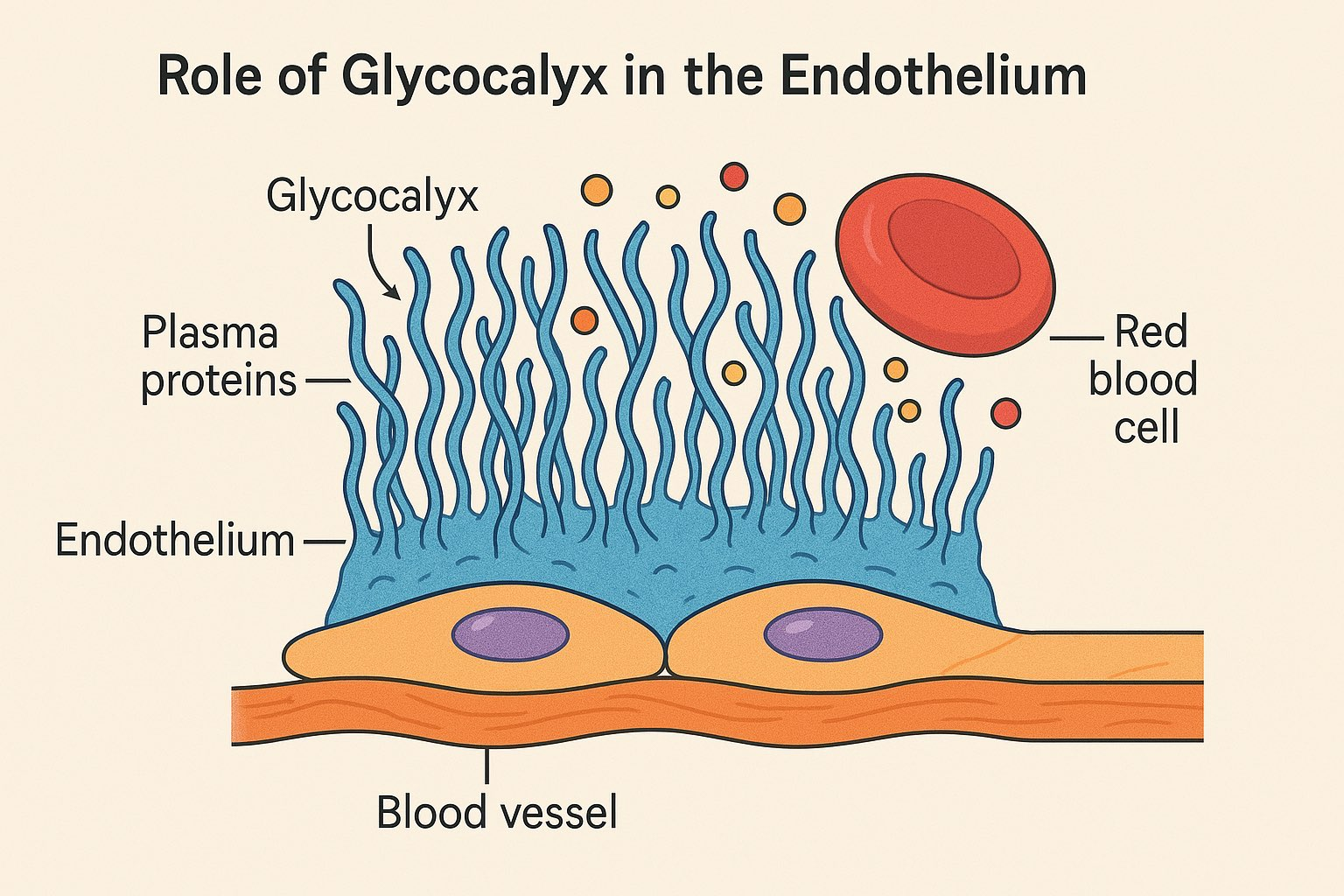
At its foundation, the glycocalyx is made up of complex sugar chains, proteins, and lipids. Its construction begins with basic nutrients: glucose provides the raw material for the long sugar chains called glycosaminoglycans, glutamine fuels the production of nucleotide sugars needed for building these chains, and methylation processes help regulate which parts of the sugar-protein scaffolding are modified or extended. This means that the body’s ability to synthesise a healthy glycocalyx relies directly on having sufficient energy, nutrient availability, and intact metabolic pathways.
However, in chronic diseases where metabolism is compromised, the body’s ability to maintain the glycocalyx begins to falter. In particular, when glycolysis - the process of breaking down glucose to produce energy, hepatic gluconeogenesis - the liver's ability to produce new glucose and Pentose Phosphate Pathway - which produces PRPP, are all disrupted, the raw materials and energy needed for glycocalyx upkeep become limited. This is especially problematic in conditions involving a persistent immune response, such as low-grade bacteremia, where bacteria or bacterial components circulate at low levels and chronically stimulate the immune system. The immune system, in turn, can damage the glycocalyx both directly and indirectly through the release of inflammatory signals and enzymes.
This sets up a vicious cycle. As the glycocalyx erodes, the tight
junctions between endothelial or mucosal cells become leaky. This
increases the permeability of blood vessels and mucosal barriers like
the gut lining, allowing more microbial fragments or toxins to pass
through, which further activates the immune system. With each cycle, the
body becomes increasingly inflamed and less capable of repairing the
very barrier that protects it. In this way, the health of the glycocalyx
becomes both a victim and a regulator of chronic disease processes,
especially in conditions marked by sustained inflammation, microbial
presence, and metabolic dysfunction. Preserving or restoring the
glycocalyx may therefore be a key strategy for breaking this cycle and
supporting overall recovery.
Where glycolysis is impaired, glycoalyx assembly can be supported by dietary sources of N-acetylglucosamine (GLcNAc, NAG) and hyaluronic acid (HA), however functional methylation and sufficient manganese, magnesium and phosphate are also required.
Human studies on NAG in Multiple Sclerosis and other diseases have shown favourable results.
NB. NAG is also beneficial to a range of helpful and unhelpful species, eg. Aggregatibacter actinomycetemcomitans, Akkermansia muciniphila, Arthrobacter bussei, Bacteroides caccae, Bacteroides thetaiotaomicron, Bifidobacterium bifidum, Bifidobacterium infantis, Bifidobacterium longum, Candida albicans, Enterococcus faecalis, Escherichia coli, Faecalibacterium prausnitzii, Hahella ganghwensis, Lactobacillus casei, Lactobacillus rhamnosus, Methanobacterium spp., Pseudomonas aeruginosa, Staphylococcus aureus and Streptococcus mutans. NAG dosing can be taken sublingually, if necessary.

One of the less visible yet deeply consequential ways the immune system can affect the glycocalyx involves the production of reactive molecules. In response to chronic infection or even low-grade bacterial presence in the bloodstream, the immune system normally ramps up interferon signaling. These interferons activate a set of enzymes that include inducible nitric oxide synthase (iNOS) and NADPH oxidase. These enzymes produce nitric oxide and superoxide, respectively - both reactive molecules that in balanced amounts help fight infection. But when produced in excess or under poor metabolic conditions, they can become damaging. Spirulina is a potent NADPH oxidase inhibitor. Curcumin and schisandra are also helpful. Low-dose dextromethophan is an over-the-counter anticholinergic that also acts as a NADPH oxidase inhibitor.
A crucial factor here is a molecule called tetrahydrobiopterin, or BH4. This cofactor is required for nitric oxide synthase (NOS) to properly generate nitric oxide. When BH4 levels are insufficient, which can happen during oxidative stress or nutrient shortages, NOS becomes "uncoupled" and instead of making nitric oxide, it generates more superoxide. This superoxide quickly reacts with any available nitric oxide to form peroxynitrite, a highly reactive and damaging compound. Peroxynitrite can attack lipids, proteins, and DNA, and the delicate glycocalyx is especially vulnerable to this kind of oxidative onslaught.
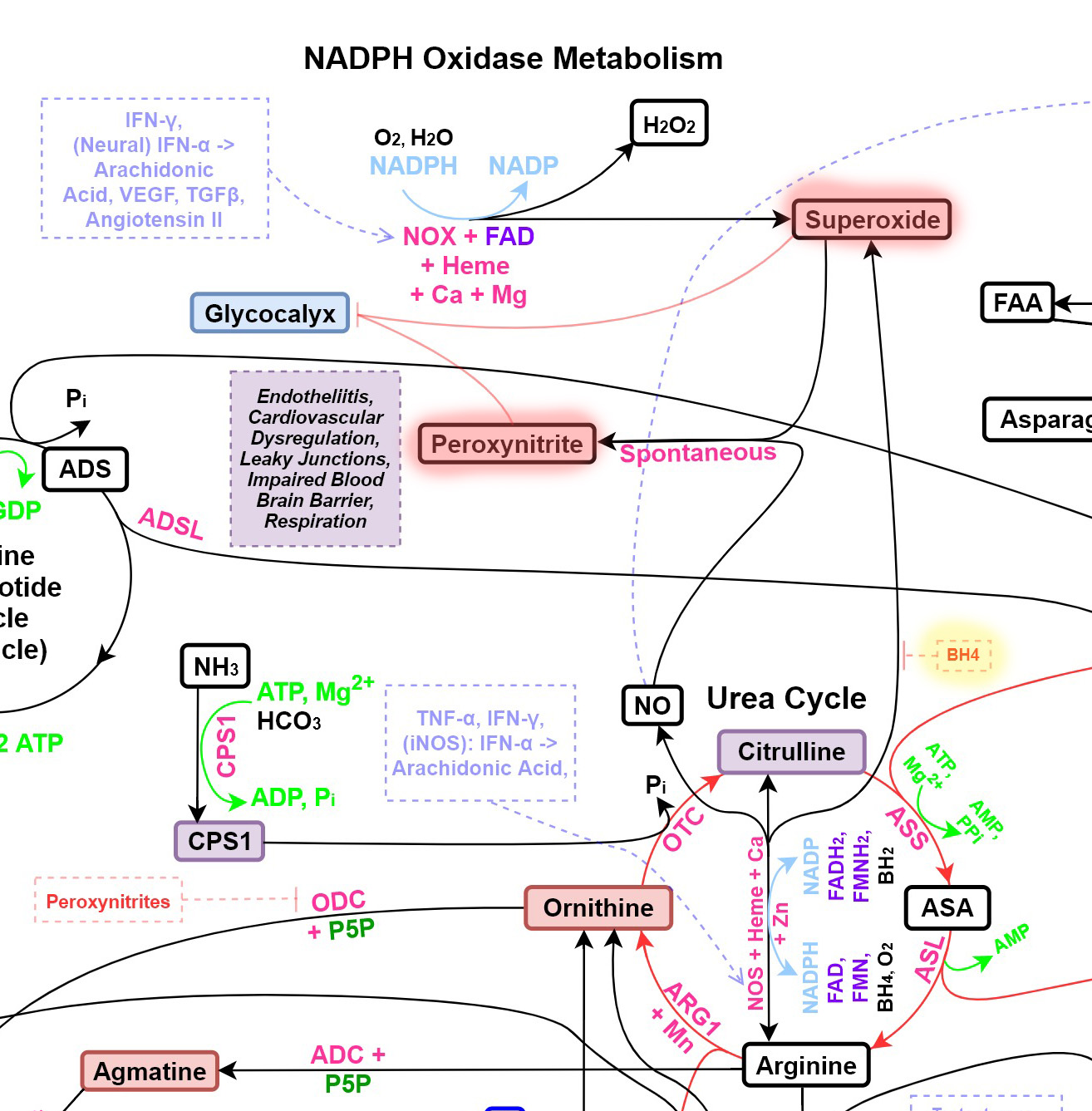
Compounding this problem is the state of the microbiome. A healthy microbiome contributes to the host in numerous ways, including the synthesis and salvage of rare micronutrients like queuine, a modified base that gets incorporated into human tRNA as queuosine. This modification supports proper mitochondrial translation and protein folding, and helps limit mitochondrial production of reactive oxygen species (ROS). When the microbiome is imbalanced or depleted, levels of queuine can fall, impairing mitochondrial function and allowing ROS to accumulate. These reactive species leak into the surrounding environment, adding to the oxidative burden that the glycocalyx must withstand. Rich sources of dietary queuine include coconut water (not heat-treated), wheat germ (gluten), milk (dairy).

In addition to oxidative stress, chronic inflammation also activates enzymes like matrix metalloproteinase-9 (MMP-9), which can directly degrade components of the glycocalyx and the underlying extracellular matrix. MMP-9 is particularly problematic in chronic immune activation, where its expression is upregulated by inflammatory cytokines and sustained by feedback loops involving ongoing tissue damage and immune signaling. As MMP-9 breaks down the structural scaffolding of blood vessels and mucosal linings, it exposes the underlying cells to further immune activation and microbial intrusion, continuing the cycle.
The end result of these overlapping pathways - interferon-driven enzyme activation, uncoupled nitric oxide production, mitochondrial stress due to micronutrient depletion, and enzymatic breakdown by MMPs - is a gradual but relentless erosion of the glycocalyx. Once this protective layer is compromised, not only does it lose its physical barrier function, but it also becomes less able to buffer mechanical forces, regulate immune signals, and maintain redox balance at the vessel surface. In this way, the glycocalyx becomes both target and amplifier of the chronic inflammatory state, linking microbial signals, metabolic strain, and immune dysfunction into another self-perpetuating loop. Ginger, berberine and doxycycline are all inhibitors of MMP-9.
Interventions
Whenever our interventions or immune system responses are successful in killing microorganisms, their death can cause “dumping” and circulation of these toxins which contribute to a well-known “die-off effect” occurring. This die-off effect is responsible for a number of highly debilitating symptoms, such as headaches, nausea, additional fatigue, dizziness, swollen glands, bloating / gas, constipation or diarrhoea, joint or muscle pain, tachycardia, chills, cold hands / feet, itchiness, rashes, sweating and/or fever which resembles the “disulfiram effect”. Read more here: https://www.thecandidadiet.com/candida-die-off-symptoms/
This cascade can cause an ongoing / recurring cycle of extreme unpleasantness, if these infections and their original “safe spaces” (biofilms) are not fully resolved and a protective microbiome restored.
We have been actively researching a combination of some innovative and existing strategies to help kill these microorganisms and minimise the die-off symptoms (see 2.3.1 Herxheimer / die-off / acetaldehyde support). Some additional challenges relating to biofilms, which provide further protection against our immune activities are also targeted.
In addition to the metabolic supplement schedule included in this protocol, a more rapid clearance of any (somewhat) accessible microorganisms may be achieved by direct or topical interventions for these infected tissues. Commercial preparations are available with various levels of efficacy.
However, the quality of your data will determine the quality of your results. Having known targets allows for precision interventions to be used, whereas having unknown targets leaves you no choice other than "throwing darts in a dark room, hoping one or more of them lands". With a competent immune system, targeting the biofilms allows the immune system to see the pathogens and throw precision "darts".
Binders
Area of effect: localised and systemic interventions exist.
Limitations: somewhat selective interventions - matching products with toxins is important.
Risk profile: "Final binders" are usually non-toxic, some binders can also bind to nutrients, such as minerals, causing deficiencies over a short time.
Silicol Gel, Enterosgel: Both of these readily-available products are non-absorbing silica-based gels that act as “sponges” for endotoxins / LPS / acetaldehyde and salts of heavy metals, backed by clinical trials. These are consumed around mealtimes or interventions that induce die-off, to mitigate the Herxheimer effect symptoms.
Zeolite: Zeolite is a natural volcanic mineral with a high affinity for binding heavy metals, environmental toxins, and radioactive isotopes. It acts as a molecular sieve, trapping toxins within its cage-like structure. Zeolite is non-toxic and passes through the body without being absorbed, making it a popular detox aid. It is often used in detox protocols to support the elimination of lead, mercury, and other harmful substances.
Bentonite Clay: Bentonite is a type of absorbent clay known for its ability to bind toxins, chemicals, and heavy metals. When hydrated, it swells and creates an electrical charge that attracts toxins like a magnet. It is often consumed mixed with water and is widely used for digestive issues, detoxification, and skin health. It can be especially useful after exposure to environmental toxins or as part of a regular detox regimen.
Diosmectite (Smecta): Diosmectite is a natural clay-based binder with potent adsorption capabilities, specifically targeting bacterial toxins, viruses, and harmful substances in the gut. It forms a protective layer over the gut lining, reducing inflammation and aiding in the healing of gut mucosa. Diosmectite is commonly used for gastrointestinal issues like diarrhea and leaky gut and can be helpful in reducing symptoms of food poisoning and infections.
Activated Charcoal: Activated charcoal is one of the most popular and widely available binders. It has a porous surface that traps toxins, chemicals, and gases, preventing their absorption into the bloodstream. Often used for acute poisoning or in situations involving gastrointestinal distress, it can also be part of regular detox protocols. It is taken in capsules or powder form and is effective in reducing bloating, gas, and Herxheimer reactions during detoxification.
Fulvic Acid: Fulvic acid is a natural organic compound found in soil and water sources. It has strong binding properties and can help chelate heavy metals and toxins, making them more water-soluble and easier to eliminate through the kidneys. Fulvic acid is also known for its ability to enhance nutrient absorption and support cellular detoxification. It is often consumed in liquid form as a supplement for detox and overall health.
Humic Acid: Humic acid is a large molecule that works alongside fulvic acid to bind heavy metals, glyphosate, mycotoxins, and other environmental toxins. Its complex structure allows it to act as a natural chelator, pulling toxins from the body and supporting liver and kidney detoxification. Humic acid is commonly used to help restore gut health and improve immune function.
Spirulina: Spirulina is a blue-green algae rich in nutrients and known for its detoxifying properties. It is particularly effective at binding to heavy metals such as mercury, lead, and arsenic, promoting their elimination from the body. Spirulina is often used as part of heavy metal detox protocols and can be consumed in powder or tablet form.
Chlorella: Chlorella, another algae, is renowned for its detoxifying capabilities, especially in binding heavy metals, pesticides, and other toxins. It contains a unique outer cell wall that traps and removes these substances from the body. Like spirulina, chlorella is used in detox protocols and is available in various forms, including tablets and powders.
Pectin: Citrus pectin, especially in modified form, is a powerful binder that helps remove heavy metals and environmental toxins. It works by binding to these toxins in the bloodstream and digestive tract, preventing their reabsorption and facilitating their excretion through urine. Modified citrus pectin is often included in protocols for reducing toxic burden, particularly for lead and mercury.
Chitosan: Derived from the shells of crustaceans, chitosan is a natural polymer that acts as a binder for fat-soluble toxins, heavy metals, and excess lipids. It has therapeutic effects against LPS. It is often used to support weight loss and detoxification by reducing the absorption of fats and toxins from the digestive system. Chitosan supplements are available in capsule form and can be helpful in detox protocols.
Cilantro (Coriander): Cilantro is a natural herb known for its ability to mobilize heavy metals, particularly mercury, from tissues. While it may not be as potent as synthetic chelators, cilantro is often used in combination with other binders like chlorella to promote the safe excretion of heavy metals. It is a common addition to natural detox protocols and is consumed as fresh leaves, tinctures, or supplements.
A number of these binders are already included in the protocol at different stages.
Bacteriophages
Area of effect: localised, replicating and systemic (nebuliser, IV).
Limitations: highly selective intervention - matching products with species and strain are important.
Risk profile: Non-toxic, can create die-off symptoms.
A bacteriophage is a virus which doesn't infect human cells, however it does infect and kill bacteria with high specificity,
unlike antibiotics. They've been studied for over a hundred years and
Russia is well-established as the world-leader in this area.. which makes things a little
tricky in 2024.
Bacteriophages have been studied against gut microbiome dysbiosis in long COVID, with positive results.
https://www.mdpi.com/1999-4915/14/12/2614
A little-known fact about bacteriophages is that they can be found in seawater in concentrations of up to 107 mL−1,
however this does not automatically mean that random doses of seawater
will contain the relevant bacteriophages that eg. match your collections
of pathogenic species.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7150976/
If you have data from a microbiome report that indicates particular species of pathogenic bacteria,
you may be able to use a bacteriophage product in that tissue to help
eliminate them - very, very selectively.
However, on the basis of various species
regularly appearing in different tissues, bacteriophage products are
also available which target a range of common pathogenic species. It's
possible you may need more than one product to target all of the species
reported in your data.
A product selection table and various product instructions translated from Russian to English are provided in 5 Bacteriophage lookup.
For
GI related targets, oral + rectal administration is recommended by
product manufacturers, presumably to avoid being degraded by stomach
acid.
The same W302 nebuliser mentioned in the DIY antiseptic recipe section is also appropriate for bacteriophage delivery to lungs and circulating targets.
Luer slip syringes can be used for other tissues / orifices.
NB.
Just like when using any other any other well-targeted anti-microbial,
die-off is expected. The more potent the anti-microbial, the larger the
wave of toxins you need to metabolise and/or excrete. Some support for
this can be found in 2.3.1 Herxheimer / die-off / acetaldehyde support.
DIY antiseptic recipe: mucosal clean and flush, rinse, topical spray
Area of effect: localised, with some systemic absorption / effects in some cases, eg. black seed oil.
Limitations: broad spectrum, can harm good and bad species. Requires follow-up probiotics.
Risk profile: Negligible toxicity, can create significant initial inflammation and die-off symptoms.
Popular antifungal soaps, shampoos and creams containing zinc pyrithione can be effective at inhibiting fungal overgrowth. However, these products are now banned in Europe due to concerns around causing DNA damage - warning: avoid.
Part of a successful "untargeted" intervention for these tissues may also include first administering a solution to break up any protective biofilms, leaving this solution to incubate for 20–30 minutes before (where possible / appropriate) wiping the area clean and then administering a second solution to selectively inhibit these foreign cells. These two solutions can also be applied simultaneously. The process may be repeated daily for 1–2 weeks, or as necessary.
Getting started:
Ongoing testing and literature review has suggested that a simple solution of NAC and hypertonic sodium bicarbonate water solution can reliably break up many biofilms and lyase cells. Breaking biofilms exposes any remaining microbes to immune surveillance and any other interventions you may explore. Using this recipe in a Neilmed Sinugator, douche or other appropriate tool can be a gentler way to start clearing biofilms and remodelling microbiomes, such as the nasopharynx and sex organs.
Further research has also suggested that a solution containing diluted tea tree oil, clove oil and other oils, when applied with or immediately following NAC yields a tolerable, yet significant inhibitory effect on bacteria, yeasts, moulds and fungi which may rival or exceed existing pharmacological interventions and is appropriate for a range of applications.
Commercial preparations made from tea tree oil and clove oil, are also readily available as shampoos, vaginal douches, topical sprays, mouthwashes, creams and suppositories.
Available from your local chemist, Neilmed make sinus washing products – such as “Sinugator” and “Sinus Rinse”, which can be highly effective at pre-rinsing these difficult-to-reach mucosal tissues, 20 minutes prior to application of any antiseptic products.
2g boric acid and 5–10 droops of Lugol's iodine can also be added to the Neilmed solution, for additional potency. A temporary smell of iodine and some burning / stinging would also be expected where infected tissues exist.
Note: Due to the die-off effect when killing fungi, using this antiseptic recipe while not using the other supplements from Stage 1 may be unnecessarily unpleasant and exacerbate symptoms.
| Part 1: Mix 500mg of NAC powder (preferably not from a capsule, as these usually have fillers, although these could also be filtered / strained after stirring), 500mg of sodium bicarbonate (baking soda), 1g of xylitol and >5 ml of water. |
| Part 2: Separately, mix essential oils – 20 drops of tea tree oil, 80 drops of black seed oil, 6 drops of oregano oil, 6 drops of clove oil, 1 capsule of Biofilm Phase 2 Advanced (BP2A). (You can add more black seed oil if you find this too strong and want to dilute the more potent / irritating oils further.) |
| Mix both parts together to form your final solution – allow a 2 week shelf life. Store in an empty glass bottle with a dropper for convenient dosing. Shake well before use. |
To test this as a nasal antiseptic: while laying on your back, with your head tilted back and breathing through your mouth, drip about 6 drops of the solution into each nostril.
Let the solution run into the nasopharynx and incubate for a minute or so, while you suffer through some shockingly unpleasant burning for a few minutes (the first time), assuming you have infected tissue. (See the experiences reported in the Discord server for more information.)
Healthy tissues won’t be irritated at this concentration, so if it "burns" – repeat this process every 1-3 days until irritation / inflammation is not observed. It will get progressively much easier.
Rotating your head slowly to each side and very gently “equalising” (like pinching your nose, gently exhaling through the nose against the close nostrils and "popping your ears", like on an aeroplane) with fluid in the nasopharynx may allow the solution to access the Eustachian tubes. (Performing the same in reverse and inhaling against closed nostril can evacuate the tubes, also.) After some time, blow / purge your nose, leaving some residue behind. A follow-up nasal probiotic may be very helpful after eg. 5-7 days of this, assuming there is no significant inflammation in response to the antiseptic.
To test this as a topical antiseptic: simply clean the area and then spray / apply the solution. A cotton tip could assist application to the ear canal or rectum (don’t use this in enemas).
To test this as a dental pre-rinse: apply a few drops to your tongue, teeth and gums, or more to gargle and spit. Wait a few minutes, then brush / floss as usual. Note: unpleasant flavour. Note: as an antiseptic, small amounts reaching your throat isn’t likely to cause toxicity, whereas drinking it intentionally could be harmful.
For sensitive tissues
Recipe 2:
Combine a “squirt” of Johnson & Johnson Baby Shampoo (it contains a gentle detergent and EDTA as a biofilm breaker. NB. We are currently exploring organic alternatives) ,
plus;
1 x "Neilmed hypertonic sodium sachet" (or a teaspoon of sodium bicarbonate / baking soda), for osmolality,
in 240mL of clean water.
This recipe makes a gentle, yet potent, biofilm breaking intervention that can be used in a Neilmed Sinugator/Sinus Rinse tool, vaginal douche, Waterpik, etc.
Alternatively, you can also make another DIY rinse recipe:
Recipe 3:
Per 500mL of boiled / cooled water -
Mix 5g of sodium bicarbonate (baking soda) with 5g NAC. This allows an acid:base reaction (and gas release) to occur, which helps create a pH balanced solution.
This can then be combined with ¼ teaspoon of boric acid (making a 1½–2% solution) and 10 drops of the 5% Lugol’s iodine or 25 drops of 2% Lugol’s iodine.
To administer recipe 2 or 3:
- Eyebath: Use 30mL of the solution to bathe each eyeball, also cleaning the eyelids, lashes.
- Urethra: Administer 5–30mL of the solution via a large (needleless, Luer slip) syringe to the opening.
- Vagina: Administer 50-120mL, using a suitable douche tool or syringe and keep your hips and legs elevated for 30 mins.
- Lungs: (Use "Recipe 3" only) Administer 1-3mL via a drop-feed ultrasonic nebuliser, such as a "W302", found in most online marketplaces
- Sinuses, Eustachian tubes: This recipe can also be added to the Neilmed Sinugator reservoir.
The colostrum from Stage 2 can also be successfully used in mucosal tissues to neutralise unwanted species, antigens, etc.
Rotating between the “potent” recipe and the “gentle” recipes for 1–2 days is recommended if intense inflammation for more than 30 minutes is experienced. Continue with the nasal probiotics from the next section once an inflammatory response can’t be provoked by the normal antiseptic recipe.
Other simple and effective tools:
60-70% ethanol, as eg. rubbing alcohol or hand sanitiser, is also a well-known broad-spectrum, highly penetrative, highly indiscriminate intervention that can be used effectively in small amounts against viruses, bacteria, fungi and parasites on externally accessible tissues. In one RCT, where healthcare workers colonised with nasal S. aureus were swabbed intranasally three times daily with 70% ethanol plus natural oil emollients and benzalkonium chloride, they reported a median 99% reduction in CFU and no adverse effects during the study. From personal experience, it will feel temporarily "warm" and briefly quite unpleasant on broken or inflamed tissue and can be potentially damaging, if overused. Caution is also needed with ocular tissue - alcohol will cause damage.
Regardless of the recipe used, strong die-off effects can be expected the first time and should only be implemented after sufficient metabolic and detox support supplements are added in Stage 1 of the protocol / pre-protocol support.
Links to ingredients and tools mentioned can be found in the "5 Ordering products" section.
Biofilm breakers
Area of effect: some are localised, others are systemic.
Limitations: does not directly kill microorganisms - requires immune activity, probiotic species and/or other interventions to eliminate the species inside. Different biofilm compositions respond to different biofilm breakers - more than one may be required in chronic diseases with more than one pathogen indicated.
Risk profile: usually broad effects on biofilms for both good and bad species. Can trigger elevated immune activity and redistribution of microorganisms. If misused or overused, can damage microbiome diversity and abundance profiles.
Biofilm Phase 2 Advanced (BP2A): a localised bismuth-thiol biofilm breaker. Doesn't absorb. Included in Stage 2 and DIY antiseptic recipe.
NAC: a systemic biofilm breaker, particularly at higher doses.
Glutathione: a systemic biofilm breaker, particularly at higher doses.
Fulvic acid / humic acid: a systemic biofilm breaker, even at lower doses.
R-Alpha lipoic acid: a systemic biofilm breaker and metal chelator, particularly at higher doses.
Soap / detergent: a localised biofilm breaker, when used externally.
Ethylene Diamine Tetraacetic Acid (EDTA): a localised biofilm breaker and metal chelator, usually supplied bound to an electrolyte or mineral. Doesn't absorb well, orally - 5%. Can be used IV for circulating biofilms.
Dimercaptosuccinic acid (DMSA): a systemic biofilm breaker and metal chelator. Doesn't absorb well, orally - 25-30%. Can be used IV for circulating biofilms.
Dimercaptopropane-1-sulfonic acid (DMPS): a systemic biofilm breaker and metal chelator. Can be used orally or IV.
Microdacyn / hypochlorous acid: a localised biofilm breaker. Some absorption.
Ethyl acetate: a systemic biofilm breaker, even at very low doses. Found in robusta coffee and various acetone-free nail polish remover products.
Silver: a systemic biofilm breaker, even at very low doses.
Compounds found in foods: Allicin (Garlic), Curcumin (Turmeric), Epigallocatechin gallate (Green tea), Quercetin (Onions, Apples), Resveratrol (Grapes, Red wine), Eugenol (Cloves), Cinnamonaldehyde (Cinnamon), Sulforaphane (Broccoli, Brussels sprouts), Apigenin (Parsley, Celery, Chamomile), Berberine (Goldenseal, Barberry), Thymol (Thyme, Oregano), Carvacrol (Oregano, Marjoram), Fisetin (Strawberries, Apples), Linalool (Coriander, Lavender), Gallic acid (Blueberries, Pomegranates), Cinnamic acid (Honey, Cinnamon), Citric acid (Citrus fruits), Naringenin (Citrus fruits), Rosmarinic acid (Rosemary, Basil), Catechin (Cocoa, Dark chocolate), Ellagic acid (Pomegranates, Raspberries), Diallyl disulfide (Garlic), Capsaicin (Chili peppers), Piperine (Black pepper), Hydroxytyrosol (Olive oil), Xylitol (Berries, Plums), Isothiocyanates (Kale, Mustard greens), Ferulic acid (Rice bran, Oats), Kaempferol (Spinach, Kale), Pterostilbene (Blueberries), Saponins (Beans, Legumes), Chlorogenic acid (Coffee, Potatoes), Luteolin (Peppers, Carrots)
Probiotics: many of the probiotic species included in the protocol have potent functions as biofilm degraders and inhibitors. (see "Protective probiotics").
A number of these biofilm breakers are already included in the protocol. Overall, biofilm breakers should be considered an integral part of any microbiome dysbiosis or infection intervention and food sources should be included in any dietary strategy.
There are some additional strategies being tested which may feature in future updates, for example:
Upper GI biofilm flush, bind and purge recipe (advanced):
This a 3 step process, with similarities to a colonoscopy prep or gallbladder flush procedure. This
is not intended to ever be used a daily routine, as this intervention is
significantly broad spectrum and is highly destructive to the entire microbiome in the
upper GI. It would be used in limited circumstances only.
Step 1
contains a potent mix of biofilm breakers and anti-microbials, plus
some starch and warm water. Some of these items are not normally
consumed, however they are successfully used for pre-faecal microbiome
transplant (FMT) procedures. The mixture of anti-biofilm and
anti-microbial interventions is
adapted from Dr Thomas Borody’s excellent pre-FMT biofilm flush protocol and uses 2g biocompatible detergent (baby shampoo), 4mL of 1% iodine and 50mL Microdacyn).
The biofilm
flush recipe adaptation includes some additional items - an extra
biofilm degrader (ethyl acetate, from 2 shots of ground robusta coffee), 1 spoonful of diatomaceous
earth as a bulking agent and binder, along with an optional (opened) capsule of cascara to irritate / stimulate the bowels and increase GI motility. All of
these items are added to an empty glass and half a glass of hot water is
stirred in.
3 large spoonfuls of sifted potato starch (to prevent clumping) slowly stirred in to make a
rubbery mass that helps dislodge and drag / sweep along the broken biofilms. Fill the remaining part of the glass with cool water.
(This delightful concoction needs to be consumed quickly, or it'll polymerise in the glass.)
Step 2,
20 mins later - binders to help absorb toxins instead of allowing them
to circulate, which was a concern with the original pre-FMT protocol.
This next step includes a generous mix of binders, being 1/2 tablespoon of charcoal, 1/2 tablespoon of zeolite, 1/2 tablespoon of pectin and
1/2 tablespoon ofslippery elm powder, mixed into a glass of water.
Step 3,
20 mins later - this functions just like a colonoscopy prep or
gallbladder flush recipe. A large amount of electrolytes (Epsom salts / magnesium
sulphate) and lots of water are consumed. The large volume of magnesium
sulphate draws water into the bowel and purges the contents in a predictably dramatic fashion.
Add 1 teaspoon of Epsom salts (magnesium sulphate) to a glass of water. Stir until dissolved and consume.
Repeat this step 2 more times - 60 and 120 minutes later.
Overall, this allows the original biofilm breaking concoction from Step 1 around 40 minutes of travel throughout the GI tract, before being chased and diluted by the flush, reducing the impact of the biofilm breakers on the remaining length of bowel. It can potentially be adapted around the timing of peak gas output during a SIBO breath test, or reactivity timing to food.
Expect some unpleasant die-off symptoms / herxheimer-style reactions,
diarrhoea, nausea shortly afterwards. Exclusive bathroom access would be advisable for the next 12-18 hours.
Step 4, 12-24 hours later - consume S.boulardii, Bifidobacteria and Lactobacillus probiotics + prebiotics, related foods.
This flush could be performed
1-3 times, if
severe upper GI overgrowth exists, as evidenced by reactions to food in
under 1 hour. Excessive use of this recipe would NOT be recommended.
Protective probiotics
Area of effect: localised, however can translocate to other tissues.
Limitations: probiotics may not provide a comprehensive solution in isolation.
Risk profile: Non-toxic, can create significant die-off symptoms. The literature suggests some species can be opportunistic pathogens in highly immunocompromised people.
Following on from any efforts in clearing unwanted biofilms and microbial species overgrowth in the eyes, sinuses, nasopharynx, mouth, throat, oesophagus, lungs, GI tract, vagina, urethra and other mucosal tissues, further restorative efforts are usually needed in repopulating these tissues with helpful species to promote and maintain a healthy microbiome. (Links to these products can be found in the “5 Ordering products” section.)
These helpful species assist in inhibiting unwanted species, degrading biofilms and preventing opportunistic growth. They can also provide helpful functions, such as metabolism of oxalates, acetaldehyde, histamine, plus production of short chain fatty acids and other compounds beneficial to humans. Please note inclusion of these probiotics are based on an observed pattern of
diversity loss and are included for specific functions, to generally
promote a healthier balance in the microbiome, when combined with remineralisation and dietary changes.
They are not intended to replace MARCoNS, vaginal swabs, “GI-MAP” or Biomesight gut microbiome tests.
Many of these species were traditionally found in the Bacillus, Lactobacillus and Bifidobacterium genus, although recent taxonomy changes have relabeled / reclassified some of them, providing some minor confusion when researching species.
Bacillus subtilis:
Key Mechanism: Produces enzymes and antimicrobial compounds that degrade biofilms.
Notable Features: Spore-forming bacterium, resilient and able to survive harsh conditions, which allows it to act more potently against biofilms.
Effective Against: Both Gram-positive and Gram-negative bacteria.
Additional Benefits: Supports overall gut health and resilience against environmental stressors.
Lactobacillus fermentum ME-3:
Key Mechanism: Produces glutathione (antioxidant), disrupts pathogenic biofilms, reduces oxidative stress.
Notable Features: Dual-action as a biofilm breaker and antioxidant producer. Glutathione production sets it apart from many other probiotics, as it supports cellular detoxification.
Effective Against: Harmful gut pathogens and biofilm-forming bacteria, also including H. pylori..
Additional Benefits: Supports immune function, reduces inflammation, and has cardioprotective effects.
Lactobacillus reuteri:
Key Mechanism: Produces reuterin, a powerful antimicrobial compound that breaks down biofilms.
Notable Features: Strong antimicrobial activity, especially effective in the oral cavity and gut.
Effective Against: Pathogens like E. coli, H. pylori, and oral biofilm formers.
Additional Benefits: Promotes oral and gut health, reduces inflammation.
Lactobacillus rhamnosus:
Key Mechanism: Produces bacteriocins and SCFAs, which inhibit biofilm formation.
Notable Features: Excellent at inhibiting gut biofilms and maintaining gut balance.
Effective Against: E. coli, Pseudomonas aeruginosa, and other biofilm-producing pathogens.
Additional Benefits: Supports immune system, often used in combating gastrointestinal infections.
Lactobacillus plantarum:
Key Mechanism: Produces hydrogen peroxide and antimicrobial peptides that break down biofilms.
Notable Features: Broad-spectrum biofilm inhibition, active in the gut and oral cavity.
Effective Against: Gut and oral pathogens, including Candida and Staphylococcus aureus.
Additional Benefits: Improves digestive health, supports immune system function.
Lactobacillus casei:
Key Mechanism: Disrupts biofilms through production of bacteriocins and lactic acid.
Notable Features: Particularly effective against Helicobacter pylori biofilms in the gut.
Effective Against: H. pylori and other gut pathogens.
Additional Benefits: Supports digestive health, beneficial in addressing stomach ulcers.
Bifidobacterium bifidum:
Key Mechanism: Produces SCFAs like acetate, which create an acidic environment that disrupts biofilms.
Notable Features: Prevents biofilm formation by pathogenic bacteria in the gut.
Effective Against: Pathogens like Clostridium difficile and other harmful gut bacteria.
Additional Benefits: Supports overall gut health, improves digestion and immune system.
Bifidobacterium longum:
Key Mechanism: Like B. bifidum, B. longum produces SCFAs that lower the pH in the gut, which can inhibit biofilm formation. It also promotes the production of antimicrobial peptides and enzymes that disrupt pathogenic biofilms.
Notable Features: One of the most common Bifidobacterium species in the human gut, B. longum is well-adapted to the gut environment and plays a crucial role in maintaining microbial balance. It is especially good at outcompeting pathogenic bacteria.
Effective Against: Effective against a range of harmful bacteria, reducing biofilm formation in the gut.
Additional Benefits: Enhances immune function and promotes gut health, further protecting against biofilm-related infections.
Bifidobacterium lactis:
Key Mechanism: B. lactis can modulate immune responses, leading to the production of compounds that degrade biofilms or prevent their formation. It also produces lactic acid and acetic acid, which inhibit the growth of biofilm-forming pathogens.
Notable Features: Known for its resilience in the gastrointestinal
tract, B. lactis is widely used in probiotic supplements due to its
strong ability to survive stomach acid and bile. It's particularly
effective at adhering to the gut lining, enhancing its biofilm
prevention capabilities.
Effective Against: Has shown effectiveness in reducing biofilm formation by Escherichia coli and other gut pathogens.
Additional Benefits: Improves gut barrier function and promotes overall digestive health.
Bifidobacterium breve:
Key Mechanism: B. breve produces metabolites that interfere with pathogen adhesion and biofilm formation. It can inhibit the colonization of harmful bacteria by promoting a balanced gut microbiome and maintaining a lower gut pH through lactic acid and acetate production.
Notable Features: B. breve is one of the earliest colonizers of the human gut in infancy, making it especially important in the development of a healthy microbiome. It plays a significant role in maintaining gut integrity and has strong antimicrobial activity against pathogens.
Effective Against: Effective against Clostridium difficile and other gut pathogens that form biofilms.
Additional Benefits: Helps alleviate symptoms of gut dysbiosis, supports digestion, and reduces inflammation in the gut.
Bifidobacterium adolescentis:
Key Mechanism: Produces SCFAs and antimicrobial peptides that help prevent pathogenic biofilm formation. B. adolescentis can also enhance gut mucosal immunity, providing an additional layer of protection against biofilm-forming bacteria.
Notable Features: B. adolescentis is prevalent in the adult gut and plays a crucial role in breaking down complex carbohydrates, contributing to overall digestive health. Its ability to stimulate immune cells makes it particularly effective in preventing gut infections.
Effective Against: Reduces biofilm formation by pathogens in the gut, such as Salmonella and Escherichia coli.
Additional Benefits: Supports the immune system, promotes gut health, and reduces inflammation.
Saccharomyces boulardii:
Key Mechanism: Inhibits biofilms and outcompetes pathogens in the gut.
Notable Features: Effective against Candida and Clostridium difficile biofilms. Not susceptible to antibiotic influence.
Effective Against: Fungal pathogens and gut pathogens, particularly in cases of infection or dysbiosis.
Additional Benefits: Supports gut health, reduces diarrhea and inflammation, commonly used in traveler's diarrhea prevention.
Also potentially helpful is Oxalobacter formigenes, as an oxalate degrading species. When present in the small intestine, it also signals the host to secrete oxalates into the gut, instead excreting them via the kidneys. However, acidemia will override this.
Bifidobacterium are largely pH sensitive. You will have difficulties in restoring diversity and abundance while lactic acid metabolism is overused and zinc is low (hypoxia, impaired glycolysis, low minerals, anxiety disorders). Your OAT results should help indicate if lactic acid (+ oxalates) markers are elevated or the lactic acid : pyruvic acid ratio is elevated.
Studies and dosing information for these microorganisms in different mucosal tissues can be found on the Discord online discussion group and/or the literature. This protocol currently includes a number of key probiotics relating to these studies and their described functions / benefits:
- Life Extension Florassist: (Oral microbiome)
Probiotics - BLIS M18 S. salivarius M18, L. plantarum L-137 - DrFormulas Nexabiotic for Women: (Acid resistant capsule)
PaCran®SP (Cranberry fruit 50:1 extract), D-Mannose,
Probiotics - Saccharomyces boulardii, Lactobacillus helveticus, Lactobacillus delbrueckii LE, Enterococcus faecium, Bifidobacterium bifidum, Bifidobacterium longum, Bacillus coagulans, Lactobacillus rhamnosus LB3, Lactobacillus plantarum LM, Lactobacillus acidophilus, Lactobacillus rhamnosus, Bifidobacterium animalis lactis (formerly named Bifidobacterium infantis), Lactobacillus fermentum, Lactobacillus gasseri, DE111® (Bacillus subtilis), Lactococcus lactis, Lactobacillus casei, Lactobacillus salivarius, Lactobacillus brevis, Lactobacillus reuteri, Streptococcus thermophilus, Bifidobacterium lactis, Low moisture rice dextrin, delayed release capsule (hydroxypropyl methylcellulose, pectin, and water), silica. Allergen warning: Contains milk. - DrOhhira RegActiv Essential ME-3: (Survives stomach acid.)
Probiotics - Lactobacillus fermentum ME-3®, maltodextrin, magnesium salts of fatty acids (anti-caking agent). Vegetable capsule (hydroxypropylmethylcellulose). - CFUful 300 Billion CFU: (Acid resistant capsule)
Probiotics - Bifidobacterium longum BB536, Bifidobacterium longum HRVD90b, Bifidobacterium breve BR3, Bifidobacterium breve HRVD521, Lactiplantibacillus plantarum LP1, Lacticaseibacillus rhamnosus LR6, Lacticaseibacillus rhamnosus HRVD113, Lacticaseibacillus rhamnosus GG, Bifidobacterium infantis M63, Bifidobacterium lactis BS5, Bifidobacterium lactis HRVD524, Bifidobacterium lactis SD150, Lactobacillus crispatus LCR01, Lacticaseibacillus casei HRVD300, Limosilactobacillus fermentum LF8, Lactobacillus reuteri RD830, Lactobacillus acidophilus, Ligilactobacillus salivarius LS1, Bifidobacterium longum CECT7347, Lactobacillus casei CECT9104, Bifidobacterium bifidum, Lactiplantibacillus plantarum LPLDL, Bifidobacterium lactis MB2409.
Prebiotics - Fructooligosaccharides (FOS), Organic Barley Grass Powder, Organic Wheat Grass Powder, Organic Alfalfa Grass Powder, Organic Oat Grass Powder, Organic Beet Juice Powder, Organic Spinach Powder, Organic Suma Root Powder, Organic Licorice Root Powder, Organic Dandelion Root Powder, Organic Astragalus Root Powder, Organic Milk Thistle Seed Extract, Organic Ginkgo Leaf Extract, Organic Bilberry Extract, Organic Ginger Root Powder
- General Biotics Equilibrium Boost MegaDose Probiotic: (2 x acid resistant capsules per container.)
Probiotics - 115 strains, which have their own page, here - https://www.generalbiotics.com/equilibrium/strains/ - Ochek: (Only needed if indicated as missing in gut microbiome data. Promoted by dietary oxalates.)
Probiotics - O. formigenes, L. acidophilus, L. rhamnosus, B. lactis
Prebiotics - FOS - Pendulum Metabolic Daily: (Butyrate producers. Akkermansia promoted by pomegranate.)
Probiotics - Clostridium butyricum WB-STR-0006, Clostridium beijerinckii WB-STR-0005, Bifidobacterium infantis, Anaerobutyricum halii WB-STR-0008, Akkermansia muciniphila WB-STR-0001 - (Various sources, Kimchi) - L. sakei: (Anti-microbial. Also used in food production to prevent spoilage, etc.)
Probiotic - Lactobacillus Sakei
For example:
Nostrils: cotton tip / fingertip and apply inside the nostrils. Eustachian tubes: place drops of liquid into the nose and use the “equalisation” technique.
Mouth / throat / oesophagus / upper GI: gargle and swallow.
Lungs: nebuliser, 1-2 mL.
Vagina: add to a 5ml vaginal douche and elevate hips/legs for 15 minutes, while laying down, or place recently moistened, unopened capsule deep into fornix and allow it to dissolve.
Lower GI tract: use a probiotic rectal syringe (no tip) with <50mL of water, then “down dog” yoga pose for 15 mins to bypass stomach acid. Achieves a similar colonisation rate to FMT.
Eyes: place drops of liquid into the corners of the eyes and / or under the eyelids.
Prebiotics
Area of effect: localised, with systemic benefits.
Limitations: can be highly selective for promoting helpful species, if well-selected.
Risk profile: Non-toxic, can create die-off symptoms. Can promote unwanted species, if poorly selected.
You cannot solve dysbiosis by probiotics alone. Strategically feeding your microbiome and correcting symbiotic host metabolism, via remineralisation, etc. is the best way to make any lasting transformations. If you've ever made yoghurt, you'll have a good understanding of just how rapidly 2L of milk can turn into a (probiotic) fermentation product. 8 - 12 hours can turn eg. 2L of milk into 2L of yoghurt with just a spoonful of starter culture / microorganisms.
Your GI tract is no different, in this respect. Your choice of foods (substrates) allows you to achieve some selectivity in the species being fed and promoted. What you eat matters.
Inulin + fructooligosaccharides (FOS) are types of soluble fiber found in a variety of plants. Some common food sources include:
Chicory root (one of the richest sources), Jerusalem artichokes, Garlic, Onions, Leeks, Asparagus, Bananas, Dandelion greens, Wheat
Galacto-oligosaccharides (GOS)
is often added to foods as a prebiotic fiber, but it is also found in
trace amounts naturally in certain foods. Some food sources include:
Human breast milk (high content of GOS), Cow's milk, Lentils, Chickpeas, Green peas, Soybeans
Resistant starch is a type of starch that resists digestion and feeds beneficial gut bacteria. Common sources include:
Green
(unripe) bananas, Cooked and cooled potatoes (cooking and cooling
increases resistant starch), Cooked and cooled rice, Oats, Legumes
(lentils, chickpeas, beans), Barley, Corn
Polyphenols are compounds found in many fruits, vegetables, and beverages. Some common polyphenol-rich foods include:
Berries
(blueberries, strawberries, raspberries), Pomegranates, Cranberries,
Dark chocolate (high in cocoa content), Green tea (especially rich in
EGCG), Red wine, Olive oil, Nuts (walnuts, almonds), Herbs and spices
(turmeric, cloves, oregano)
These should be considered as high priority food items to introduce when planning your diet. However, they'd be expected to create some die-off reactions, gas and digestive discomfort at first. (see "2.2.1 Diet" for information on food items which also includes prebiotics)
Herbal Anti-microbials
Area of effect: localised and systemic
Limitations: may have broader effects on metabolism.
Risk profile: over-the-counter, generally regarded as safe. Can create significant initial die-off symptoms. Can alter drug metabolism.
There are a number of very effective and highly selective, plant-based anti-microbial products / foods.
Some of these interventions can simultaneously promote good species at the same time as inhibiting unwanted species. These would ideally be introduced in Stage 2 and will relate to your microbiome report data.
Notes:
Vanillin is often used at 2g, 2x per day and has been shown to kill sulphur-reducing and other unwanted species, however these species can be producing metabolites which have an antidepressant-like effect. Removing these species can create antidepressant-like 'rapid withdrawal' symptoms for up to 2 weeks.
Allicin has a particularly potent Minimum Inhibitory Concentration (MIC) for H. pylori, Candida spp., Porphyromonas gingivalis, Prevotella intermedia, Enterococcus faecalis, Clostridia spp. and Escherichia coli.
Resveratrol has broadly beneficial effects at 300-600mg, 3x per day, but can inhibit aldehyde dehydrogenase activity, especially in larger doses.
Short-chain fatty acids (SCFAs) such as butyrate can have highly positive effects on the microbiome and epithelium, however can create significant alterations which induce multi-day long die-off. Starting slowly is advisable.
Quercetin has many beneficial effects, but can inhibit aldehyde dehydrogenase activity, especially in larger doses.
Berberine has potent effects against Clostridia, but has similarly potent effects on enhancing fatty acid transport at CD36 and inhibiting mitochondrial complex 1. May not be well tolerated by some people, especially before Stage 2.
Here is a table of direct and indirect promoters and inhibitors, by genus / species (sorry, this table is too large for mobile and tablet screens):
A highly potent, combination herbal anti-microbial product is available called GI-Synergy. It features many of the interventions listed in the table above. It would be advisable to start slowly and work up to a full dose, in Stage 2.
(Prescription-based interventions and other options)
Area of effect: some are somewhat localised, however usually systemic.
Limitations: highly non-selective and broadly harmful to many species - good and bad. Antibiotic resistance can be created.
Risk profile: may harm mucosal tissues. May inhibit host metabolism. Can create potent die-off symptoms. Requires probiotics, prebiotics and dietary optimisation to prevent deleterious effects on microbiomes. Creates risk for fungal overgrowth, if not combined with anti-fungal interventions.
It’s expected that for “PSSD” symptoms that a UTI or sex organ infection may be present. With good data and a discussion with your doctor, specific antibiotics may be appropriate to treat an indicated infection, as these tissues are difficult targets, especially in males. Bacteriophages may also be an option for many cases.
Once you have collected quality data, you should be empowered to make better decisions around how to move forward. To assist this process, a database of pathogens and overgrowth vs interventions is being developed to help you decide what the best course of action is and will grow, over time. Most of these inhibitors are prescription antibiotics that require a discussion with your doctor, who can also advise you on the risks and benefits of pairing any antibiotic use with anti-fungal medications like itraconazole and fluconazole, to prevent the opportunistic overgrowth of fungal species during any significant microbiome remodelling. Careful attention will also be needed towards probiotics, prebiotics and diet.
Ideally, any antibiotics and anti-fungal interventions would not be started until Stage 2, or very late in Stage 1, if some urgency is required.
For further information on prescription antimicrobials, their mechanisms and effects on human metabolism, you can explore our Antimicrobial Library.
The table below will hide columns on smaller screens. You can use complete or partial words eg. "kleb" or "Klebsiella" for searching genus, species or inhibitors.

When a person is chronically ill and confined to their bed / house, the transfer of pathogenic microbes from their body to their surroundings becomes a significant concern. Pathogenic microbes can transfer easily from the body to the environment and back again, causing an ongoing challenge to an already compromised immune system.
One of the primary concerns is the transfer of pathogenic microbes to the bed, pillows, sheets, and mattress. These surfaces can harbour pathogens and continue a cycle of infection.
Bed linen – sheets, pillowcases, and blankets – should be changed frequently and washed in hot water, with a hygienic detergent to kill any pathogens present and arrest the cycle of reinfection.
Mattresses and pillows should also be rotated and disinfected regularly. A waterproof mattress protector can also help prevent the accumulation of moisture and bacteria. These will also need regular cleaning.
Another concern is the transfer of airborne pathogens through air conditioning systems. Air conditioning systems can spread pathogens throughout a room, increasing the risk of infection. It is important to clean / change the air filter frequently and consider using an air purifier to help remove pathogens from the air.
Wet areas are a common issue - bathrooms and kitchens, etc. Mould, fungi and other microorganisms can be found in water filtration systems, extractor fans, drains, towels, rugs and soft furnishings, tile grout, spaces / voids around baths, showers and sinks, before being transferred to other locations. Mould / fungi also produce mycotoxins in the form of gases, which can be silently poisoning household occupants - inhibiting energy metabolism and neurotransmitter homeostasis.
Nasopharyngeal inflammation and even intracranial pressure can sometimes be a "helpful" clue to investigate if there is a potential mould issue.
Carpets, window frames, walls, skirting boards, ceilings, books and bookcases, etc should also be inspected and maintained appropriately. Commercial air quality testing and mould remediation services are also available.
If not completely bed-bound and where the room doesn't have plants and/or pets (which can be excluded from the room for an hour), a relatively cheap ozone generator can be used to disinfect entire rooms, very effectively. [NB. This will cause a number of materials to off-gas aldehydes and other volatile organic compounds (VOCs). [YOU WILL NEED TO VENTILATE THE ROOM FOR A REASONABLE PERIOD OF TIME, AFTER SANITISING WITH OZONE.]
Sunlight is also helpful in inhibiting certain microorganisms.
Overall, it is essential to maintain good hygiene practices – regularly disinfecting surfaces and fabrics, to prevent ongoing reinfection and unnecessary delays in progress.
We also share our microbiomes with close contacts. This happens in both directions, which can create interesting challenges and yet another reinfection cycle, in some cases. A host with a competent microbiome and immune system should be resilient against new challenges, helping to prevent this.
Where possible, getting outside of the home environment regularly can boost microbiome diversity and improve the efficiency of microbiome remodelling, as can interaction with pets who spend time outdoors. There are many anecdotes of short-term remission events occurring, simply by taking a holiday away from home. Unfortunately, these normally revert within 1-2 months of returning to the original environment, or eg. staying in the same hotel room for more than 1-2 months.
Anyone who has experience with ME/CFS-like conditions is deeply familiar with the daily challenge and risks associated with "crashing”, technically called Post Exertional Malaise (PEM).
In contemporary guidelines for diagnosing ME/CFS, PEM is now the key symptom enabling diagnosis, which - in the absence of much discussion about biomarkers, supports or interventions - can give us the mistaken assumption that it is a somewhat designed-in feature with inalterable risks (despite our experience of it being dynamic, changing every day).
PEM typically results in fatigue / malaise, flu-like symptoms and quite frequently - tinnitus, joint laxity and/or pain.
Severe patients often recall how a particular incident of PEM decreased their baseline, or persisted for days / weeks / months. The very real trauma associated with this loss of baseline can additionally contribute to sympathetic overdrive and liver glycogen depletion, perpetuating a loop / trap of these symptoms, without "trauma" having been the origin.
A more complete hypothesis surrounding the mechanisms involved in PEM is important and described in the upcoming paper. However the work-in-progress diagrams are available on the Disease Model page (see figure 9, figure 12, figure 18 and "2.2.6 Cortisol, limbic system, glycogen and IFN-γ" for key influences affecting glycogen homeostasis and mineral status.)
Some highlights from this work describe oxidative stress and (liver) glycogen depletion as the two major variables driving PEM.
Zinc is a cofactor for over 300 enzymes, including those responsible for
metabolising lactate and detoxifying aldehydes (including from
pathogens). Zinc is certainly not the only mineral deficiency involved, but plays a central role in a major self-perpetuating loop that leads to these crashes. "Lactic" acidaemia, which lowers arterial and venous pH, weakens the binding of zinc to albumin, thereby causing the kidneys to accelerate the excretion of zinc and electrolytes in urine. The same acidaemia that causes zinc loss also forces the kidneys to dump phosphate, magnesium, calcium, sodium, and potassium. Because these are required for normal mitochondrial metabolism, glycolysis and coenzyme synthesis, their depletion directly undermines energy production, causes the lactate threshold to lower and the energy crisis to deepen with each episode of acidaemia.
Separately, another branch of this cascade which elevates specific cytokines, further elevates hepcidin, inhibiting Divalent Metal Transporter 1 and Ferroportin - functionally blocking absorption and distribution of at least 11 metals throughout the body.
For example, a deficiency in manganese can significantly impacts hepatic gluconeogenesis (the creation of new glucose) at pyruvate carboxylase, which is a critical factor in preventing the "crash" associated with PEM, as well as post-prandial brain-fog, fatigue.
Similarly, low iron, selenium, iodine and/or calcium availability can affect thyroid hormone synthesis, creating an almost-identical outcome for this part of the metabolism.
Oxidative stress created during exertion, in part caused by insufficient enzymatic metabolism of reactive oxygen species by metal-dependent enzymes like CuZnSOD, MnSOD, glutathione peroxidase + glutathione reductase, catalase consumes excessive Vitamin C and BH4, further disrupting energy pathways and neurotransmitter balance.
Therefore, to prevent PEM, one must not only "pace" mitochondrial metabolism, to appropriate levels of eg. (immune) activity, but also correct resource insufficiencies affecting your biochemistry - maintain levels of glycogen, electrolytes, minerals, and active forms of B vitamins simultaneously. The threshold before encountering PEM is progressively increased / reversed by supplying precision support to these underlying mechanisms. In many cases, this must be achieved by non-oral routes, as the inflammatory cascade blocks normal dietary uptake.
Pacing as only part of the road to recovery
When patients are not informed of these dynamic processes affecting PEM, "pacing" becomes reduced to a management or behaviour strategy, self-management becomes burdonsome, and can be psychologised by care teams, if residually impacted by the logic of Graded Exercise Therapy (GET). However, the second risk in managing PEM, once staging targeted nutritional interventions towards slow repair, is the risk of muscle activity staying below baseline. This needs to be carefully explained because it is not advocating a return to the GET approach (which was based on a false theory of muscle conditioning/deconditioning, whilst ignoring the specific role of pathogens, deficiencies and neuro-immune function affecting capacity otherwise).
The key difference in the disease modelling and protocol here is the recognition of the role of muscle activity in directly promoting the activity of Interferon-gamma (IFN-γ), which the model identifies as a primary tool used by the innate immune system against microbial challenges. Physical activity, along with heat and sex hormones, helps shift the immune system toward this IFN-γ response, which is necessary for tissue adaptations and long-term resilience. Interferon-gamma (IFN-γ) drives the TCA cycle flux, which generates the NADH required to replenish the mitochondrial NADPH pool. This surplus of NADPH acts as a critical reductive currency that powers enzymes like NADPH oxidase (NOX) and nitric oxide synthase (NOS) to produce the reactive oxygen species (ROS) necessary to oxidise and kill pathogens hidden in biofilms.
Furthermore, muscle contractions are the primary driver of lymphatic circulation, ensuring the effective excretion of metabolic waste, and returning extracellular fluids to the bloodstream to prevent blockages that lead to localised hypoxia and lactic acidemia. (This is why manual lymphatic work is even more important when physical exertion is restricted or limited, and on non-exercise days).
While physical exertion promotes essential processes like hormone synthesis and methylation, it must be carefully balanced through "pacing" to avoid over-exertion that triggers periods of lactic acidemia, crippling the enzymes needed for detoxification and energy production.
Consequently, an optimal recovery strategy involves understanding biomarkers, and testing the appropriate upper threshold for activity each day to maintain immune resilience, while ensuring the recovery window remains short and does not provoke an extended period of anaerobic metabolism.
Acidaemia: a key influence in disease progression
Pacing is intended to limit a biochemical loop in which exertion-driven lactic acidaemia and microbiome-derived acetaldehyde combine to accelerate renal and sweat zinc, phosphate, calcium, magnesium, sodium, potassium and other mineral losses and, in turn, deepen the very metabolic defects that provoke symptom flare-ups.
In unstressed adults the kidney excretes roughly 0.02–0.97 mg zinc per 24 h, a volume-dependent trickle that represents a minor fraction of total turnover. A sweat concentration of about 0.5 mg L⁻¹ means two litres of perspiration add ≈1 mg to that baseline. Neither figure on its own threatens balance, but both are highly sensitive to pH and albumin status.
Low arterial or venous pH weakens the high-affinity zinc site on albumin; the drop in binding increases the freely filterable fraction and raises renal clearance in proportion to the acidaemia. In diabetic ketoacidosis (our best human analogue for fermentation-related lactic acidaemia) 24-h urinary zinc typically doubles to about 1 mg and can reach 2–3 mg when urine flow exceeds 3L. Rat studies in ammonium-chloride acidosis show a similar two-fold rise, confirming that pH itself, and not only glycosuria, drives the leak. When mitochondrial impairments push the exercise lactate below pH 7.30, the same renal multiplier is expected in ME/CFS.
Acetaldehyde supplies a second driver. Aldehydes oxidise cysteine thiolates in metallothionein, liberating bound Zn²⁺ and creating a transient cytosolic zinc wave; the displaced ions must then be buffered in plasma, mainly by albumin and, ultimately, by renal clearance.
As gut ethanol is oxidised to acetaldehyde before significant systemic absorption, EtG and other sobriety markers are often negative, yet aldehyde exposure and zinc displacement are continuous. However, Mosaic DX's Toxdetect panel contains 2-Hydroxyethyl Mercapturic Acid (HEMA), which is able to capture acetaldehyde burden.
1. Low pH and acetaldehyde lower albumin affinity, increasing the freely filterable fraction of divalent cations.
2. Acidification and osmotic load inhibit ZIP/ZnT, TRPM6/7 and other re-uptake transporters.
3. Bone buffering dissolves hydroxy-apatite, providing Ca²⁺, Mg²⁺, Zn²⁺ and phosphate that are cleared in the same urine.
4. The loss of Zn further affects lactate dehydrogenase, aldehyde dehydrogenase, prolyl hydroxylase, superoxide dismutase and carbonic anhydrase, worsening aldehyde and lactate accumulation, oxidative stress and buffering capacity, so excretion of every mineral above is amplified again.
Zinc loss is a significant problem. More than 300 enzymes use zinc as a structural or catalytic co-factor, including carbonic anhydrase, aldehyde dehydrogenase, prolyl hydroxylase, Cu/Zn-superoxide dismutase, alkaline phosphatase, RNA and DNA polymerases and multiple DNA repair endonucleases. Figure 7 on the Disease Model page highlights some of the key enzymes relative to the cascade. Falling zinc therefore slows aldehyde dehydrogenase, prolongs aldehyde residence (Vitamin B6, Vitamin A, neurotransmitter metabolites, histamine, etc), weakens carbonic-anhydrase-mediated bicarbonate buffering and blunts superoxide dismutase activity, tightening oxidative and acid-base stress.
The result is a feed-forward loop - lower zinc reduces lactate handling and aldehyde detoxification, pH and acetaldehyde both rise, albumin binding falls further and renal clearance accelerates again.
For pacing the practical target is to keep lactate levels appropriate, venous pH ≥7.30 and sweat volumes modest. Short activity bursts with generous rest, cool environments, avoidance of febrile triggers and rapid rehydration all reduce the renal multiplier and the sweat term.
Elemental zinc intake should routinely exceed 30 mg per day and be coupled with copper and mineral testing to avoid secondary deficiency. Spot or 24h urine zinc above ~1 mg, rising 24h urine lactate or a downward trend in serum albumin signal that either exertion must be cut or supplementation increased.
Out of range lactic acid, oxalic acid and phosphoric acid markers in the OAT are useful indicators for mitochondrial dysfunction and lactic acidaemia.
Phosphorus and sulfur markers on Oligoscan are useful LAGGING indicators for this cascade, also. Where low, and where dietary sufficiency / supplementation is being correctly managed, this can indicate excess exertion, relative to metabolic capacity / lactate threshold. Hypoxia, septicaemia and blood-flow issues should be further explored and excluded.
LDH isoenzymes can be very useful, however also confounded by the zinc and NAD+ status.
Wearable lactate meters will be available in coming months / years.
Left unchecked, daily combined losses in this phenotype reach 2–4 mg, three to six times the obligatory renal flux and is sufficient to disable key zinc enzymes within weeks, creating a spiral progression of metabolic impairments.
NADPH: a reductive "currency", powered by TCA cycle flux
One of the primary tools the innate immune system can use against microbial challenges is creating reactive oxygen species (ROS) to oxidise these pathogens. IFN-γ partially inhibits Complex I, which means that NADH generated by the TCA cycle can be diverted towards elevating NADPH, also powering NADPH oxidase (NOX) and nitric oxide synthase (NOS), which then (like xanthine oxidase, which uses NAD+ instead) create reactive oxygen species to oxidise pathogens, potentially damaging your cells in the process.
Excess NADPH / low NADP with elevated NADH / low NAD+ can be observed / inferred by elevated cholesterols, impaired glucose metabolism, elevated cortisol / inverted diurnal release profile, low aldosterone, low testosterone (often with elevated DHT), low BH4, impaired methylation and various other compensations.
NADPH is a critical cofactor in human metabolism, serving as the primary reductant for antioxidant systems, anabolic pathways, and xenobiotic clearance. While cytosolic sources like glucose-6-phosphate dehydrogenase (G6PD) are well known, a large portion of NADPH - especially during periods of stress or high energy demand - is maintained by the mitochondria, specifically through the enzyme NAD(P) transhydrogenase (NADPT).
NADPT is embedded in the inner mitochondrial membrane and uses the proton gradient to transfer reducing power from NADH to NADP⁺, producing NADPH:
NADH + NADP⁺ + H⁺ → NAD⁺ + NADPH
This links mitochondrial NADH levels - which rise with increased TCA cycle activity - to the regeneration of mitochondrial NADPH.
During exertion/exercise, immune activation, or inflammatory adaptation, metabolic flux through the TCA cycle increases, producing more NADH. As long as the mitochondrial membrane potential (Δψm) remains intact, this NADH surplus feeds directly into NADPT, increasing mitochondrial NADPH availability. The result is enhanced capacity for antioxidant defence (via glutathione and thioredoxin systems), and support for NADPH-dependent biosynthesis, including steroid hormones, proline, and coenzyme Q.
Interestingly, partial inhibition of Complex I, whether through physiological stressors like interferon-gamma (IFN-γ) - used by the body both in immune defence and as a signalling molecule during muscle adaptation - or low-grade mitochondrial oxidative stress, can shift the system into a transiently favourable state. In this “grey zone”, NADH accumulates upstream of Complex I, fuelling NADPT activity more aggressively. As long as the respiratory chain isn’t fully impaired and Δψm is preserved, this can elevate the mitochondrial NADPH pool, supporting redox balance and tissue resilience. This may partly explain the hormetic benefits of controlled stress exposures such as fasting, exercise, or polyphenol intake.
However, this compensatory state is fragile. If Complex I is significantly inhibited - by toxins, sustained inflammation, infection, or mitochondrial dysfunction - the proton gradient begins to collapse. NADPT can no longer function effectively, and NADPH regeneration fails despite high NADH availability. The result is impaired antioxidant defence, loss of redox control, and metabolic vulnerability.
This interplay - between NADH accumulation, proton gradient integrity, and NADPH generation - reveals how mitochondrial function dynamically regulates the redox economy of the cell, determining whether the system bends toward adaptation or collapse.
NADPH functions as a central reducing currency in human metabolism, and the enzymes that consume it fall broadly into two major functional clusters: biosynthesis and innate immune response / detoxification.
On the biosynthetic side, NADPH is used to support a wide range of anabolic processes. Within the mitochondria, endoplasmic reticulum, and peroxisomes, NADPH is required for building complex molecules including cholesterol, steroid hormones, and ubiquinone (CoQ10). It also plays key roles in amino acid interconversion pathways (e.g. proline, ornithine) for collagen synthesis, for methylation and in maintaining cofactor pools such as tetrahydrobiopterin (BH₄) and tetrahydrofolate (THF). Many of these reactions involve reductive steps that cannot proceed without a steady supply of NADPH, especially in pathways with high flux during cell growth, repair, or hormone synthesis.
By contrast, the cytosolic and membrane-associated NADPH-consuming enzymes are primarily involved in defensive or detoxification roles. These include enzymes like NADPH oxidases (NOX), inducible nitric oxide synthase (iNOS/NOS2), and cytochrome P450 reductase (POR), which feed reducing power into systems that produce reactive oxygen and nitrogen species. These reactive molecules play essential roles in microbial killing, xenobiotic metabolism, and immune signalling. In parallel, NADPH also fuels antioxidant and damage-mitigation systems, including the glutathione reductase and thioredoxin reductase pathways, as well as aldo-keto and carbonyl reductases that detoxify lipid peroxidation products and reactive carbonyl species.
Together, these two clusters reflect the role of exertion / TCA cycle flux → NADPH in human physiology - enabling synthesis and repair on one hand, and powering immune defence and redox control on the other. The balance between these uses is tightly regulated, and disruptions-such as oxidative stress, chronic inflammation, or metabolic imbalance-can deplete NADPH reserves, impacting both clusters simultaneously.
For optimal immune response and hormones, “pacing” should always be attempted - testing the appropriate upper threshold for activity, each day, unless that threshold has been exceeded already. Over sufficient time, inactivity leads to immune insufficiency, which is wholly undesirable, as the immune response is pivotal for maintaining resilience against pathogens.
The combination of supplements here should help improve the exertion threshold and buffer against “crashing”. However, you may have already noticed that fungal “die-off” symptoms share some common features with PEM and crashing, as does any immune activity.
(Acetaldehyde ->) histamine is another significant influence, as exertion uses histamine signalling to control glycogen homeostasis in the muscles and liver. This will add some challenges for identifying your upper limits for exertion / glycogen synthesis rate.
(Methylation | glycine recycling ->) (glutathione peroxidase +) glutathione reductase activity provides the cytosolic NADPH redox partnership to G6PD and 6PDG activity in the Pentose Phosphate Pathway. When impaired, this can be a cause of dysregulation for PRPP + R1P synthesis, required for uridine triphosphate -> glycogen synthesis, inosine synthesis and NAD+ synthesis pathways. Certain heavy metals can dramatically impair selenium binding with glutathione peroxidase and its activity while others can impair glutathione reductase activity. In this way, impaired methylation, low glycine or heavy metal toxicity can impair glycogen synthesis rates and cause a lowered PEM threshold.
(You can find more on this in 2.2.6 Cortisol, limbic system, glycogen and IFN-γ.)
Note the upper limit for exertion will be artificially reduced when IFN-γ is elevated and Complex I is inhibited, during any intense immune response. Increasing temperature elevates IFN-γ levels potentially ten-fold. Spirulina, schisandra and curcumin modify this pathway, favourably, by inhibiting NOX.
Proceed carefully. This approach requires edging the upper threshold of your daily baseline with a certain amount of patience and courage, assuming that precision nutritional supports and biomarker literacy make a very real difference to risks of PEM, and that results will come in a non-linear fashion.
Increased baseline can noticeably diminish intracellular pathogen reserves (producing many other benefits to cognitive function etc). As long as your recovery window is short and you're not experiencing extended periods of lactic acid metabolism (see: Figure 12), your exertion falls into the "safe and appropriate" zone and is beneficial towards recovery. If phosphorus (+ sulphur) stalls / gets lower on oligoscans, or oxalate markers increase on OATs, you may need to better support the mitochondrial function, investigate glucose / hypoxia / oxidative stress issues, and/or pace your exertion more.
Thoracic Outlet Syndrome (TOS)
The lower traps and rhomboids are essential muscles responsible for scapular control and stability. Weakness in these muscles can lead to poor scapular control, which can result in chronically pronated shoulders and TOS.
Pronated shoulders occur when the shoulder blades “wing” and rotate forward, leading to a hunched posture. This can occur when the lower traps and rhomboids are weak and unable to maintain proper scapular alignment and is common in people with hypermobile Ehlers Danlos Syndrome (hEDS) metabolism. hEDS metabolism is described in the disease model as a "normal feature"
whenever innate immune response pathways are activated and/or specific
mineral deficiencies are present. The resulting forward shoulder position can cause tension and compression in the neck and shoulder region, leading to TOS.
TOS is a condition where the nerves, lymphatic thoracic duct and blood vessels that pass through the thoracic outlet become compressed, leading to pain, numbness, and weakness in the arm and hand. This can be bilateral or unilateral. Forward head position will further contribute to the progression of this syndrome. This can cause impaired immune response and water retention / lymphoedema.
To prevent TOS and other related conditions, it is essential to maintain proper scapular control and stability. This can be achieved through exercises that strengthen the lower traps and rhomboids, such as scapular retraction and shoulder blade squeezes. Additionally, maintaining good posture and avoiding activities that require prolonged shoulder and arm elevation can help prevent TOS, however when this position occurs during sleep, it can be hard to avoid.
Slipped Rib Syndrome, costochondritis and chest pain
Slipped rib syndrome, costochondritis, and worrying chest pain can all be downstream effects of a poorly seated rib – usually between T6–T8. When a rib is not properly aligned, it can cause thoracic instability, leading to overworked intercostal muscles and inflammation in the surrounding tissues. This is a common issue where hEDS metabolism is present.
Slipped rib syndrome occurs when a rib slips out of place and moves too easily, causing pain and discomfort. Costochondritis is inflammation of the cartilage that connects the ribs to the breastbone, which can also cause significant chest pain, which can mimic having a cardiac event.
When a rib is poorly seated, it can create an unstable environment for the intercostal muscles that are responsible for breathing. With mitochondrial dysfunction, these overworked muscles can become fatigued and inflamed, leading to scary chest pain and difficulty breathing.
It is wise to seek medical attention if you experience chest pain, as it can be a symptom of more severe conditions such as a heart attack or pulmonary embolism. However, if you have chronic chest pain that is related to slipped rib syndrome or costochondritis, treatment may include correcting the alignment of the rib and regular physical therapy, once any hEDS metabolism is corrected. Like any other resistance training, this tissue rehabilitation process will normally take weeks or months to complete.
A (free for the Born Free community) online posture rehabilitation course can be found here, using code: Free4Me - please carefully observe the modification to the advanced stretching technique for working around hEDS metabolism.
Atlas and / or upper cervical misalignment
Another potential structural issue can come from neck alignment
issues, relating to trauma and / or chronic cranial instability.
This
can severely affect blood-flow to and from parts of the brain via impingement of eg.
vena and arteria vertebralis, leading to neural hypoxia and a range of other symptoms. This is more likely to occur with someone
who has hEDS metabolism / collagen synthesis issues - which is described
as a feature in this disease model.
Various tests and interventions are available, with different
levels of risk / return. One particularly interesting approach is Atlas
Orthogonal (AO). Unlike the "high risk" neck manipulation techniques
used by everyday chiropractors, the AO method is gentle and uses a
special machine to perform the atlas adjustment.
https://youtu.be/O-cjIq7s6mM
As a precursor or replacement for AO, there are also some specialised stretches you can perform at home for free. These are included as part of the posture rehabilitation course above, however there are also some standalone videos on upper cervical stretching by various specialists.
https://youtu.be/NATds3r1zxw
If
you've had a previous history of neck trauma from vehicle accidents,
sports, chiropractic or other interventions, etc., visiting an AO
practitioner could be a worthwhile investment.
Practitioners can be found in many parts of the US, Australia and only sparsely in EU, by eg. searching Google for "atlas orthogonal near me"
Cortisol is the “master” negative regulator for IFN-γ related immune activity and promotes catabolic energy availability via epinephrine (adrenaline).
Elevated cortisol doesn't just suppress immune function; it also alters neurotransmitter balance, which can influence mood, cognition, and energy levels.
What this means is that any/all influences which promote cortisol also decrease IFN-γ activity and provide some “relief” for many of the symptoms observed in ME/CFS.. while potentially creating others. This allows periods of increased functionality, while simultaneously inhibiting the necessary suppression of the pathogens that are triggering the innate immune response pathways.
In the disease model, we have described how cortisol acts as a “sensor” and signalling relay for insufficiencies of NAD+, P5P and glucose / glycogen, via phosphatidylserine and HSD11β1/2 flux (see figure 4). The metabolism for NAD+ and P5P is altered by IFN-γ and they act as upstream sensors for specific IFN-γ activities which can upset the metabolism or cause excessive tissue damage via oxidative stress. An inverted diurnal cortisol release pattern is expected.
When any of the sensed metabolites are insufficient, cortisol increases, signalling for an increase of epinephrine. This promotes energy "scavenging" or "catabolism", while inhibiting IFN-γ immune activity. This allows some of the cofactors and metabolites to replenish and by doing so, it helps restore normal metabolism.
However, the same epinephrine -> cAMP-PKA elevation from any trigger also signals for your cells to stop storing glycogen and instead use the existing glycogen pools for energy (see figure 1, upper right). Epinephrine activates hepatic glycogen phosphorylase and inhibits glycogen synthase within minutes; glucagon cooperates during fasting. Cortisol modulates these systems on a slower timescale. Glycogen storage can therefore become problematic when epinephrine and/or cAMP-PKA is dysregulated and chronically elevated.
As the metabolites reach sufficiency, cortisol levels normalise. If any triggers for IFN-γ are still present, then IFN-γ activity will resume and the cycle will repeat, as necessary.
Exercise, sex hormones and heat can increase IFN-γ. Dietary supplements can support IFN-γ activity. Cortisone medications are potent immunosuppressants and will inhibit IFN-γ.
Appropriate carbohydrate and protein intake (with uninhibited metabolism) supports optimal glycogen homeostasis. Sublingual NAD+ or NADH can efficiently support the total NAD+:NADH pool status, methylene blue can support the NAD+:NADH redox and apigenin can reduce the pool degradation. Creatine can reduce the methylation “costs” associated with use of this pathway and also increase glucose transport. Magnesium and zinc can support B6 -> P5P metabolism. Manganese, biotin and B12 sufficiency is required for conversion of other substrates (protein -> amino acids, odd-chain fatty acids) into glycogen, usually via the TCA cycle to the glycolysis pathway, however flowing in reverse.
Hypothyroidism affects both glucose metabolism and “B6 toxicity” / P5P insufficiency. The thyroid hormone, T3 (tyrosine, heme iron, iodide, selenium, calcium) is required to maintain FMN levels, needed for P5P recycling and to induce pyruvate flux into the TCA cycle.
Chronic hypoxia can be a significant contributor to this cascade.
The primary sex hormones (testosterone / DHT in males, estradiol in females) sense the elevation of NADPH (created during physical / metabolic activity), with sufficiency of NAD+, magnesium, boron and zinc. These primary sex hormones then promote creatine synthesis and glucose uptake. They inhibit cortisol levels, promote nitrogen metabolite recycling and glycogen synthesis. This also allows IFN-γ activity to increase, which is also needed for tissue adaptations to exercise. Non-optimal sex hormones can cause chronic cortisol increase.
Overnight, hepatic glucose output draws on glycogen then shifts toward gluconeogenesis; the pre-awakening rise in cortisol supports glucose production, whereas glycogen replenishment resumes mainly with daytime, insulinised feeding.
In severe ME/CFS this diurnal rhythm is
delayed, blunted at night and erratic by day. With hepatic glycogen
never fully restored, even small physical or emotional stresses deplete
the reserve. The body responds with abrupt pulses of cortisol and
epinephrine to keep blood glucose within safe limits, but these surges
have costs and the repetitive signalling can contribute to nervous
system adaptations / programming towards hyper-arousal and sympathetic
overdrive.
Histamine triggers glycogen redistribution
When intestinal dysbiosis shifts towards ethanol‑producing organisms, portal blood delivers a steady acetaldehyde load to the liver. Hepatic aldehyde dehydrogenase (ALDH) is the main clearance route, yet acetaldehyde itself oxidises the enzyme’s catalytic cysteines and slows its own detoxification. The diamine oxidase (DAO) -> ALDH pathway, responsible for extracellular histamine degradation in the gut wall and liver sinusoids, is inactivated by the same aldehyde, as is the monoamine oxidase MAO) -> ALDH pathway, in the brain. Consequently, acetaldehyde and histamine accumulate in parallel. Extracellular ATP signalling can also degranulate mast cells and release histamine, which can be triggered by a number of sources, including autonomic dysfunction.
Microbiome dysbiosis allows basal histamine levels to become elevated and creates further sensitivity to small histamine release triggers.
Histamine released from resident mast cells activates two hepatic pathways. H1 receptors raise intracellular Ca²⁺ and switch phosphorylase kinase, accelerating glycogenolysis. H2 receptors follow the classical Gs → cAMP → PKA → CREB/CRTC2 route, up‑regulating the G6pc gene and sustaining gluconeogenesis. Plasma glucose rises briefly, then falls once hepatic glycogen stores are exhausted, prompting compensatory sympathetic activation. In susceptible individuals this often presents as episodic tachycardia, light-headedness and adrenergic symptoms 45–90 minutes post-meal.
However, histamine also binds H1 receptors on perivascular macrophages in skeletal muscle. The resulting IL‑6 pulse engages STAT3 in adjacent fibres, increasing GLUT4 expression and glycogen‑synthase activity.
Logically, under normal circumstances this histamine signalling cascade would support post‑exercise muscle glycogen recovery, by converting liver glycogen into circulating glucose, whilst promoting muscle glycogen storage.
However, when hepatic glycogen is already depleted, the extra glucose uptake is limited, leaving IL‑6 signalling elevated and favouring low‑grade inflammation. This also creates and/or exacerbates symptoms of liver glycogen depletion.
Acetaldehyde compromises tight‑junction proteins - particularly claudin‑1, occludin and ZO‑1, through oxidation of cellular glutathione and direct adduct formation with junctional proteins. Transepithelial electrical resistance falls, allowing luminal antigens (dietary proteins, lipopolysaccharide, fungal mannans) to enter the portal and systemic circulation. These antigens engage hepatic Kupffer cells and circulating innate‑immune receptors, amplifying IL‑6, TNF‑α and further mast‑cell priming. The additional antigen load therefore strengthens the histamine–acetaldehyde feedback and broadens symptom variability to include post‑prandial urticaria, arthralgia and fluctuating cognitive function.
Mitochondrial ROS generated during acetaldehyde metabolism oxidise tetrahydrobiopterin (BH4) to BH2, uncoupling endothelial nitric‑oxide synthase. Uncoupled eNOS diverts electrons to superoxide formation; superoxide combines with residual nitric oxide to form peroxynitrite, which nitrates and further impairs both ALDH and DAO. The resulting endothelial dysfunction limits capillary dilation, reduces oxygen delivery to muscle and contributes to orthostatic intolerance.
Mast‑cell activity is sensitive to the prevailing sex‑steroid environment. Physiological oestradiol concentrations enhance Ca²⁺ influx through membrane‑bound ER‑α, lowering the threshold for degranulation. Androgens act more slowly via nuclear AR to repress cytokine transcription and reduce mediator content. The net effect is hormone‑dependent rather than genetically sex‑specific: high oestrogen states (peri‑ovulation, pregnancy, oestrogen therapy) generally increase histamine release, whereas adequate testosterone or progesterone temper it.
Understanding this cascade clarifies why seemingly minor dietary choices, hormonal fluctuations or exercise sessions can provoke disproportionate symptoms. Interventions need to address microbial-sourced acetaldehyde, barrier integrity, and enzymatic detoxification simultaneously to break the self‑reinforcing loop.
Figure 9 shows this in a more concise way.
Histamine is also known as the stomach’s on-demand acid tap. Enterochromaffin-like (ECL) cells in the gastric corpus suffuse their neighbourhood with histamine whenever gastrin or vagal acetylcholine says it is time to digest. The molecule travels perhaps a millimetre, binds H2 receptors on neighbouring parietal cells and ignites the Gs → cAMP → PKA cascade that lifts proton pumps to the apical membrane. Within minutes, the luminal pH trends towards highly acidic, pepsinogen flips to pepsin and dietary proteins begin to unravel. Antagonising H2 receptors, as many dyspepsia patients discover, cuts this acid tide by roughly two-thirds, while potentially disturbing protection against oral pathogens entering the small intestine.
Further down the GI tract, histamine’s role becomes subtler. In the muscularis it tweaks peristaltic tone: H1 receptors on circular muscle promote contraction, whereas H2 receptors on longitudinal muscle ease it, ensuring chyme does not idle too long yet still pauses where absorption is richest. In the ileum histamine encourages chloride and water secretion through enteric neural reflexes, a housekeeping flush that keeps the mucosa clear of excessive bacterial growth.
Histamine also acts as a sentinel mediator. Intestinal mast cells sample antigenic fragments leaking through the epithelium; when they degranulate, the released histamine increases local blood flow and vascular permeability, banking extra immune cells against potential breach. At modest concentrations this response is quietly protective, tightening junctions through H4-receptor signalling on epithelial cells and stimulating mucus production that traps pathogens.
At higher levels, eg. created by chronic acetaldehyde, the same mechanisms become counter-productive: permeability rises too far, afferent nerves fire, and the familiar triad of bloating, cramps and watery stool appears. Acid may swing low, motility becomes erratic, antigen load climbs and patients experience the fluctuating constellation of symptoms often labelled “histamine intolerance” or Mast Cell Activation Syndrome (MCAS).
Overall, some of these challenges can influence further self-sustaining cycles, eg.
Increased protein catabolism - cortisol mobilises amino-acids for gluconeogenesis, gradually lowering the circulating pools of (often already problematic, due to low Queuine) tyrosine, histidine, asparagine and aspartate, which are needed for neurotransmitter and enzyme synthesis, affecting energy metabolism, causing additional epinephrine spikes / sympathetic bias.
Dysregulated metabolic feedback - frequent intermittent epinephrine bursts further inhibit glycogen synthase, perpetuating the under-filled liver glycogen tank, causing additional epinephrine spikes / sympathetic bias.
Sympathetic overdrive
There are also many influences observed in ME/CFS which can contribute to sympathetic overdrive and chronic flight/flight. Overall, the balance is normally biased heavily against being able to maintain parasympathetic sufficiency and (liver) glycogen stores.
This bias NEEDS to be shifted towards a neutral balance to restore normal energy metabolism and help remove glycogen deficiency as an influence in debilitating symptoms like POTS, PEM, cognitive, mood and sleep disorders. This means adding / increasing parasympathetic tone promoting influences into your routine and removing as many unnecessary sympathetic tone promoting influences, often sources / triggers of epinephrine spikes.
Some of these influences can induce long-term shifts, some are acute effects.

Separately, the catecholamine degradation pathways needs to be restored and adrenergic receptor expression / sensitivity restored, to remove unhelpful "hair-trigger" response to stimuli.
A simple test for sympathetic overdrive is trying to swallow, three times, quickly. In severe ME/CFS, loss of ability to swallow often coincides with loss of parasympathetic / vagal tone.
https://www.instagram.com/reel/DHtW0iHsbOE/
[A helpful Instagram video by Taylor and Alisha Kruse - they have a lot of relevant neuro content.]
What the parasympathetic system actually does
The parasympathetic nervous system sets the body’s “rest-and-digest” baseline. It is not an on/off switch. Brainstem nuclei send fibres through the vagus to the chest and abdomen, and sacral outflow serves the pelvis. When sympathetic drive runs high for long periods, parasympathetic signalling is blunted or becomes erratic. The result is predictable changes in gut propulsion and secretion, glandular output, pupil behaviour, heart rhythm, bladder emptying, and sexual function.
Gastrointestinal
Swallowing - starting a swallow is a voluntary, somatic motor act coordinated in the brainstem using cranial nerves V, VII, IX, X and XII. Parasympathetic vagal output is not required to initiate it. Once the bolus enters the oesophagus, parasympathetic pathways organise primary peristalsis and relax the lower oesophageal sphincter. The enteric nervous system can still generate secondary peristalsis locally, but global coordination drops when vagal tone is low.
Stomach - vagal input enables receptive relaxation of the fundus, coordinates antral grinding, and gates pyloric opening.
Pancreas and bile - vagal drive stimulates pancreatic enzyme and bicarbonate secretion, and assists gallbladder contraction alongside CCK.
Intestine and colon - parasympathetic-enteric crosstalk supports peristalsis and fluid secretion. Sacral outflow drives the defecation reflex by contracting rectum and relaxing the internal anal sphincter.
Sympathetic overdrive pattern: dry mouth, weak or discoordinated peristalsis, early satiety, reflux from poor LES control, slow gastric emptying, flat or greasy stools from low enzyme/bile delivery, bloating, constipation or paradoxical alternating bowel habit.
Cardiovascular
Vagal tone sets the resting heart rate below the pacemaker’s intrinsic speed and stabilises AV nodal conduction. With persistent sympathetic bias you see a higher resting rate and reduced beat-to-beat variability.
Sympathetic overdrive pattern: resting tachycardia, low HRV, exaggerated heart-rate responses to minor stressors.
Respiratory
Vagal efferents tighten airway smooth muscle and promote mucus secretion, which is part of normal airway defence. Sympathetic signalling tends to dilate the bronchi and dry the mucosa. In real life both systems interleave.
Sympathetic overdrive pattern: dry airways, throat irritation and cough with little mucus. In some phenotypes, unstable vagal reflexes coexist with overdrive and produce intermittent bronchospasm.
Ocular
Parasympathetic fibres constrict the pupil to light and enable near-focus by contracting the ciliary muscle. They also drive tear secretion.
Sympathetic overdrive pattern: larger pupils in room light, difficulty with near vision, dry or gritty eyes.
Salivary and nasal glands
Parasympathetic secretomotor drive sustains watery saliva and nasal mucus that humidifies inspired air.
Sympathetic overdrive pattern: dry mouth, altered taste, tooth and gum vulnerability, nasal dryness or crusting.
Urinary
Sacral parasympathetic outflow contracts the detrusor and relaxes the internal sphincter during voiding. Somatic pudendal control handles the external sphincter.
Sympathetic overdrive pattern: hesitancy, weak stream, incomplete emptying, or conversely urgency from reflex instability.
Reproductive
Sacral parasympathetic activity initiates erectile tissue engorgement via endothelial nitric oxide. Emission and ejaculation are mainly sympathetic and somatic.
Sympathetic overdrive pattern: reduced arousal and erection quality (penile and clitoral), difficulty sustaining engorgement.
Here is a table of influences that promote acute and/or chronic *parasympathetic* tone:
Here is a table of influences that promote acute and/or chronic *sympathetic* tone:
One of the many takeaways from the parasympathetic vs sympathetic influence tables above is that any kind of breathing disorder, especially one that biases mouth breathing over nasal breathing can have a negative affect on achieving a balanced parasympathetic-to-sympathetic tone and will therefore be a high priority for targeted intervention.
https://pubmed.ncbi.nlm.nih.gov/37867476/
In that context, autonomic imbalance has also been reported in small studies for allergic rhinitis using HRV analysis.
https://pmc.ncbi.nlm.nih.gov/articles/PMC3582187/
Chronic sinonasal inflammation has also been studied in relation to autonomic markers (eg. HRV and pupillary light reflex metrics) in CRS cohorts. While this doesn’t prove nasal inflammation causes systemic dysautonomia, it supports the idea that sinonasal disease can couple to autonomic state, directly (sensory/autonomic reflexes) and indirectly (obstruction, sleep fragmentation, hyperventilation patterns).
https://www.nature.com/articles/s41598-021-01153-1
The clinical picture may include fasting intolerance, exaggerated post-exertional malaise, morning hypoglycaemia and wide swings in lactate that resemble certain glycogen-storage disorders, albeit driven by signalling rather than an inborn enzyme defect.
Therapeutic priorities are (i) frequent balanced meals that combine low-glycaemic carbohydrate with medium-chain triglycerides (or large doses of L-carnitine / acetyl L-carnitine used in the protocol), (ii) consider nocturnal adrenergic dampening (for example low-dose clonidine / ivabradine) to allow normal cortisol timing, and (iii) graded re-entrainment of sleep-wake cues so that the liver again “expects” to store glycogen after dusk.
Overall, multiple biochemical bottlenecks converge in ME/CFS to disturb catecholamine balance:
eg.
1. Queuine deficiency (secondary to microbiome dysbiosis) and tetrahydrobiopterin (BH₄) depletion slow translation and activity of tyrosine hydroxylase, the rate-limiting step in dopamine production, causing reduced dopamine synthesis.
2. Acetaldehyde directly inhibits aldehyde dehydrogenase (ALDH), depletes zinc and inhibits thiamine pyrophosphate (active Vitamin B1) synthesis. The zinc deficiency leads to further deficiencies of active B vitamins. Low FAD (active Vitamin B2) and zinc limit monoamine oxidase (MAO) and catechol-O-methyl-transferase (COMT) activity. Released dopamine, norepinephrine and epinephrine may therefore persist longer.
3. Acetaldehyde depleting zinc also affects P5P metabolism and dopamine synthesis by inhibiting aromatic L-amino decarboxylase (AADC) activity.
4. Acetaldehyde triggering mast cell activation and histamine release affects tyrosine hydroxylase activity.
5. Low iron and/or neural hypoxia, affecting phenylalanine and tyrosine hydroxylase.
6. P-cresol from dysbiosis, affecting dopamine beta hydroxylase.
7. Oxidative stress affecting phenylalanine, tyrosine and dopamine beta hydroxylase.
8. Electrolyte deficiencies affecting tyrosine hydroxylase, VMAT2, DAT and NET transporters.
9. cAMP-PKA dysregulation from chronic endogenous opioid synthesis pathway being activated by ALDH inhibition, if MAO is still functioning.
..This is not an exhaustive list.
Chronic sympathetic over-activity down-regulates vascular β₂- and presynaptic α₂-adrenoceptors. The system compensates with larger and less predictable bursts of catecholamines to achieve ordinary physiological tasks (for example standing or minimal exertion). This can also be exacerbated by (presumed regulatory, as a compensation) "autoimmune" antibodies for adrenergic receptors.
These receptor alterations also mean that any shift towards parasympathetic sufficiency can induce a level of temporary hypometabolism until the homeostasis resets, over a few weeks. The level of hypometabolism may also be enough to force a reflex into sympathetic spikes, exacerbating efforts towards normal homeostasis.
When catecholamine levels normalise, but receptors remain desensitised due to the previous sympathetic overdrive, chronic PTSD or stress, symptoms like fatigue, cognitive dullness, low BP, and orthostatic intolerance can appear. This results from a “relative catecholamine deficiency.” Even with normalised levels, desensitised receptors (like alpha2 and beta2) mean there's a decreased adrenergic tone and paradoxical crashes. Surges of epinephrine may occur after episodes of low energy, causing hypoglycemia-related adrenal bursts and crashes, leading to unexpected symptoms like anhedonia and fatigue.
Clinical tell-tales of an epinephrine surge while receptors are still half-asleep:
0–5 min - Sudden heart-in-throat palpitation, cold sweat, tremor, pilo-erection, brief spike in systolic BP. EPI acts on the fraction of β₁/β₂ receptors that are not desensitised; α₁ vasoconstriction is relatively spared.
5–30 min - Shaky hunger, light-headedness, hyper-alert or “wired” feeling. Hepatic glucose release overshoots; brain re-gains perfusion but over-reacts
30–120 min - Crash: profound fatigue, yawning, headache, sometimes nausea. As EPI is metabolised the receptor deficit is unmasked again; glycogen is partly spent, leaving a transient energy hole
Exercise intolerance and easy fatigability will occur. β₂-adrenergic drive to skeletal muscle and myocardium is blunted, so peak cardiac output and mitochondrial substrate flux lag behind demand. This mirrors the desensitisation seen in chronic muscle-pain cohorts.
Impaired β-oxidation impairs catabolic energy metabolism and means small drops in glucose activate hypothalamic “fuel alarm” pathways, causing adrenaline surges that can feel indistinguishable from panic. Sleep will temporarily become broken and difficult, relative to glycogen stores and norepinephrine "long" pulses.
The brain has a hard-wired crisis response for cellular energy deficit -
1. The ventromedial hypothalamus senses falling intracellular ATP or glucose.
2. It fires the sympatho-adrenal axis, causing the adrenal medulla to release epinephrine.
3. Epinephrine burns glycogen stores, elevates hormone‑sensitive lipase in adipose tissue, and raises cardiac output.
This
counter-regulation is best documented in insulin-induced hypoglycaemia:
even modest falls in plasma glucose produce a several-fold surge in epinephrine
that is not fully replaceable by glucagon alone.
These changes can reinforce an anxiety-phobia cycle. Each adrenergic spike produces tachycardia, dizziness and a sense of impending collapse; the cortex learns to associate ordinary movement with danger, encouraging further inactivity and social withdrawal. Poor sleep prevents overnight receptor resensitisation, and the cycle repeats. A large part of overcoming this vicious trap is awareness of the issue and then learning to consciously override the signals being fed to the nervous system while the transition is underway.
The receptors will wake up, however it's a slower journey:
β-receptor resensitisation needs days-to-weeks of lower catecholamine tone and adequate omega-3 intake (membrane fluidity matters).
The α₂ presynaptic brake tends to reset faster (days), which is why clonidine/guanfacine at night could smooth the ride during taper.
Adequate sleep and micronutrients (esp. Mg²⁺, Zn²⁺ and B-vitamins) can also hasten the up-regulation of G-protein coupling units.
Ketotifen can also be particularly helpful. Histamine released from mast cells can stimulate sympathetic outflow and locally augment norepinephrine release. Blocking H1 and stabilising mast cells removes that extra push on the accelerator. Long-term oral ketotifen has been shown to increase β2-adrenergic receptor density. Central H1 blockade and mild anticholinergic tone tilt the ANS parasympathetic, lowering baseline sympathetic tone and improving slow-wave sleep - both conditions that favour receptor resensitisation. Net effect: fewer histamine-triggered norepinephrine releases, shallower epinephrine spikes, and a slow rise in β-receptor responsiveness.
(Practical caveats: drowsiness - take at night, anticholinergic dry-mouth, and mild orthostatic drops; dose-titrate over a week from 100 mcg to avoid a “hung-over” feel.)
Until then, oscillating between “underpowered” and “epinephrine dump” is common. Forewarned is forearmed: frequent small meals with complex carbs and fat, gentle aerobic work (appropriate levels of walking, etc.) to retrain β-oxidation, and cautious use of α₂ agonists or low-dose β-blockers can soften the swings while the receptors crawl back to baseline.
This area of homeostasis reset can be challenging and without awareness, it can easily create another loop / trap. Don't fall into it.
In this protocol, restoring homeostasis starts with biochemical housekeeping. Replenishing the minerals, reducing acetaldehyde through targeted antimicrobial therapy and binders, and rebuilding queuine-producing microbial colonies can give the enzymatic machinery a chance to recover and reduce influences promoting sympathetic overdrive.
Frequent meals that pair low-glycaemic carbohydrates with medium-chain triglycerides (and/or the protocol dosing acetyl L-carnitine) helps protect the liver’s limited glycogen and spare amino-acids, while spirulina and other metabolic supports help realign cortisol timing.
As adrenergic spikes quieten, short recumbent muscle contractions or very gentle cycling become tolerable, promoting vascular conditioning without provoking post-exertional malaise. This can open up to walking and other activities as they become appropriate. A brief daily video call or other similarly "low-demand" social contact can then begin to reactivate normal reward pathways and help shift the balance towards a more parasympathetic state. Within this framework, behavioural strategies such as paced breathing or graded stressor exposure need no longer fight against biochemical headwinds and instead build on a slowly stabilising neuroendocrine landscape.
As described above, chronic disease-related lifestyle factors and trauma imprinting / autonomic learned responses to stimuli - namely stress / fear / anxiety - cause the limbic system to promote cortisol levels and inhibit the IFN-γ pathway / immune response, while decreasing glycogen stores. As this also temporarily decreases some “ME/CFS” symptoms, before rebounding, a persistent cycle of fear / anxiety, and immune dysregulation can also be learned / imprinted.
Has your life been entirely devastating for many months or years?
Have you lost nearly everything?
(Are you lonely?)
..Have you been medically gaslit (or abandoned) during this time and have therefore spent many of your days isolated from your friends, loved ones and former life, while possibly laying for long periods in your own filth and often a mouldy bedroom?
These circumstances can reliably create trauma.. and guess what? No one - literally, no one - can deal with their trauma, alone!
What you’re experiencing is what NORMALLY HAPPENS when a sensitive, intelligent system is asked to survive without the right support. Trauma isn’t imagined - the studies show it gets imprinted in cells. It alters your hormones, neurotransmitters, immune function, and even nutrient handling. This is intrinsic biology and not something to blame.
In addition to the daily trauma created by the disease, the chronic endogenous opioid synthesis pathway PRIMES the nervous system towards hyper-vigilance and rigidity -
see figure 17 and figure 18 and figure 19 on the disease model page. Preliminary data also shows that the adenosine / inosine dampening signal for extracellular ATP alarm signalling is impaired, biasing the nervous system towards hyper-vigilance and hyper-arousal.
These symptoms will normally be exacerbated during withdrawal from the endogenous opioid synthesis cascade, creating another trap, however this will need to be completed to achieve a full recovery.
If your nervous system feels like it’s running the show lately - prioritising short-term survival over long-term repair, THAT'S NOT YOUR FAULT. This is the body’s normal way of surviving / coping. However, over time and repeat exposure to stressors or trauma, your nervous system adapts to existing in this harsh environment and is often reluctant to reset the alarm system, especially if it thinks you might still be unsafe. When this happens, it needs gentle reminders to hand control back to the repair systems, after removing the metabolic crisis alarms and enough of the pathogenic burden.
The nervous system is NOT malfunctioning - it's adapting to excessive chronic stress signalling and trying its best to keep you safe.
By understanding these adaptations, we can work WITH the body to restore balance.
If you find yourself in this situation - which is entirely expected after "living" with ME/CFS or any other named entry-point to the disease model) - then getting help is essential to your recovery.
Your nervous system sends "predictions", not "facts"
It can be helpful to understand that your nervous system is not a neutral, unbiased reporter. It doesn't state "facts". It has a pattern-matching threat predictor function, with a primary goal of keeping you safe. It continually guesses what is about to happen next and prepares you in advance.
When you've had a history of chronic illness, trauma, or prolonged stress, that prediction system can be primed by biochemistry and threat priors to run a “better safe than sorry” program - it overestimates danger and underestimates your capacity to cope, giving you a false and limiting perception of real life.
That program shows up as thoughts like:
“This is unsafe.”
“I’m going to fail.”
"This will hurt me."
“This isn’t the right time.”
“I can’t do this.”
“This will go wrong.”
“If I don’t do X, I’ll be unsafe.”
.. and it is NOT just thoughts - a threat prediction from the nervous system can recruit the whole body to make you really FEEL the message, too. The thoughts may be potentially accompanied by eg. tight chest, nausea, adrenaline dumps, difficulty swallowing, GI upset, immune system activation, mast cell activation, gnawing sensations in the stomach, "stomach drop", weakness, fatigue, pain spikes, breathing difficulties, even panic.
Those sensations and their related biochemistry are completely real and measurable.. however, the BIGGER question is whether the nervous system's prediction is really accurate, or often (without a lot of NEW life experiences to recalibrate from), largely based on OLD fears, OLD traumas, OLD patterns, or OLD emotionally-charged memories… which don't relate to what’s actually happening RIGHT NOW.
"The trap" is treating the ALARM as a true verdict, or FACT, rather than just a PREDICTION.
To move forward from this trap, treat the alarm signal instead as a hypothesis and allow for the idea that your nervous system is running on incomplete and outdated data.
Predictions can be challenged.
Predictions can be tested.
Predictions are not reality.
Next time, you can try this, in the moment:
Ask, “Is this a FACT, or is this my body running a threat PREDICTION?”
Name the prediction, out loud, in one sentence: “My nervous system predicts X will happen.”
Then choose one small, safe test: a 30–120 second action that gathers new evidence (eg. stay in the situation, take one step, send the message, stand up, walk to the door, do the first minute, write the first sentence).
(Nose-breathe slowly, deeply and deliberately throughout the test. Try to keep your nervous system in a parasympathetic state.)
Baby steps. With each successful test, you’re updating the threat-prediction model data and recalibrating the nervous system.
Another good, cheap literary resource - if you want an accessible, non-technical introduction to these systems is "Don’t Believe Everything You Think", by Joseph Nguyen. [Book link]
Trauma counselling / therapy, EMDR, vagus nerve stimulation and various other interventions can also be game-changing for some people who are suffering from chronic "fight or flight" programming induced by complex trauma and chronic illness. A 19 page, downloadable ChatGPT-generated "Deep Research" report on the latest evidence for different interventions as of August 2025 can be found here.
Stellate Ganglion Blocks (SGB) can be another helpful intervention, by resetting and controlling this state, however they are not a long-term solution, unless you use them as a helpful educational tool, to experience a period of remission from the crisis state, which helps you learn to rebuild trust in your body. NB. SGBs should not be used until the underlying issues causing hypometabolism are resolved, otherwise you'll feel like you've taken a backwards step in functionality. The crisis state is providing a level of energy to sustain you, even if that's dysregulated.
However, this protocol also describes an anxiety -> phobic response trap that can cage people and ways to navigate this successfully. From my observations, this affects a significant number of people.
If you are affected by this subconscious programming, you will struggle to make forward progress while still in a chronic "fight or flight" state, due to the downstream metabolic consequences:
The "fight or flight" and/or "crashed" state may also lead to low glycogen and significant amounts of lactic acid and oxalates being generated. If the lactic acid can't be metabolised efficiently to usable energy, this can cause swollen / inflamed / numb / tingling body parts, especially in areas with smaller blood vessels, such as hands, feet, face and lungs.
Lactic acidaemia can also make it very difficult to restore zinc, electrolytes and missing bacteria which are pH sensitive, eg. bifidobacterium and butyrate producers, as excess lactic acid is secreted into the GI tract and also via your kidneys, leading to frequent urination, "sandy urine", kidney stones, etc.
If you are feeling lost or in a crisis, THRIVE Lifeline offers 24/7 international text-based crisis support to anyone aged 18+, with a specific focus on multiple marginalized communities. They do not engage in non-consensual "active rescue" and they prioritise the texter's consent + autonomy.
For urgent help
SMS: +1.313.662.8209
General enquiries
Website: https://thrivelifeline.org/
Email: info@thrivelifeline.org
"Anxiety", isolation, and phobia
Before continuing, for clarity, I'll restate my previously published, long-standing position against using CBT and GET as a primary therapy for ME/CFS and similar diseases:
I anticipate that there is a special place in hell reserved for clinicians who negligently misdiagnose ME/CFS patients with a purely psychological disease or "anxiety", or force patients with measurable mitochondrial dysfunction from chronic infections / dysbiosis / induced malnutrition to perform "graded exercise".
You wouldn't initially prescribe a diagnosed septicaemia patient CBT and GET as their primary therapy, so it's appalling that this continues to be the "gold standard approach" taken by numerous clinicians for ME/CFS patients. There are decades of evidence against this.
Yes, once the infections and malnutrition are sufficiently resolved and mitochondrial metabolism allows for it, physical rehabilitation is absolutely encouraged as part of the recovery process.
Yes, there are neurological and psychological issues created in this disease model - biochemically and from trauma, isolation, coping mechanisms and learned fear responses. These each require different interventions.
[/RANT]
This section explores the connections between "anxiety", isolation, and phobic responses to symptoms in individuals with ME/CFS or similar chronic diseases. Drawing on parallels between chronic pain, fibromyalgia and ME/CFS, it aims to provide a clearer understanding of these challenges and how to exit another closed-loop / cycle which can be present in some patients.
Understanding the fear-avoidance cycle
A fear-avoidance model, initially developed in the context of chronic back pain by Dr Sarno as "Tension Myositis Syndrome (TMS)" and later extended by Dan Buglio as "Perceived Danger Pain (PDP)", also provides a working description for an observed pattern of daily experiences, physiological responses and behaviour that may create a further trap for some people already suffering from ME/CFS and precursor states on the slippery slope described by the disease modelling.
A popular example of perceived danger pain is the "Rubber Hand
Illusion" - a psychological experiment that demonstrates how the brain
can be tricked into perceiving a fake hand as part of one's own body. In
this setup, a participant's real hand is hidden from view, and a rubber
hand is placed in front of them. Both the hidden real hand and the
visible rubber hand are simultaneously stroked with brushes. Over time,
many participants begin to feel as though the rubber hand is their own.
This illusion highlights the brain's ability to integrate visual and
tactile information to create a sense of body ownership. https://youtu.be/sxwn1w7MJvk
In chronic pain, the fear of pain or "perceived danger pain" can lead to avoidance behaviors, which ultimately reinforce fear and reduce / prevent pain-free movement. The brain creates a genuine sensation of pain and measurable metabolic alterations to a perceived danger, to try and keep you safe. This is described as a learned phobic response that happens even when the original danger has been removed.
https://journals.lww.com/pain/fulltext/2022/08000/impaired_pain_related_threat_and_safety_learning.18.aspx
Similarly, some people with ME/CFS may fear pain from triggering or exacerbating existing metabolic symptoms such as mast cell activation syndrome (MCAS), post-exertional malaise (PEM), inflammation, sleep deprivation, etc, leading them to increasingly avoid foods, supplements and people, along with physical and mental activities. This avoidance can result in severe deconditioning, increased isolation, and a greater severity of symptoms, perpetuating a closed-loop / cycle of fear and avoidance.
Notably, even the possibility of avoiding discomfort can paradoxically increase fear over time. Studies show that individuals who are given the option to avoid pain experience increased fear when that option is removed, highlighting how avoidance can amplify anxiety rather than reduce it.
https://academic.oup.com/abm/article-abstract/55/3/216/5876277
Stress, isolation, and heightened threat response
Heightened threat-perception and response is a significant factor for individuals "living" with ME/CFS, similar to its role in chronic pain. People with ME/CFS often experience heightened anxiety, too - created by the mitochondrial dysfunction and downstream energy crisis. Neural hypoxia can be one of the more common influences, downstream of immune activity, impaired iron homeostasis, oxidative stress, blood-flow and structural issues.
Additional stress can also sometimes be driven by feelings of inadequacy and/or fear from not being able to participate in life and fulfil roles as parents, lovers, workers, or friends. This anxiety is often compounded by fear of the unknown, thanks to inadequate medical care and also anticipatory fear - worrying about potential symptoms exacerbation by taking even small actions. This leads to heightened stress and worsened symptoms.
Isolation and unrefreshing sleep further intensifies this stress. For those with ME/CFS, reduced social contact can enhance the brain’s threat-detection systems, making individuals more likely to interpret normal bodily sensations as signs of danger. Studies indicate that even brief periods of social isolation can increase vigilance to perceived threats, which contributes to the cycle of fear and avoidance.
https://royalsocietypublishing.org/doi/10.1098/rsos.240101
Moreover, as a "perceived danger syndrome", symptoms related to immune activity and die-off, such as inflammation, pain, elevated histamine, rashes, nausea, diarrhoea or flu-like sensations, can be misinterpreted by the brain as a danger signal.
It sounds rather incredible, however mere perception of a threat can alter biology before any contact. In humans, simply anticipating an “infectious” other in virtual reality engages peripersonal-space and salience networks, tightens coupling with the hypothalamus, and transiently shifts innate lymphoid and NK-like cell frequency and activation. In plain terms, prediction alone briefly primes the immune system and readiness circuits, even without a pathogen present.
https://www.nature.com/articles/s41593-025-02008-y
Repeated or uncontrollable threats write a slower trace in limbic circuits. In rodent stress paradigms, extracellular ATP accumulates in the hippocampal microenvironment, activates microglial P2X7, assembles the NLRP3 inflammasome, and increases IL-1β. causing microglial-driven neuroinflammation and behavioural output. Blocking P2X7 or deleting NLRP3 prevents the behavioural phenotype. Translation: ongoing stress can lock in an inflammatory signal in brain immune cells that sustains hypervigilance. (See Figure 19.)
https://www.sciencedirect.com/science/article/abs/pii/S0006322315010367
Top-down outputs then signal for gut microbiome alterations within hours. Chemogenetic activation or inhibition of hypothalamic AgRP or POMC neurons, or central leptin or ghrelin, rapidly re-tiles intestinal microbiota in mice within 2-4 hours, independent of food intake. This is a fast autonomic channel by which threat state can alter microbial metabolites that feed back to glucose handling and inflammatory thresholds.
https://www.nature.com/articles/s42255-025-01280-3.pdf
Early-life experiences set priors that change how the loop runs. In a longitudinal cohort, toddler microbiota composition predicted resting-state network architecture at age 6, which in turn tracked internalising symptoms at 7.5 years. The mediation via the connectome puts the brain in the middle of a gut-to-brain-to-behaviour cascade. This evidence is early, however the direction is consistent.
https://www.nature.com/articles/s41467-025-64988-6
Surprisingly, trauma and threat experiences can be narrowly encoded across generations. Paternal odour-fear conditioning in mice produced cue-specific sensory hypersensitivity and glomerular enlargement in 8 generations of offspring, with hypomethylation at the matched olfactory-receptor locus in sperm. That implies inherited, feature-specific threat priors can raise threat-detection circuit gain before any new learning.. which reminds me acutely of the saying "you either face your demons or they raise your children".. and great-[..]-great-grandchildren.
https://pmc.ncbi.nlm.nih.gov/articles/PMC3923835/
Severe trauma also leaves a durable systems imprint even when symptoms are less obvious. Years after a mass-trauma event, medically healthy survivors showed higher IL-1β, lower IL-2R, lower morning cortisol, higher resting diastolic blood pressure, and blunted cardiovascular reactivity to trauma scripts, with weak coupling to current PTSD or depression scores. This means our biology can remain shifted while conscious distress abates.
https://www.cambridge.org/core/services/aop-cambridge-core/content/view/C5935399886A5B10F0EBD55C6C7B0F4A/S1049023X24000360a.pdf/learning-from-hindsight-examining-autonomic-inflammatory-and-endocrine-stress-biomarkers-and-mental-health-in-healthy-terrorism-survivors-many-years-later.pdf
This heightened threat perception can create a nervous system feedback loop, as a form of dysautonomia, where normal metabolic processes, eg. immune responses are seen as threats, further elevating stress levels and acting as a "fight-or-flight" trigger, chronically depleting glycogen stores, activating altering blood-flow and potentially leading to avoidance behaviors.
This misinterpretation by your subconscious brain reinforces the fear-avoidance cycle, making it more difficult for people to break free from the loop of symptom exacerbation and fear. The nervous system can create real, measurable symptoms of physical pain and emotional fatigue in the process of keeping you safe.
How this loop sustains itself
Perception of a threat creates inflammation
Anticipatory salience plus limbic extracellular ATP, P2X7 and IL-1β signalling amplify salience for the feared cue. Avoidance then prevents corrective exposure and keeps the prior high.
Metabolic bias
Sympathetic tilt, mast cell activation and cytokine signalling favour rapid glycogen mobilisation and transient insulin-resistant windows, along with histamine-related symptoms.
Gut feedback
Hypothalamic outputs acutely shift proximal-gut communities and metabolites, modulating adenosine and inflammasome thresholds that influence microglial reactivity and threat learning.
The phobic response to symptoms
"Do not be bluffed by a symptom.
Accept it. Float through it.
Let time pass." - Claire Weekes, MD
The pattern I call the "phobic loop" has deep roots in biology -
trauma, metabolism, inflammation, sensory gating. However, the
experience of being trapped in that loop isn't new.
Decades ago, a
brilliant Australian physician named Dr. Claire Weekes described a nearly identical cycle [BOOK LINK - highly recommended],
using language like “first fear, second fear,” and explaining how a
sensitised nervous system can become stuck in protective sympathetic overdrive. She
wasn’t simply dismissing symptoms - instead, she was validating them. Her key insight was that the fear of the symptom was more disabling than the symptom itself.
What
she offered patients was a way to float through the storm - not by
ignoring it, but by removing the "fuel": the resistance, the bracing,
the fear of fear. There are similarities to key elements in this section
- restoring safety to the system, not by silencing it, but by helping
it stand down.
Repeated experiences of PEM, MCAS, etc., can result in a conditioned, phobic response to certain triggers. This means that the brain starts to associate specific activities - such as physical exertion or even mental tasks - with symptom exacerbation, leading to an increased fear response. The brain, in a state of chronic stress or "under siege", may misinterpret normal sensations as threats, reinforcing feelings of vulnerability and the development of phobic responses to a wide range of stimuli.
People with strong ADHD and/or OCD-like traits are expected to have a
more difficult time with this, as the subconscious hyper-focus and
pattern-recognition traits can easily be fixated on the symptoms,
instead of the recovery progress. As an analogy, I'm reminded of a lesson once given by my motorcycle riding instructor:
When
riding a motorcycle, you seamlessly "merge" with the bike, to the point
that wherever you're looking is where the bike will travel towards.
Imagine a scenario where you're riding a motorbike around a large
paddock that has a single tree in the middle of it. The paddock is so
large that there is absolutely no reason that the tree should present a
significant risk of collision - you have a lot of wide open space to
enjoy. However, if you're consciously or subconsciously afraid of
hitting the tree, you'll keep glancing or looking over at it to make
sure you're safe. Consequently, by these actions, you'll increase the
risk of actually hitting the tree, or perhaps succeed in doing so. By
simply focusing on the wide open space where you want to actually be
riding, you will be significantly safer and enjoy your ride more.
This lesson applies to ME/CFS in the same way: don't focus on the symptoms - focus on the destination. Trust your body. The symptoms that we worry about the most may persist the longest. We give energy and life to things by paying attention to them.
It's important to understand that your symptoms are NOT imagined - they’re real, measurable, and rooted in biology. Whereas, HOW your nervous system INTERPRETS and AMPLIFIES those symptoms can change the entire trajectory of the illness.
In other words, it's NOT "in your head", it's "through your nervous system" ...and that gives us tools to work with.
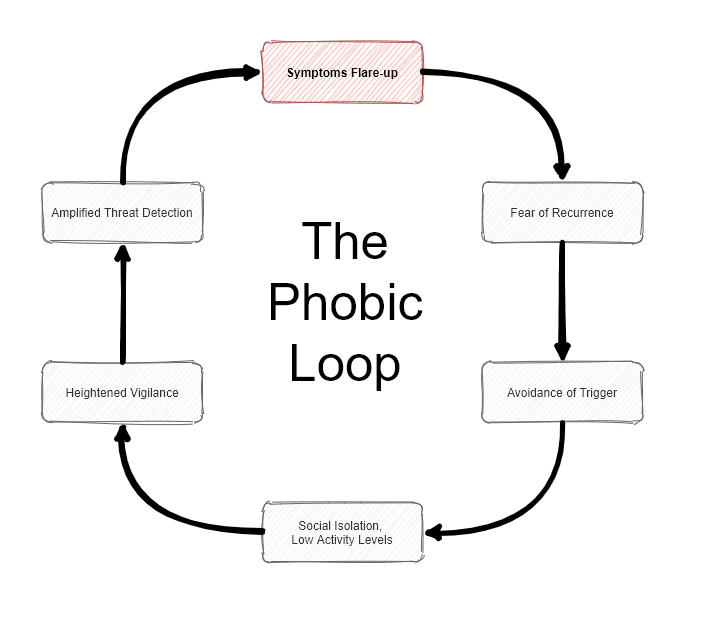
The loop is debilitating, but not irreversible. Every loop has a way out - and that’s what this section is about.
Steps towards recovery
Several strategies can help people with ME/CFS, etc., navigate the complex interplay of physical, neurological and psychological symptoms:
Recognising the Role of the Mind
Understanding the powerful connection between the mind and body is crucial. Unregulated fear can perpetuate symptoms, so addressing these emotions is an essential part of recovery.
Perceptual Recalibration
Graded stressor exposure with interoceptive control to reduce salience-hypothalamus coupling to the cue. Expect the transient innate lymphoid cell signature to normalise as exposure succeeds.
Purinergic Damping
Aim to lower extracellular ATP signalling or raise adenosinergic tone conceptually. This is an area being actively researched. Early data suggests the inosine + adenosine synthesis, which acts as the dampening signal to extracellular ATP is dysregulated by impaired glycolysis, pentose phosphate pathway, methylation, acidosis and low glutamine:glutamate. Inosine is included in the protocol to help regulate this imbalance.
Autonomic Gating
Slow nasal-breathing or baroreflex-oriented work to raise RMSSD and blunt post-prandial adrenergic spikes, then re-test symptom provocation.
Gut Microbiome Modulation
Increasing fermentable-fibre intake and other microbiota-supportive tactics in the post-exposure window can exploit the short hypothalamus → microbiota latency and stabilise feedback metabolites.
Daily Mantras / Replacing Unhelpful Thoughts
This can help re-frame negative thoughts and beliefs about symptoms, thereby removing unnecessary obstacles, fears and anxiety, eg.
1. "This is a chapter in my life, not the whole story."
This
mantra puts the illness experience into perspective, reminding people
that their lives are not defined by their symptoms. It encourages them
to look beyond the present moment and envision a future filled with
possibility. It helps to counteract the sense of hopelessness that can
accompany chronic illness. It reminds people that their lives are still
unfolding and that their illness, while a significant challenge, does
not have to define their identity or their future.
2. "I choose to focus on what I can do, not what I can't."
This
mantra promotes a positive outlook and encourages individuals to find
joy and fulfillment in the present moment, even within the constraints
of their illness. This affirmation helps to shift attention away from
limitations and towards possibilities. It encourages people to explore
activities that bring them joy and a sense of accomplishment, however
small, to counteract the sense of loss and frustration that can
accompany chronic illness.
3. "Every step I take, no matter how small, is a victory."
This
mantra celebrates small wins and acknowledges the courage it takes to
move forward even when faced with fear and uncertainty. It encourages
people to appreciate their efforts, no matter how seemingly
insignificant. It emphasizes that progress is not always linear and
that even small steps forward contribute to overall healing.
4. "I am not alone in this journey."
This
mantra reminds people that they are part of a larger community of people
who understand their struggles. It helps to combat feelings of
isolation and foster a sense of belonging. It underscores the importance
of connecting with others who have experienced the challenges of living
with ME/CFS. Sharing experiences, offering support, and learning from
one another can be a powerful source of healing and hope.
5. "I am learning to listen to my body with kindness and curiosity."
This
mantra encourages a compassionate and non-judgmental approach to
symptom management. It fosters a sense of collaboration with the body
rather than seeing it as an adversary. This affirmation helps to shift
the internal dialogue from one of self-criticism and blame to one of
understanding and acceptance. It encourages people to pay attention to
their body's signals and respond with care and compassion.
6. "My body is healing, even when I can't see it."
This
mantra fosters patience and hope, reminding people that recovery is a
process that may not always be visible. It encourages trust in the
body's innate capacity to heal. It helps to counteract the
discouragement that can arise when progress feels slow or setbacks
occur. It reminds people that healing is happening on multiple levels,
even when it's not immediately apparent.
7. "My symptoms are a signal, not a sentence."
This mantra helps to re-frame symptoms as messengers rather than threats. It acknowledges that symptoms are trying to communicate something, but they don't dictate the future or define one's limitations. It draws on the idea that pain, fatigue, and other symptoms in ME/CFS are often amplified by fear and anxiety. It encourages a shift in perspective from viewing symptoms as inherently dangerous to seeing them as signals that need to be understood and addressed.
8. "I am safe, even when I experience symptoms."
This mantra directly addresses the fear response, offering a powerful message of reassurance. It emphasizes the distinction between experiencing a sensation and being in actual danger. It is particularly helpful in breaking the cycle of fear and avoidance. By repeating this affirmation, people can begin to retrain their nervous systems to associate symptoms with safety rather than threat.
9. "I am stronger than my fear."
This mantra
empowers people to face their fears and challenge the limitations they
have imposed on themselves. It emphasizes that fear does not have to
control their lives. This affirmation promotes self-efficacy and
encourages individuals to take an active role in their recovery. It
reminds them that they have the inner strength to overcome their fears
and gradually expand their boundaries.
These mantras, when repeated regularly and with intention, can help to rewire the brain's threat response, reduce anxiety, and foster a sense of safety and empowerment in the face of challenging symptoms. With practice and persistence, belief in these mantras strengthen. It only takes a few wins or reductions of something to see this approach is helping.
Gradual Exposure and Pacing
Gradually increasing exposure to normal activities and day-to-day life, along with appropriate pacing, can help desensitize the nervous system and break the fear-avoidance cycle.
Emotional Processing
Techniques such as journalling, therapy, or other methods for exploring and expressing emotions can be key in addressing underlying emotional issues that may contribute to symptom persistence. Recovery is not linear. Record your wins as a list. On bad days go back to the listed wins list and focus on the positive.
Somatic Practices
Practices like mindfulness, gentle movement, and breath-work can help people with ME/CFS develop a greater sense of safety and connection with their bodies, shifting the nervous system from sympathetic to parasympathetic mode.
Try this:
Place your hand over your chest and breathe slowly into your ribs for 10 seconds.
As you exhale, say (in your head, or aloud): "I’m safe. I’m adaptive."
Happily, this isn't about "magic thinking" - it's reprogramming the body's fear interpretation loop through safe, predictable signals.
Self-Compassion
Cultivating patience and kindness towards oneself during the recovery journey is crucial, as ME/CFS recovery can be a slow, non-linear and challenging process.
Building Social Support
Connecting with others who understand the experience of ME/CFS and critically, are supportive of the process you are undertaking and / or are ideally further along the same recovery process than you, can reduce feelings of isolation, provide validation, and offer emotional peace.
Recovery from ME/CFS is a deeply personal journey of "putting Humpty Dumpty back together again". Everyone has slightly different shaped pieces to reassemble.
As part of normal female reproductive health, oestradiol normally elevates on days 10–12 and 22–26 of the menstrual cycle. This decreases cortisol levels and promotes IFN-γ activity. Without chronic infection, these alterations would allow for increased energy availability and libido. With chronic infection, these alterations allow for increased immune activity, pain / inflammation in infected tissues, neurological and emotional challenges, etc. Conversely, oestradiol is low on days 1–8, allowing cortisol to increase – decreasing immune activity and increasing anxiety.
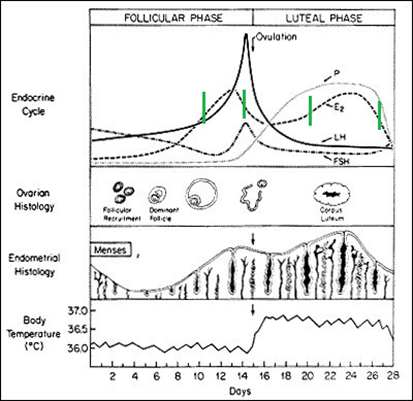
[source: Feingold KR et al., editors. South Dartmouth (MA): MDText.com, Inc.; 2000-.]
Both of these situations are ultimately helpful, long-term. However, no one enjoys the symptoms of immune activity. Supplements like DIM, found in broccoli and calcium d-glucarate can help reduce the effect of these hormonal alterations.
Metabolism described in this disease model can significantly influence urinary tract infections by weakening the immune system, promoting bacterial growth in the urinary tract due to elevated glucose levels, renal excretion of oxalates, impaired nerve function and bladder emptying.
Similarly, pathogenic species found in the nasopharynx, oral, gut and other microbiomes may translocate or be transferred to urinary and sexual organs, potentially leading to further sexual dysfunction, pain and inflammation.
This may be more prevalent in PSSD, PCOS, endometriosis, cystitis, prostatitis and epididymitis sufferers, however dysbiosis and biofilm formation in urinary and sexual organs is generally found across the entire scope of chronic diseases.
For renal and urinary tract infections, methylene blue protocols and the ‘purple foods’ containing anthocyanins may be particularly relevant. Elderberries and chokeberries appear to be the richest sources of anthocyanins and will provide the same benefits in other tissues. Bacteriophages and protective probiotics can be extremely helpful.
Sleep is often viewed as a simple daily routine, but it is far more than just rest for the body and mind. It is a complex and essential physiological process that plays a pivotal role in maintaining overall health, particularly when it comes to the brain.
Sleep is a naturally recurring state of altered consciousness and decreased physical activity. It is divided into several stages, including non-rapid eye movement (NREM) and rapid eye movement (REM) sleep, each serving different purposes in the sleep cycle.
Dopamine is a neurotransmitter that plays a vital role in mood regulation, motivation, and reward systems in the brain. However, the metabolism of dopamine produces toxic by-products. If these metabolites accumulate excessively, they can lead to oxidative stress and damage to brain cells.
The glymphatic system is a relatively recent discovery that has revolutionised our understanding of brain health during sleep. This system acts as the brain’s waste clearance system, similar to the lymphatic system in the rest of the body. It operates primarily during sleep and is responsible for removing metabolic waste products from the brain.
Melatonin is a hormone produced by the pineal gland in response to darkness. It plays a crucial role in regulating the sleep-wake cycle. Melatonin levels rise at night, promoting the onset of sleep and maintaining sleep duration. What’s fascinating is that melatonin has been shown to enhance the efficiency of the glymphatic system during sleep. It does this by causing a temporary contraction of brain cells, which allows cerebrospinal fluid to flow more freely, aiding in the removal of waste products. Oxytocin -> Prostaglandin F2α signalling also controls glymphatic activity.
https://www.nature.com/articles/s43587-024-00691-3
When we don’t get enough sleep, the glymphatic system’s efficiency is compromised. This can lead to the accumulation of toxic metabolites in the brain. Over time, this build-up can contribute to cognitive decline and increased risk of neurodegenerative diseases like Alzheimer’s, Parkinson’s and severe mood disturbances.
To benefit from this natural brain-cleansing process, it’s essential to establish a healthy sleep routine. Aim for 7–9 hours of quality sleep per night, starting ideally before 10pm. Maintain a consistent sleep schedule, create a comfortable sleep environment, and limit exposure to blue light from screens before bedtime.
The protocol targets issues which cause low serotonin, GABA and high cortisol levels at night, preventing quality sleep. If you fall asleep and wake up quickly with myoclonic jerks, you may have a calcium or other electrolyte deficiencies, hypometabolism as energy insufficiency from catabolic pathways and/or liver glycogen, and/or respiratory depression / airway restrictions. Another influence is low vitamin C from oxidative stress, further inhibiting dopamine beta hydroxylase, the enzyme which makes norepinephrine from dopamine. This is more likely to occur with increased immune activity and/or exertion. Low glycogen can reliably cause cortisol increase and is one of the major influences in post exertional malaise.
Hypometabolism can also occur during rapid microbiome changes and withdrawal from microbial / endogenous alcohol -> acetaldehyde -> morphine and/or GHB, see ("2.3.4 Rapid withdrawal symptoms, hypo/hyper-metabolism").
Following the dietary guidelines, plus correcting chromium, vanadium and other deficiencies will help prevent this.
One of the hallmark symptoms of ME/CFS, Long COVID / Long Haulers and various other named syndromes is post-exertional malaise (PEM).
The disease model shows that exertion promotes IFN-γ and oxidative stress, which further inhibits glycolysis, fatty acid oxidation, methylation and other key energy metabolism. Simultaneously, histamine is released during exertion, signalling for liver glycogen to be redistributed to muscle tissue.
Part of the glycolysis impairment relates to inhibited liver glycogenesis (glycogen synthesis). This is acutely influenced by epinephrine in response to the energy crisis, however there are additional "background" influences from elevated microbiome-related acetaldehyde and various cofactor + nutrient deficiencies. This part of the disease cascade is described as a reversible liver glycogen storage disease.
Glycolysis insufficiency is frequently accompanied by tinnitus, vision reduction, dizziness, reduced mobility / muscle activation, muscle spasms / tremors, tachycardia and nausea.
The protocol addresses these upstream influences and the glucose uptake and glycolysis rate has been shown to improve / revert, however some daily variability around glycogen usage will exist relative to your exertion and immune activity levels.
During increased exertion and/or (downstream) immune activity, energy consumption also increases and creates oxidative stress, hence your carbohydrate and protein intake may need to be increased to match your glycogen expenditure. This would normally be additional carbohydrates, protein as additional small meals over the day, and a large additional intake of vitamin C and/or other antioxidants.
However, in a crash / PEM, the priority is restoring liver glycogen (and sodium) levels. Spoonfuls of NZ Manuka honey are one of the least risky sources for simple carbohydrates, as it has an antimicrobial profile thought to be related to the methylglyoxal content and various phenols. H1 antagonists like doxylamine succinate can also be helpful, especially before sleep - as they normally cause drowsiness.
You can also target restoration of energy availability and glycogen synthesis via alternative pathways, if they are functioning. These pathways may include (non-exhaustive):
- Branched-chain amino acids (BCAAs) catabolism. BCAAs are found in dietary protein sources. BCAA catabolism requires sufficiency of manganese, Vitamin B1 (as thiamine pyrophosphate), P5P, biotin and Vitamin B12 (as adenosylcobalamin, for 2 of the BCAAs - L-leucine has a different pathway). Assuming you are supporting these co-factors with the protocol, you can simply take 5-10g of BCAAs or L-leucine alone to rapidly help initial recovery and then increase carbohydrates and/or protein to prevent reoccurence.
https://www.bulksupplements.com/search?q=bcaa - Ketogenesis - supplying beta-hydroxybutyrate (BHB). This pathway requires phosphatidylcholine (PC) and NAD+ sufficiency. Assuming you are supporting phosphatidylcholine and NAD+ biosynthesis and redox with the protocol, you can also take 10–20g of a BHB supplement, as needed to help recovery and then increase carbohydrates and / or protein to prevent reoccurrence.
https://www.bulksupplements.com/search?q=hydroxybutyrate
If you have an asthma inhaler (salbutamol), it can be very helpful to increase catabolic activity and provide emergency energy availability for a period of time, but may also inhibit glycogen storage, where insulin is not elevated (between meals), so should not be used frequently and should be accompanied by frequent carbohydrate intake for glycogen repletion.
For best results, this schedule should be printed, laminated and ticked off with a whiteboard marker, each day.
Note that this schedule has been prepared using the compounded nutrients, DIY "shake" and "sipper" recipes. Details for these can be found in the "4.2 Compounded nutrients", "4.3 DIY shake and DIY sipper" and “5 Ordering products”
sections.
These preparations significantly reduce the daily complexity and
cost of the protocol, however it is also still possible to utilise individual
supplements. Links to those products are also provided in “5 Ordering products”.
However, if you aren't planning on using the compounded nutrients, and / or DIY shake, you will instead need to optimally schedule a large array of individual products. (An alternative for the DIY sipper is not provided, or suggested.)
Powders with smaller doses, eg. <500mg, can be accurately measured using the milligram scales and small metal spoons listed in the protocol's products schedule. Powder density varies by compound and vendor. However, once you have used the milligram scales to initially identify an appropriate spoon size and serving amount, eg. 50mg of uridine monophosphate might approximate a full 1/64th tsp, you'll then be able to quickly use that serving spoon to measure out future doses, without needing to weigh them again.
For sublingual dosing of powders, eg. uridine monophosphate, NAD+, NADH, etc., they can be placed under your tongue using the metal spoon and left to quickly dissolve.
Details for these alternative schedule options are provided here:
2.3A Alternative daily supplement schedule - [no compounded nutrients] - (if you intend on using the DIY shake recipe and not the compounded nutrients)
2.3B Alternative daily supplement schedule - [no DIY shake] - (if you intend on using the compounded nutrients and not the DIY shake recipe)
2.3C Alternative daily supplement schedule - [no DIY shake or compounded nutrients] - (if you intend on not using the compounded nutrients or the DIY shake)
.. please be aware, these schedules are considerably less convenient.
Stage 1: Remineralisation, increasing collagen synthesis rates and performing a controlled initial “die-off”
This stage will typically last at least two weeks and can be initially unpleasant due to the microbial “die-off” effect – even though it is being minimised by various supplements.
If necessary, slow things down, as needed / use reduced doses and build up. If tolerated, 100mg/day aspirin can be helpful at this stage to help inflammation / hypoxia.
However, many items are complementary to each other, therefore moving too slowly during Stage 1 implementation may lead to an unsupported / unsustainable increase of immune activity, ultimately reducing energy availability and leading to lower glycogen and increased oxidative stress induced damage.
Stage 2: Increased GI / mucosal interventions
Whilst continuing all items from Stage 1, add the following elements. Note that the Stage 1 DIY sipper and shake recipes are replaced with a Stage 2 DIY sipper and shake recipes that contains additional ingredients.
Stage 2 is expected to trigger additional gastrointestinal immune activity, which is likely to be observed as diarrhoea lasting a few days and sometimes nausea. Extra water and diosmectite / Diarelieve may be a useful binder during this time.
https://wikipedia.org/wiki/Diosmectite
A high-dose methylene blue protocol (ie. not the microdosing used for NAD+ redox) is being tested as a Stage 2 intervention.
https://bornfree.life/download/methylene_blue_protocol.xlsx
If your doctor has prescribed any anti-fungals and/or antibiotics, Stage 2 is the most appropriate place to introduce them.
However, these may have an impact on your existing efforts to restore microbiome diversity – some additional focus on probiotics, prebiotics and diet may be required. Ideally, any antibiotic use should be followed by Biomesight and/or other microbiome reports.
When you have completed Stage 2, repeat an Oligoscan / CMA + OAT test and don't proceed to Stage 3 until you have confirmed successful remineralisation. Similarly, iron status via standard pathology should be confirmed, if needed - iron, ferritin, transferrin saturation%, transferrin.
Stage 3: Stimulate and support a strong immune response
This stage will typically require 4+ weeks.
Important: confirm successful repletion of copper, zinc, selenium and manganese via CMA / Oligoscan and iron status via blood tests before proceeding to this stage.
Do NOT proceed into Stage 3 if you still have a low lactate threshold, evidenced by eg. low phosphate, sulphur (Oligoscan / OAT),
Do NOT proceed into Stage 3 if you are battling with food and/or supplement intolerances, PEM, POTS or if there is still significant microbiome dysbiosis.
Failure to observe these logical gates when entering Stage 3 is likely to generate an inappropriate level of immune activity vs host capacity, leading to metabolic acidaemia / acidosis and downstream mineral losses in the cascade, ie. NEGATIVE BASELINE SHIFT. (see Figure 12)
If your cortisol / heart rate becomes elevated for long periods (>6 hours), or immune-related tissue pain/inflammation extends beyond 3 days per localised tissue, take a few days off the mushrooms, double the vitamin C and simultaneously decrease spirulina to 500mg during this “recovery break”. 100mg aspirin may again be helpful.
Expect temporary die-off symptoms, heavy immune response, pain / inflammation, POTS, fatigue, nausea, diarrhoea, headache, etc.
You will likely feel temporarily worse than your pre-protocol baseline, as the intensity of the innate immune response induces most of the ME/CFS symptoms. This may add some additional psychological challenges to this stage.
Continue items in all previous stages, apart from any minerals now measuring as “Normal+” on the Oligoscan report. Whilst continuing all Stage 1 and Stage 2 items, add the following elements. Note that the Stage 2 DIY sipper and shake recipes are replaced with a Stage 3 DIY sipper and shake recipes that contains additional ingredients.
Acetaldehyde is one of the primary toxins released during microbial die-off events and also in smaller amounts, multiple times per day, in response to normal dietary intake of nutrients. Our food intake also feeds our resident microorganisms – including the pathogenic species – which allows them to produce (toxic) metabolites and poison us following each meal.
Acetaldehyde potentially places a difficult burden on our metabolism in key places – histamine degradation, neurotransmitter degradation, collagen synthesis, carnitine synthesis (needed to transport longer chain fatty acids), fatty acid degradation, glucose transport and glycolysis, GABA metabolism, choline metabolism, methylation, vitamin B6 degradation, vitamin A metabolism, lysine degradation, pyruvate metabolism and many other pathways.
Countering that, in appropriate doses, it appears to function as an antidepressant - by slowing down the neurotransmitter degradation pathway and triggering endogenous morphine + GHB synthesis. (see 2.3.4 Rapid withdrawal)
It also functions as an exertion mimetic, by increasing the mitochondrial NADH pool level for Complex I to take electrons from and feed the electron transport chain. (see 2.2.4 The importance of pacing and Figure 14)
Aldehyde dehydrogenase enzymes (ALDH2, 1A1, 1A2, etc.) detoxify acetaldehyde into acetate as a priority over their normal substrates due to the kinetics involved. This means that these enzymes are the primarily affected reactions by chronic acetaldehyde and this will initially create a number of metabolic impairments to important pathways. This may be observed as eg. elevated LDL cholesterol, elevated serum vitamin B6, elevated histamine, elevated retinol / beta-carotene and an array of symptoms.
However, having low NAD+ as a result of chronic IFN-γ
activity, and/or
inhibited NMNAT activity (eg. low cAMP-PKA, oestradiol, MAPK)
exacerbates this problem significantly, creating a loop / trap and extends the impact to a wide
range of important enzymes requiring NAD+ as a cofactor.
As ALDH normally requires NAD+ (and magnesium, zinc), this also includes the majority of ALDH isoforms, affecting a wider array of aldehyde metabolism.
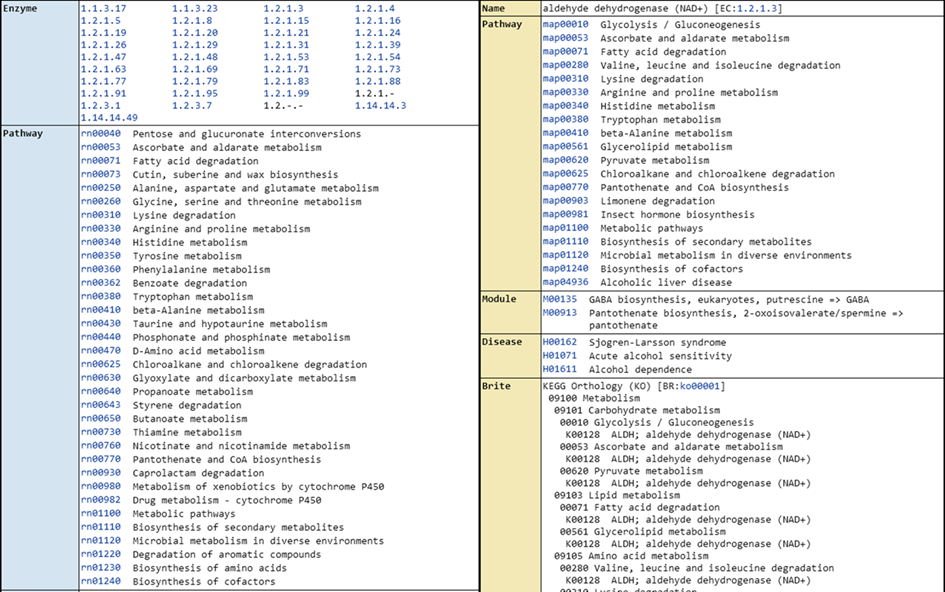
Taurine, NAD+, magnesium, zinc and molybdenum help promote ALDH activity and restore normal metabolism. Cultivating acetaldehyde metabolising probiotic species like bifidobacterium and reducing acetaldehyde producing species is the long-term goal, however using one of these short-term interventions can be very helpful pre-meal and during die-off:
Some generally helpful intervention options:
Thiamine - the thiazolium/N-heterocyclic carbene of thiamine (or thiamine pyrophosphate (TPP) / cocarboxylase) catalyses self-condensation of two acetaldehyde molecules to acetoin and can then be further reduced to 2,3-butanediol. This process is catalytic, not stoichiometric and needs an alkaline environment. Without sufficient acetaldehyde metabolism support or large doses of thiamine (often grams), expect decreased cellular TPP availability.
Glutathione - creates a nucleophilic attack of the cysteinyl thiol on carbonyl carbon, making S-Hydroxyethyl-glutathione. Creates up to to four adducts per tripeptide and requires adequate glutathione reductase activity to be sustainable. Chronic acetaldehyde / low zinc throttles this route, via low active riboflavin (FAD). Typically dosed at around 250mg.
Kislip - https://ase-onlinestore.com/products-list/asetablet-1box/ (Worldwide shipping, from Japan)
L- Carnosine - can be used at 100mg - 1g, with meals / die-off. (Being explored as a standard inclusion for future updates. Careful, if being used where zinc is still low / methylation otherwise impaired, as excess carnosine is a precursor for histidine and is normally degraded by SAMe-requiring enzymes.)
(USA / Worldwide) - https://www.bulksupplements.com/products/l-carnosine
(AU) - https://aminonutrition.com.au/products/carnosine
(EU) - https://www.amazon.de/dp/B09CH8V6S5
ZBiotics - https://zbiotics.com/products/zbiotics (Perhaps too expensive for daily use)
NAC - small amounts after meals are now included in the DIY Sipper recipe and help remove acetaldehyde.
DHM - now included in Stage 1, though additional amounts can be taken. It promotes ALDH, however this still requires NAD+ and mineral sufficiency.
Binders - Silicon binds acetaldehyde and is included in Stage 1, however you can find a table of binders for multiple purposes in 2.2.3 - Binders.
Methylene Blue - "A lifeguard for the NAD+ pool"
Methylene blue is one of the oldest synthetic medicines still in clinical use. Heinrich Caro first prepared it in 1876 for BASF as a textile dye. Fifteen years later Paul Ehrlich gave it to malaria patients, launching modern chemotherapy, and within another decade anaesthetists were using it to reverse drug-induced methaemoglobinaemia. Over the following century the dye turned up in bacteriology labs, psychiatry wards and, more recently, neurodegeneration trials.
Before implementing anything from this section, it's very important to understand that rapidly correctly a severe NAD+ or chronic acetaldehyde issue can create rapid withdrawal symptoms, mirroring those seen in alcohol and opioid use disorders.
Do not start microdosing methylene blue without first reading and preparing for this withdrawal process. (See "2.3.4 Rapid withdrawal, hypo/hypermetabolism".)
At nanomolar concentrations methylene blue slips into mitochondria and behaves like an auxiliary wire in the electron-transport chain. It accepts electrons from NADH then hands them to cytochrome c, restoring the NAD⁺∶NADH ratio, raising Complex IV activity and trimming reactive-oxygen leakage. In human fibroblasts 100 nM postponed senescence by roughly fifty per cent and boosted ATP production, a finding revisited many times since the original Atamna-Ames work.
Picture the respiratory chain as an electrical harness running across the inner mitochondrial membrane. Normally electrons step down that harness from NADH into Complex I, then through ubiquinone to Complex III, finally jumping onto cytochrome c before sliding into Complex IV and oxygen. When Complex I is inhibited by eg. chronic innate immune response and/or oxidative stress, the first hand-off stalls, the upstream NAD⁺ pool shrinks and everything requiring it as a cofactor idles.
Methylene blue slips in as a short jumper wire bridging the break. In the matrix the oxidised dye (MB⁺) meets an NADH-dependent flavoprotein such as NQO1 or a nonspecific diaphorase. The flavin passes two electrons and a proton to the dye:
NADH + H⁺ + MB⁺ → NAD⁺ + leucomethylene blue (MBH₂)
Leucomethylene blue is colourless, lipophilic and diffuses toward the inter-membrane face where oxidised cytochrome c is waiting. Because the MBH₂/MB⁺ redox pair sits at about +10 mV while the Fe³⁺/Fe²⁺ couple of cytochrome c sits at +260 mV, the electron drop is energetically downhill:
MBH₂ + 2 cytochrome c(Fe³⁺) → MB⁺ + 2 cytochrome c(Fe²⁺) + 2 H⁺
Oxidised methylene blue is now ready to shuttle back for another round; reduced cytochrome c hands its electrons to Complex IV just as if they had come through Complex III. Proton pumping at Complex IV continues, ATP synthase turns, and, crucially, NAD⁺ is regenerated inside the matrix even though Complex I never fired.
At the nanomolar doses used for redox support the cycle is gentle: the flavoprotein step limits the rate, so electrons leak only minimally to oxygen, avoiding significant superoxide. However, increase the concentration into higher single-digit micromolar and our jumper wire becomes a redox treadmill. MB accepts electrons faster than cytochrome c can take them, spills some to molecular oxygen and the extra reactive oxygen species flip the dye from helper to hazard.
(This concentration is also protective against glutamate excitotoxicity.)
In short, the “auxiliary wire” reaction is a two-stroke shuttle: NADH reduces methylene blue, methylene blue reduces cytochrome c, and the dye recycles. It restores the NAD⁺:NADH ratio and keeps oxidative phosphorylation alive without relying on a poorly-performing Complex I. You could consider micro-doses of methylene blue as a Complex I analogue.
However, once plasma levels climb into the low-micromolar bracket the story changes. Around one micromolar plasma concentrations, the dye becomes a potent reversible inhibitor of monoamine-oxidase A; that action has been explored for depression but also explains why high doses can trigger serotonin toxicity if mixed with SSRIs. Push it further, especially with light activation, and methylene blue behaves as a photosensitising antimicrobial, generating singlet oxygen lethal to bacteria and some parasites. At the top of the range, an intravenous bolus of one to two milligrams per kilogram is the standard antidote for life-threatening methaemoglobinaemia because the reduced form, leucomethylene blue, donates electrons directly to ferric haem.
Methylene blue is a lipophilic monocation. As soon as it reaches the bloodstream it starts migrating down every negative membrane potential it can find, the steepest of which is the -150 to -180 mV drop across the inner mitochondrial membrane. One proton motive force equals roughly tenfold enrichment for a monovalent cation per 60 mV, so a healthy mitochondrion will concentrate MB by 100-to 1000-fold, relative to free plasma.
Low-dose pharmacokinetic work in healthy volunteers is uncomplicated and
linear up to about 20 mg. A 1 mg immediate-release capsule yields a
peak plasma concentration (Cmax) of roughly 40 nM
within an hour, and a half-life of five hours for the fast distribution
phase followed by a terminal half-life of fifteen to twenty-four hours.
Scale the dose down and the numbers scale with it. A 0.5 mg dose tops
out at about 20 nM, while a 25 µg “pin-prick” dose peaks at a whisker
under 1 nM. Roughly forty per cent is excreted unchanged in the urine,
which turns a striking blue-green that can dye test strips and,
occasionally, the toilet bowl when used at much higher doses.
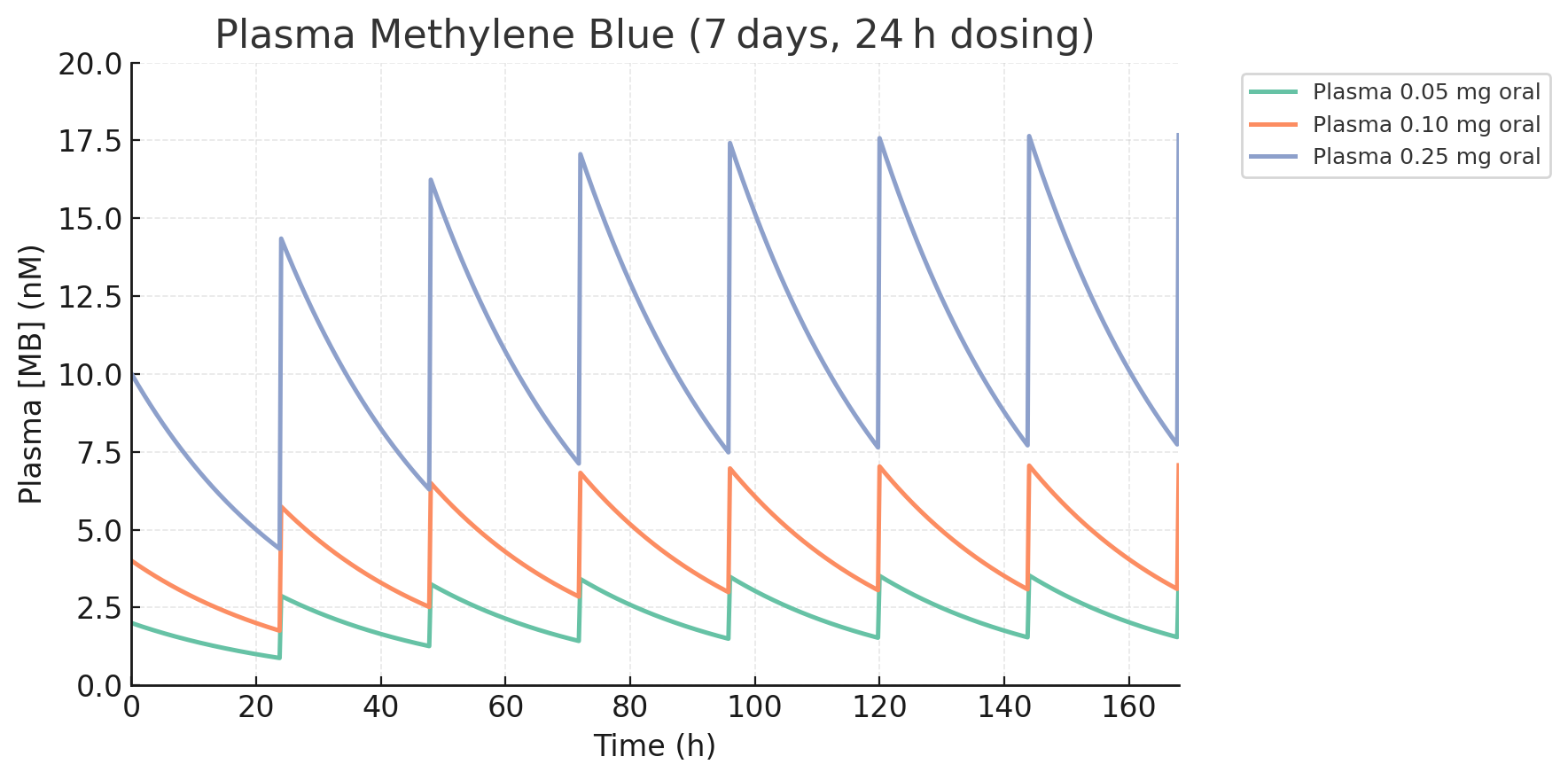
Translate those plasma numbers across the membrane potential and life inside the mitochondrial matrix looks very different. Even with a conservative 100-fold enrichment, for unhealthy
mitochondria, a 0.1 mg dose drives mitochondrial matrix MB to about 0.7
µM. For healthy mitochondria, at the more usual 1 000-fold it hovers
around 7 µM, which is just skirting the threshold where things start
becoming quite unhelpful. At 10 µM, ALDH2 will be inhibited by
approximately 30%.
However, this creates a new challenge, as the
goalposts are going to move once we introduce methylene blue (and
restore active B vitamin metabolites, CoQ10, etc), as the mitochondria
will be expected to shift from an unhealthy to a healthy state. The
concentration of methylene blue inside the mitochondrial matrix may
increase ten-fold. This means the dose will normally need to be
decreased, as mitochondrial health improves. What starts as a
functional 0.1 - 0.25mg oral dose, once per day may decrease to 0.05 -
0.1mg per day, over the first week of introducing it.
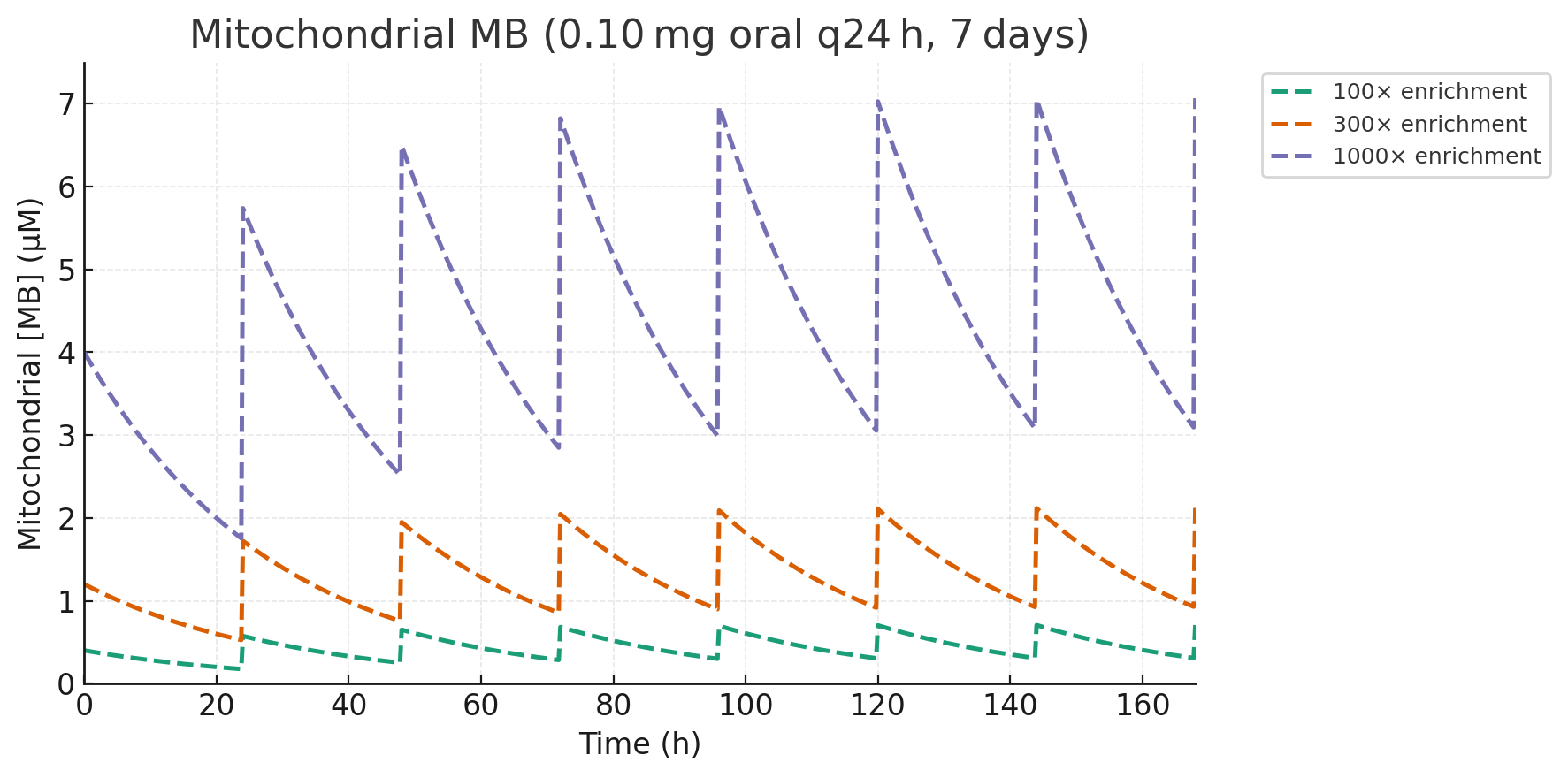
Above 0.25 mg of MB per day, the mitochondrial concentration can become
orders of magnitude above the 100 nM threshold associated with redox
shuttling, glutathione support and mild neuroprotection. As the proton
gradient is preserved, wash-out is slow, giving a useful rule of thumb -
anything that peaks at 10 nM in plasma keeps the mitochondrial concentration above 100 nM for close to one day.
Most adverse effects are concentration-dependent. Sub-milligram doses of MB may sharpen working memory yet rarely colour the urine or stools. At the other end of the scale, taking >20mg+ doses invites strong ALDH inhibition, nausea, AChE inhibition, headache, dizziness and well beyond the threshold for MAO-linked serotonin risk, while glucose-6-phosphate-dehydrogenase deficiency introduces a theoretical chance of haemolysis, though recent malaria trials found that clinically insignificant. There are a range of dose-dependent applications, in between.
When working with MB, spills happen. Fresh stains fade if they are dabbed with three per cent hydrogen peroxide, which reduces the dye to its colourless leuco form. Rinse quickly, because exposure to air re-oxidises the molecule and the blue returns; a second peroxide round usually finishes the job.
Relating to this section of the protocol, for acetaldehyde metabolism and NAD⁺ redox support, methylene blue is best dosed inside a rather narrow window. 0.05 - 0.1 milligram oral doses in water are enough to ferry electrons from NADH to cytochrome c, even when Complex I is inhibited. The 0.1mg per day end of the range is more appropriate for unhealthy mitochondria and 0.05mg is more appropriate as they improve.
NB. Taking methylene blue at this dose range can rapidly remove the NAD+ redox bottleneck. At higher doses it will do the opposite and inhibit ALDH2.
Restoring NAD+ and ALDH activity can quickly restore part of the neurotransmitter degradation pathway, so caution should be taken and expect a mood dip. This should be added only in conjunction with interventions to restore the synthesis pathway in a balanced fashion, or a longer net decrease in neurotransmitters may be experienced - creating energy, sleep and emotional dysregulation, before homeostasis is restored. (see: pre-protocol support)
Using 1% methylene blue (MB), 1 single drop is 0.5mg. This is already 5-10x the target daily dose for most people. We'll need to convert the 1% solution into a 0.1% solution, to make it quick and easy to use.
There are multiple ways to achieve this:
1) Dropper bottle
(More initial setup, maximum convenience)You'll need one of the empty dropper bottles and a larger syringes described in 5 Ordering supplements. The empty dropper bottles listed can hold up to 60mL, however smaller batches may be preferable. In this example, we'll make up a 30mL bottle:
Boil and cool some clean water. Pour some into a glass. We'll only need 27mL of this in a future step.
Using the 1% MB dropper bottle as a source, add 60 drops (3mL, being 10% of the target total solution) into the empty dropper bottle.
Using the syringe, draw up a total of 27mL of boiled and cooled water and squirt it into the same dropper bottle you added the 1% MB to in the previous step.
Screw the cap on the finished bottle and shake it for 10 seconds.
USAGE: 1 drop from your finished bottle now contains 50mcg / 0.05mg and the bottle contains 600 doses. Add desired dose to a glass of water and consume.
2) Water bottle
(Minimal setup, more long-term effort)Adding 1 drop of 1% MB into a (eg. 1L) bottle of water will mean that 1/10th (100mL) of that blue water is now 50mcg / 0.05mg. Any bottle size works, providing you use 1/10th of the total, eg. a 25ml serving is 1/10th of a 250ml bottle.
USAGE: Pour 1/10th of the total solution volume into a glass, per desired 50mcg dose and consume. You can use kitchen scales to measure a serving, where 1g = 1mL of water.
3) Syringe
(Fast, but fiddly - not ideal)As 1 drop = 0.05mL, it could be dropped into an empty glass and drawn up in a 1mL or 10mL syringe. By filling the rest of the syringe with clean water, every 1/10th of the syringe is 50mcg / 0.05mg of MB.
USAGE: Add 1/10th of the syringe content to a glass of water, per 50mcg/ 0.05mg of desired dose and consume.
Some example doses in 250mL of water, to help confirm your product label / dosing accuracy:
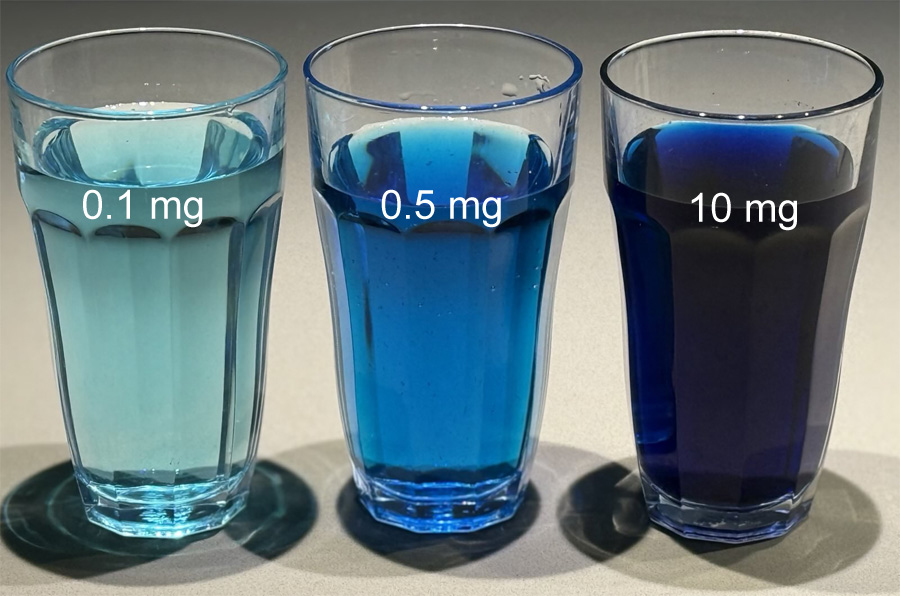
"1% USP Methylene Blue" can be found in 5 Ordering supplements.
By supporting the NAD⁺ pool without consuming it, the dye helps ALDH5A1 clear succinic semialdehyde and keeps ALDH2 from stalling, which in turn eases the brain fog that comes from endogenous GHB and tetrahydropapaveroline. Acetaldehyde and histamine metabolism will see benefits, along with neurotransmitters, energy and other important metabolism.
Successfully deployed, methylene blue may be able to negate a number of interventions supporting metabolism downstream of NAD+ deficiency and ALDH inhibition, depending on mineral status. This may be reflected in future updates.
Again, an important reminder that rapidly correctly a severe NAD+ or chronic acetaldehyde issue can create rapid withdrawal symptoms, mirroring those seen in alcohol and opioid use disorders. It is best to introduce any acetaldehyde scavenging interventions for fermenting "food-in-transit" SLOWLY. Use for Herxheimer-related acetaldehyde spikes is more flexible.
Known limitations:
There is a small subset of people with confirmed acetaldehyde markers, Complex I inhibition and significant unresolved oxidative stress issues which don't respond to microdosing methylene blue at 50mcg, or experience the normally expected endogenous morphine withdrawal symptoms.
The described methylene blue microdose appears to be "used" by the reactive oxygen species (ROS) before providing the described mitochondrial benefits.
This subset of people may also test positive for MetHb and further testing via standard pathology into the location of the ROS could prove very helpful, eg. urinary F2-isoprostanes or s-nitrotyrosine for systemic lipid peroxidation, ADMA ± SDMA (endothelial NO axis), MPO for neutrophil-driven vascular oxidants, and either oxLDL or Lp-PLA2 to see oxidised-lipid activity in the arterial wall.
In this group, a single 5-10mg methylene blue dose is often beneficial for this ROS and MetHb, however is not a long-term solution.
One strategy for this subgroup is to slowly increase the dose by 50mcg each day (starting at 50mcg / day and likely not more than 300mcg / day), until *ANY* change is observed - positive or negative, then holding steady at that dose. Eventually, this dose can be reduced to 50 mcg / day.
One of the biggest challenges for remineralisation with chronic disease and inflammation is absorption. The
disease model shows this is mostly related to elevated TNF-α, IL-1β, IL-6, IL-10, IL-22 -> hepcidin, which then inhibits 2 metal transporters - Divalent Metal Transporter (DMT-1) & ferroportin. This further inhibits dietary intake and circulation of at least 11
metals, by sequestering them in specific cells / tissues (brain, liver, kidneys, spleen).
These known metals are Iron (Fe), Manganese (Mn), Copper (Cu), Zinc (Zn), Cobalt (Co), Molybdenum (Mo), Nickel (Ni), Cadmium (Cd), Lead (Pb), Vanadium (V) and Selenium (Se), in their 2+ state.
This hepcidin-mediated mechanism appears to benefit the host during acute immune activity by depriving circulating pathogens of iron and other minerals which may help their proliferation.
During chronic immune activity (ie. failure to clear the acute infection, due to pathogen evolution and immune surveillance "blind spots" + dysregulation), this hepcidin-mediated cascade leads to depletion of these metals, via dietary blockade during the inflammatory state.
Coupled with this blockade is progressively worse acidaemia from from a lowered lactate threshold, due to progressively worse mitochondrial dysfunction and enhanced renal excretion of zinc and electrolytes. (see Figure 12 on the disease model page and 2.2.4 The importance of pacing)
The more frequent the chronic inflammatory spikes, the more difficult it is to absorb these metals from diet, as they'll be actively rejected. ie. The deeper into the ME/CFS spiral you are, the harder it is to recover the minerals via diet and oral supplementation and the more effort you'll need to put into rebuilding and maintaining their systemic levels.
This means non-oral routes or special tricks to bypass the standard mineral transporters are required for an initial repletion period and progressively less so as the inflammatory cascade is corrected.
According to the literature, a 70kg human body normally maintains an optimal level of many elements needed for enzymatic and other processes.
The amount of each element stored also appears to have a relationship with the severity of the metabolic impact experienced, if deficient, eg. oxygen deficiency creates severe and fairly rapid dysfunction.
Based on the table of elements below, this further suggests that future studies may find overlooked biological advantages in our bodies naturally maintaining a certain amount of eg. lead - perhaps, hypothetically (and purely speculatively) providing resilience against high-energy radiation?
| element | mass | element | mass | element | mass | element | mass |
| Oxygen | 45kg | Gallium | 700mg | Nickel | 15mg | Lanthanum | 800μg |
| Carbon | 13kg | Rubidium | 680mg | Chromium | 14mg | Tellurium | 700μg |
| Hydrogen | 8kg | Strontium | 320mg | Manganese | 12mg | Yttrium | 600μg |
| Nitrogen | 1.8kg | Bromine | 260mg | Arsenic | 7mg | Bismuth | 500μg |
| Calcium | 1kg | Lead | 120mg | Lithium | 7mg | Thallium | 500μg |
| Phosphorus | 780g | Copper | 72mg | Ruthenium | 7mg | Indium | 400μg |
| Potassium | 140g | Aluminium | 60mg | Mercury | 6mg | Gold | 200μg |
| Sulphur | 140g | Cadmium | 50mg | Caesium | 6mg | Scandium | 200μg |
| Sodium | 100g | Cerium | 40mg | Molybdenum | 5mg | Tantalum | 200μg |
| Chlorine | 95g | Barium | 22mg | Germanium | 5mg | Vanadium | 110μg |
| Magnesium | 19g | Tin | 20mg | Cobalt | 4mg | Thorium | 100μg |
| Iron | 4.2g | Iodine | 20mg | Antimony | 2mg | Uranium | 100μg |
| Fluorine | 2.6g | Titanium | 20mg | Silver | 2mg | Samarium | 50μg |
| Zinc | 2.3g | Boron | 18mg | Niobium | 1.5mg | Tungsten | 20μg |
| Silicon | 1g | Selenium | 15mg | Zirconium | 1mg | Beryllium | 36μg |
Standard oral absorption of certain minerals will be inhibited throughout the day, relative to the inflammatory state.
Standard oral absorption is directly inhibited by the inflammatory cascade. The more severe someone's state, the more difficult it is to absorb minerals from food and oral supplements. For this reason, the protocol specifies certain non-oral mineral supplements as a "MUST", along with various coenzymes.
Inflammation created downstream of the hypoxia / mitochondrial dysfunction -> lactic acidaemia cascade appears to be one of the most significant inhibitors of the remineralisation process. Failure to prevent acidaemia is expected to stall any efforts, regardless of the administration route. (see "2.3.3 Blood-flow, hypoxia and fibrin-amyloid" and the Acidaemia subsection of "2.2.4 The importance of pacing")
Combined with difficulties in absorption, various metabolic alterations will be causing enhanced excretion of electrolytes, and endotoxins (acetaldehyde, gliotxin, etc) can cause deficiency of silicon and zinc. Relative to the disease model, these can have significantly deleterious effects on energy metabolism, immune function and barrier function.
https://www.atsjournals.org/doi/10.1164/rccm.201301-0061OC
https://journals.physiology.org/doi/full/10.1152/ajpgi.00350.2009
Intravenous, intramuscular, subcutaneous, sublingual, rectal and transdermal routes bypass this mineral transporter blockade in the duodenum.
Dissolving nutrients in Dimethyl sulfoxide (DMSO) is another effective strategy to bypass inhibited transporters and downstream metabolism, systemically. DMSO has such an interesting regulatory history that I've written a stand-alone review article, just to cover it all.
Specially compounded vitamins and minerals which bypass this inflammatory cascade are now available internationally from an Australian pharmacy, in the form of sublingual troches and a DMSO "transdermal" solution, which can also (and preferentially) be safely used orally, in regions where that is permitted.
Please see the “4.2 Compounded nutrients” section on how to order these products.
Magnesium spray is another example of a transdermal supplement. Dead Sea
mud is another very rich transdermal source for a number of minerals and
electrolytes, eg. calcium, magnesium, bromine and silicon. However,
while reportedly highly successful at helping resolve these
deficiencies, it's also a little cumbersome and time inefficient to use.
An alternate source of bromine (and iodine) is kelp, now found in the
protocol's DIY powder schedule.
Depending on the skin microbiome,
a rash or biofilm may develop. This can be prevented by pre-rinsing and cleaning the
skin with a NAC-based solution (e.g. 5g NAC in 250mL of water) when
showering and washing the area with a cloth. Be sure to thoroughly clean
and dry your skin, especially the areas where transdermal supplements
are being used.
Iodine / iodide uptake into cells via sodium-iodide symporter (NIS) requires active Vitamin A sufficiency (all-trans retinoic acid). (See also Figure 8)
Notes and cautions:
1) Intravenous and intramuscular administration of minerals and other nutrients may be offered by local IV nutrients clinics or your doctor. Unfortunately, without these are normally not customised around your data and doses used may be closer to those commonly found in total parenteral nutrition. These are not appropriate for resolving moderate-to-severe deficiencies.
2) IV iron / ferritin administration is well-known for causing a high rate of hypophosphatemia. The disease model suggests this is largely due to an effect which is very, very similar to "refeeding syndrome". As such, IV iron and other minerals would likely have a significantly reduced risk of triggering this state, if the dietary electrolytes, vitamins and other micronutrients are being well-managed. Stage 1 of the protocol targets these variables and would be recommended as a precursor to any IV iron infusions. This can be discussed further with your doctor.
https://pmc.ncbi.nlm.nih.gov/articles/PMC8279965/
The body is actively blocking iron absorption to benefit the host during an infection. Due to the deficiencies, we are taking a necessary step in bypassing this safety mechanism to achieve mineral repletion. Cobalt and Vitamin D sufficiency can help maintain these levels.
However, once iron repletion has been achieved, there is also logic in reducing / removing iron supplementation, especially during any acute immune activity and where eg. Lyme infections, etc have been detected. Ongoing monitoring via standard blood test markers - Iron, Transferrin, Transferrin Saturation% and Ferritin - is strongly recommended.
3) The safety profile of any "nano" mineral compounds is not well-established and the data on a number of them is already concerning. I would avoid being exposed to these materials at this time.
4) In the interests of harm minimisation, I am also aware of reports that
some people have been self-administering non-prescription injectable
mineral products used in agriculture and veterinary applications out of desperation and/or frustration with the medical system, as a
way to rapidly alter their mineral status. Some of these products have seriously inappropriate ratios
and concentrations of minerals for use in humans and could cause harm.
eg. Yes, it's true that veterinary products, such as "Multimin Evolution Injection for Cattle" sold in Australia provides (elemental) zinc
@ 30mg, copper @ 7.5mg, manganese @ 5mg and selenium @ 2.5mg, per 0.5mL
subcutaneous dose. While you may consider that hypothetically, 3-4 x 0.5mL doses over 1-2 weeks
may help provide a rapid resolution for a deficiency of those minerals (apart from zinc - which has a much larger 2g+ total store in human tissues), I would strongly encourage people not to take shortcuts like these. These products are not made for humans. They're unlikely to be produced with any consideration around pH, osmolality and/or compound concentration. They may have undisclosed ingredients in the product formulations. There is a high probability of these products creating tissue damage and serious post-injection pain.
Please seek competent medical supervision / management and use registered / approved products only.
Understanding Reduced Blood Flow in Chronic Disease: Impact on Quality of Life and Symptoms
Reduced blood flow, or impaired circulation, is a common issue in many chronic diseases. It can significantly affect a person's quality of life by exacerbating symptoms, slowing healing processes, and increasing the risk of complications. Understanding the factors that influence blood flow is essential for both medical professionals and patients managing chronic conditions. Addressing these influences not only alleviates symptoms
but also enhances overall well-being and disease outcomes.
Infections in the Bloodstream
Bacteremia, fungemia, and septicemia refer to the presence of bacteria, fungi, and toxins in the bloodstream, respectively. These infections can lead to systemic inflammation, causing blood vessels to constrict and reducing blood flow. In chronic disease patients, compromised immune systems make them more susceptible to these infections, which can worsen their condition and delay recovery.
Oxidative Stress and Vascular Health
Oxidative stress occurs when there's an imbalance between free radicals and antioxidants in the body, which is a significant factor in this disease model and relates to dysregulation of IFN-γ. Excessive free radicals can damage the lining of blood vessels, leading to stiffness and reduced elasticity. This damage impedes proper blood flow and can contribute to the progression of chronic diseases like diabetes and hypertension. Additional dietary antioxidant can assist during elevated immune activity.
The Role of Zeta Potential and pH
Zeta potential is a measure of the electrical charge on particles, such as red blood cells, in a fluid. A healthy zeta potential keeps cells evenly dispersed, promoting smooth blood flow. Changes in blood pH can alter zeta potential, causing cells to clump together and slow circulation. Maintaining a balanced pH is crucial for optimal blood viscosity and flow.
Nitric Oxide Synthase and Vasodilation
Nitric oxide synthase is an enzyme responsible for producing nitric oxide, a molecule that relaxes blood vessels and improves circulation. In chronic diseases, the production of nitric oxide can be impaired by oxidative stress and mineral deficiencies, etc., leading to vessel constriction and reduced blood flow. Enhancing nitric oxide levels can help alleviate symptoms by promoting vasodilation.
Spike Protein, Fibrin, Fibrinogen, and Amyloid Aggregates
Fibrin and fibrinogen are proteins involved in blood clotting. In chronic conditions, elevated levels can lead to excessive clot formation, obstructing blood vessels. Additionally, fibrin-amyloid aggregates can accumulate, further hindering circulation. Spike protein has been found accumulating in various tissues, suggesting it has difficulties being degraded. Monitoring and managing these various protein levels are vital to prevent blockages and maintain healthy blood flow. NAC, nattokinase and DMSO may assist in degrading aggregates, along with biofilms and spike protein. A recent paper suggested a single human-equivalent oral dose of 25g nattokinase could clear fibrin-amyloid microclots. Toxicology data for nattokinase shows no observable adverse events even at 1000mg/kg in rats suggesting a similarly higher safety profile in humans, however further studies are needed. Aspirin and various prescription anticoagulants are also known to be helpful in managing symptoms in chronic disease.
Neutrophil Extracellular Traps (NETs)
Neutrophils are white blood cells that release extracellular traps to capture pathogens. However, excessive formation of these traps can increase blood viscosity and contribute to clot formation. In chronic diseases with persistent inflammation, NETs can play a role in reducing blood flow and exacerbating symptoms.
Sodium Levels and Blood Volume
Sodium insufficiency can lead to decreased blood volume, known as hypovolemia. Sodium helps retain water in the bloodstream, maintaining adequate blood pressure and flow. Low sodium levels can cause dehydration, reducing blood volume and impairing circulation. Ensuring sufficient sodium intake is important for patients unless contraindicated by their condition. (see "4.1 Electrolytes")
Dehydration and Hypovolemia
Dehydration reduces the total volume of blood in the body, leading to hypovolemia. This condition decreases the amount of blood available to transport oxygen and nutrients, negatively affecting organ function and energy levels. Staying hydrated is essential to support adequate blood flow and overall health. Impaired glycogen homeostasis and downstream electrolyte losses during windows of severe insufficiency can be drivers for hypovolemia.
Structural Influences on Circulation
Structural issues like chronic cranial instability can compress blood vessels, impeding blood flow to critical areas like the brain. This can be exacerbated when laying down, where your pillow height is inappropriate. Similarly, blocked lymphatic vessels hinder the removal of waste products and excess fluids, leading to swelling and increased pressure on blood vessels. Addressing these structural problems can significantly improve circulation and symptom management. (see "2.2.5 Structural issues")
Sleep breathing disorders from metabolic disturbances in nasopharyngeal, oral, lung and/or related tissues from localised endotoxemia / biofilms can significantly influence hypoxia and sleep quality. These may require remediation. (see "2.2.3 Living without chronic dysbiosis")
How to identify chronic hypoxia / acidaemia markers?
(Lactic) acidemia is commonly seen with (chronic infection -> immune activity -> coagulation ->) hypoxia:
a. Low phosphorus in Oligoscan or OAT data can indicate parathyroid issues, acetaldehyde and/or (metabolic/respiratory or renal) acidemia.
b. Elevated oxalate markers and/or relative elevation of lactic acid vs pyruvic acid in the OAT results are indicators for hypoxia.
c. Elevated lactate dehydrogenase (LDH) isoenzymes in blood tests can indicate hypoxia in one or more tissues.
d. Out-of-range d-dimer, APTT, INR and other blood-flow markers can indicate a higher risk for hypoxia.
If chronic hypoxia / acidaemia is present, additional support may be required:
1. Sodium bicarbonate in water, away from meals, is already included in the DIY Sipper recipe and
can be helpful in “patching” downstream issues of acidemia.
2. A combination of 300mg aspirin, >1g of NAC and 12000-16000FU (or more) nattokinase (eg. Neprinol) has been shown to effectively target multiple upstream causes of hypoxia in many people. A smaller number of people may require higher doses. This combination has similar effects to "triple therapy", with additional benefits against biofilms, oxidative stress and various toxins. (NB. Daidzin and daidzein are soy isoflavones which inhibit ALDH2 in a similar way to disulfiram. Some nattokinase products like ARG Nattokinase NSK-SD may contain residual daidzin and should be avoided.)
Notes and Limitations:
1. Correcting hypoxia is expected to help remove innate immune bias towards IFN-alpha response and assist IFN-gamma activity. Initial immune activity increase and die-off symptoms could be expected when starting these two interventions, if hypoxia issues are present. Therefore a "negative reaction", at first, is a good general indicator for hypoxia being appropriately addressed. The pre-protocol support items would be highly recommended during this time.
2. Failure to address hypoxia will stall remineralisation and microbiome remediation. If there is any doubt in the accuracy of your data, the default position is to include these interventions and monitor for a reaction.
https://www.ncbi.nlm.nih.gov/books/NBK513346/
Much like in alcohol dependence, individuals with SIBO may experience metabolic impairments due to the fermentation of sugars into alcohol and acetaldehyde within the gut. This process can disrupt homeostasis, precisely mimicking the metabolic challenges faced by chronic alcohol users.
When treating alcoholism, the typical approach involves gradually reducing alcohol intake, supported by high doses of thiamine (Vitamin B1) and large amounts of Vitamin C. In addition, psychological counseling is often recommended as part of the recovery process
https://pmc.ncbi.nlm.nih.gov/articles/PMC8302359/
In some cases, doctors may prescribe Naltrexone, a medication that can help regulate dopamine and GABA metabolism, offering relief from alcohol cravings. Naltrexone has additional benefits beyond this primary use, such as improving mood and reducing anxiety - however there are some additional benefits.
https://pmc.ncbi.nlm.nih.gov/articles/PMC2565602/
What has not been fully understood or appreciated is that alcohol -> acetaldehyde elevation further elevates endogenous synthesis of morphine, codeine and gamma-hydroxybutyrate (GHB), as can severe and chronic Complex I inhibition. Both acetaldehyde and Complex I inhibition are commonly observed in collected ME/CFS data.
For endogenous morphine and codeine synthesis, the mechanism is related to dopamine metabolism. When ALDH1A1 and/or ALDH2 are inhibited, elevated dopamine and DOPAL cause an elevation of Tetrahydropapaveroline (THP) (also known as (S)-norlaudanosoline), which is the first step in the morphine biosynthesis pathway. This altered metabolism leads to behavioural changes that overlap ADHD, coupled with homeostasis alterations and dependence .
https://onlinelibrary.wiley.com/doi/10.1111/j.1755-5949.2009.00114.x
https://www.pnas.org/doi/10.1073/pnas.050324410
https://www.science.org/doi/10.1126/science.557839
THP has also been observed in Alzheimer's and Parkinson's disease patients, however the model suggests it will be found in numerous others. Morphine and DHMA has been observed in collected data by younger members of the Born Free community, without any exogenous use.
https://www.mdpi.com/1420-3049/28/5/2166
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3560700/
https://pubmed.ncbi.nlm.nih.gov/1545408/
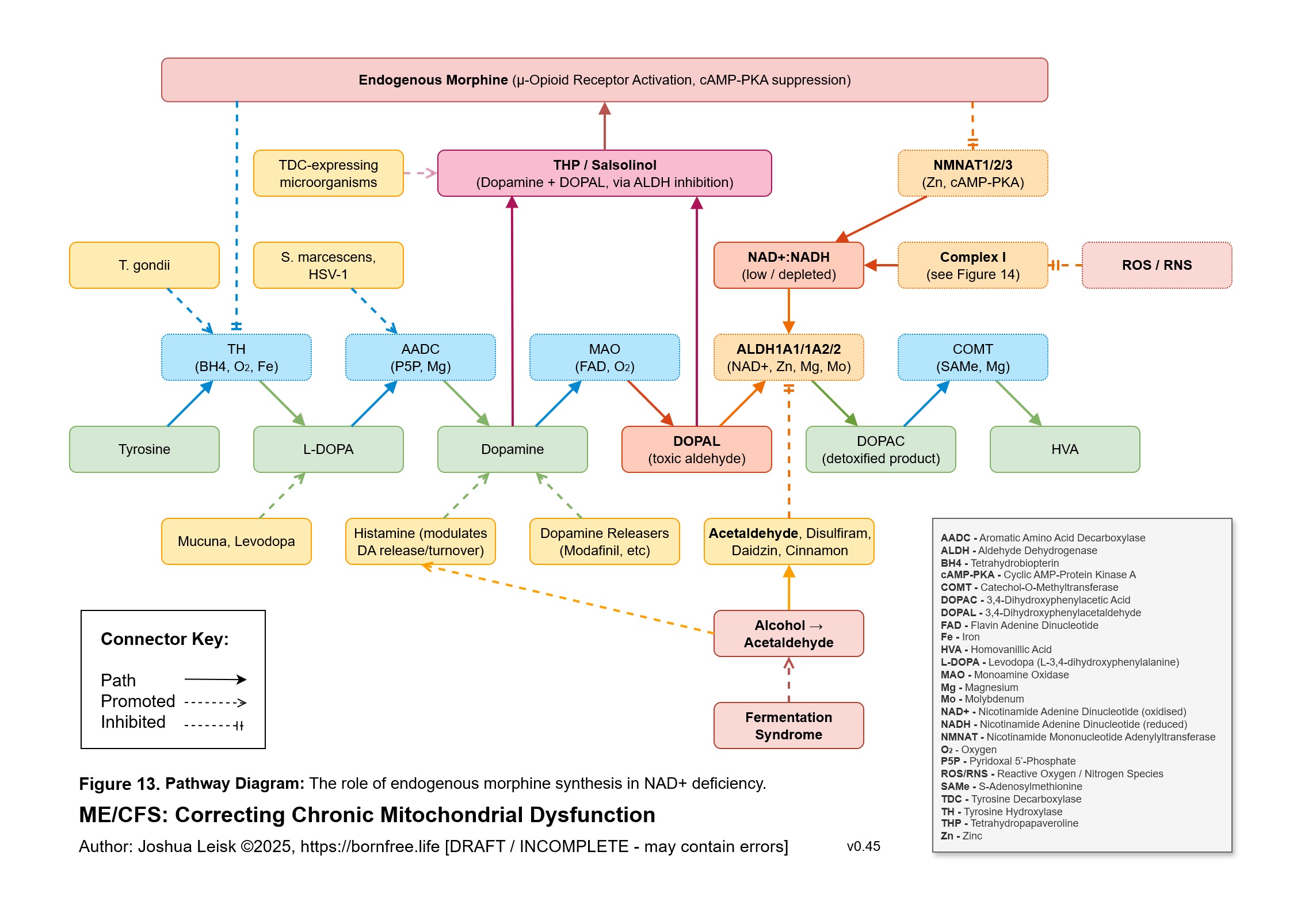
Naltrexone, particularly in its low-dose form (LDN), is a well-known therapeutic intervention for managing opioid use disorder. It is also increasingly used to treat conditions such as Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS), Long COVID, and Post-Vaccine Syndrome. The disease model suggests additional mechanisms for its observed therapeutic benefits.
https://pubmed.ncbi.nlm.nih.gov/38267326/
The body’s production of gamma-hydroxybutyrate (GHB) is linked to changes in GABA metabolism through a process connected to the GABA shunt. In this pathway, GABA is normally converted into succinic acid via an intermediate called succinic semialdehyde (SSAL). However, when the enzyme ALDH5A1 is inhibited, often due to low NAD+ levels, while NADPH levels are elevated, SSAL is instead metabolized into GHB.
https://www.ncbi.nlm.nih.gov/books/NBK1195/
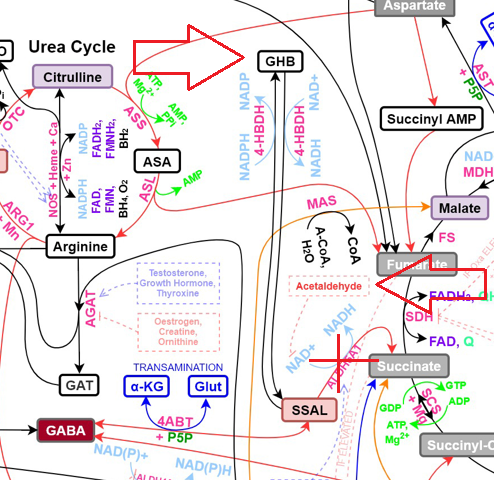
GHB is marker #75 on the OAT results and is often quite elevated in more severe patients:

As we gain a better understanding of how the gut microbiome interacts with these metabolic processes, it becomes crucial to anticipate potential withdrawal symptoms during microbiome remodelling. A rapid improvement in gut health, especially after a significant dietary shift or use of antimicrobials and/or biofilm breakers, can lead to sudden withdrawal from multiple endogenous narcotics. This is expected when introducing low-dose methylene blue in Stage 1 and also during Stage 2 of the protocol, where removing acetaldehyde producing species is the primary focus.
The more rapidly any successful gut fermentation syndrome remediation is performed, the more likely that someone will go into rapid withdrawal symptoms for multiple simultaneous narcotics. Microdosing methylene blue to provide alternative Complex I functions and restore NAD+ redox is a reliable trigger.
For instance, transitioning to a ketogenic diet or using antimicrobials can trigger an initial wave of endotoxaemia (toxins released from dying bacteria), which may temporarily suppress withdrawal symptoms. However, as microbial production of alcohol and its byproduct acetaldehyde decreases, there is a corresponding reduction in the synthesis of morphine and GHB. This may result in metabolism and symptoms expected during chronic alcohol, opioid, and GHB withdrawal, which can peak about a week after significant microbiome changes.
Depending on the significance of the alcohol / endogenous narcotic reduction, symptoms may include any of:
Insomnia, Low Liver Glycogen - Nausea and Vomiting, Sweating, (severe) Fatigue, Hypothermia (low body temperature), Diarrhea, Abdominal Cramping, Hypometabolism, Tremors, Tachycardia (rapid heartbeat), Muscle Aches/Cramps, Seizures, Hypertension (high blood pressure), Anxiety, Agitation, Panic, Terror, Reduced Motivation, Difficulty Concentrating, Hallucinations, Delirium/Confusion, Depressed Mood, Psychosis, Yawning, Goosebumps (piloerection), Runny Nose (rhinorrhea), Lacrimation (tearing), Dilated Pupils, Internal Vibrations, "Band Around Head" Pressure (warning, this is an indication for severe withdrawal, ahead of seizures).
The symptoms are largely relating to cAMP-PKA-CREB homeostasis, can be potentially life-threatening / self-harm inducing and are expected to appear and disappear multiple times over typically 2-3 weeks, like a swinging pendulum over-shooting, on its way back to the center, where homeostasis is restored (see Figure 18 on the disease model page for additional information).
With each swing, one direction has a "drugged" feeling (low cAMP-PKA tone) and the other direction includes panic, depression, elevated heart-rate, insomnia, etc. (elevated cAMP-PKA tone). Hormonal status greatly controls this pathway and for females, it would be distinctly advantageous to start any endogenous opioid withdrawal process just after menses. Oestradiol amplifies excessive cAMP signalling and progesterone calms it. During excessive cAMP signalling, any adrenergic triggers will be amplified - small signals can easily become panic, terror and spiralling. This may also explain why women suffer from neuropsychiatric symptoms manifest at different stages of their menstrual cycle (pre-ovulation and luteal phase) and why they are more likely to suffer when this pathway loses homeostasis than men, generally. More understanding and empathy around this could help inform appropriate patient care.
As this process usually accompanies restored NAD+ pool status, being the primary currency and sensor for cortisol's regulation of innate immune activity (XO, and NOS, NOX - via further NAD+ conversion to NADPH), it's expected that any tissue with an active infection or tissue repair functions orchestrated by IFN-gamma activity will flare with inflammation and pain. This can feed into adrenergic signalling to promote cAMP.
Both of these processes can be "cushioned" and managed to make them tolerable.
Ironically, the logical solution is fairly simple, although it may understandably raise some initial concerns.
It has often been said that "alcohol is the cause of and solution to all of life's problems" and never more literally than in this instance.
This observation has been shared by various well-known people with ME/CFS and related online groups such as https://www.reddit.com/r/hangovereffect/.
Although this author's opinion is bound to attract some criticism, I'd also advocate that using exogenous alcohol, as an over-the-counter tapering schedule against withdrawal from the microbial-sourced alcohol (and the 2 downstream endogenous psychoactive substances) is a far simpler and less problematic therapeutic intervention than administering exogenous opioids and/or benzodiazepines, in an attempt to create an effective tapering schedule.
These 2 classes of drugs are both well-known to be "drugs of dependence" and will likely require high doses to be effective symptomatically. High doses of these interventions can create a long tapering schedule of their own that may last 6 months to a year and is known to be highly unpleasant.
Following a strict alcohol tapering schedule and avoiding dosing at levels which induce alcoholic intoxication is required. The goal is to remain in a tolerable level of withdrawal symptoms during the taper, rather than attempting to make the process "feel pleasurable" and extending the process. This will be highly personalised and likely involve multiple doses over the day / night, which decrease over time. Having appropriate monitoring and management would be highly advisable.
Caveats and Risks
1) It would be optimal to avoid alcohol reaching the gut microbiome.
Neat alcohol such as gin, vodka or whiskey, when taken in small sips
and absorbed largely via the mucous membranes found in the mouth, throat
and oesophagus would be a preferred route of administration. These can be attempted at 1/2 a "typical" drink, eg. 15ml of neat spirits, or 1/2 a beer / wine / cider, etc. and allow 20-30 minutes to test if stability / relief has been achieved.
2) While alcohol add-back therapy is known to be problematic in chronic alcohol use withdrawal due to the risk of behavioral disorders, such issues are less likely to arise in conditions like ME/CFS or Long COVID where alcohol consumption was not voluntary or habitual. However, professional oversight and adequate peer support is still recommended to manage the process effectively and provide a safety-net.
Cinnamon contains compounds which also inhibit ALDH and can provide some tapering support for a few hours per dose. Effective dosing ranges may span from 1/10th to 1 teaspoon of cinnamon powder.
NB. Excess amounts of cinnamon can trigger a "drugged" or "drunk" feeling.
In addition to alcohol tapering, certain supplements may also help manage withdrawal symptoms relating to hyper-metabolism / panic / depression / insomnia during rebound excess cAMP signalling.
These include:
1. Tiny doses of bacopa, eg. 25-50mg active bacosides to modulate CREB and without spiking cAMP. NB. Higher doses flip the other way and exacerbate symptoms.
2. Lithium sufficiency to inhibit GSK-3beta and promote CREB.
3. Low doses of progesterone, eg. 10-50mg, to calm cAMP and promote CREB.
4. Progesterone > oestradiol balance modulators, like chasteberry.
5. Ivabradine, low dose propranolol, etc.
6. 0.5-1.5g of L-theanine, multiple times per day, to antagonise glutamate signalling.
7. Carbohydrates, uridine monophosphate. phosphate and magnesium sufficiency to promote glycogen synthesis and help negate cAMP spikes -> PEM, POTS, etc.
Other influences:
1. Insulin spikes lower cAMP (perhaps explaining "stress-eating").
2. Post-orgasmic period lowers catecholamines, reducing adrenergic signalling (perhaps explaining part of the ADHD "hypersexual" behaviour as a soothing / stress-regulating mechanism).
Various foods, drugs and supplements that promote beta-adrenergic signalling, or cAMP, or inhibit PDE will significantly exacerbate any rebound excess cAMP symptoms and should be avoided / managed appropriately during the "adrenergic excess and insomnia" side of the "pendulum swing".
These include:
1. Forskolin (cAMP promoter).
2. Yohimbe / yohimbine, rauwolscine (indirect cAMP promoters).
3. Caffeine (cAMP promoter).
4. Hesperidin and some formulations of other citrus bioflavonoids like quercetin (PDE inhibitor).
5. Luteolin (PDE inhibitor).
6. Boswellia (cAMP promoter, PDE inhibitor).
7. Cialis, viagra and related drugs (PDE inhibitors).
8. SNRIs and/or exogenous cortisone dosing may need reduction.
NB. While removing methylated B9 and B12 *can* "pull the fuse" on SAMe synthesis (needed for PNMT and epinephrine levels), this also affects a wide array of other important enzymes and leads to decline, histamine sensitivity, etc. This is not advisable except as an emergency and temporary measure.
Some effects of chronic opioid use will take many months to fully recover. Many of the related studies were conducted on heroin users and may not reflect the prognosis for someone actively supporting mineral status and other variables.
Overall, the withdrawal process is unpleasant, but manageable with the right tools and is essential to recovery.
When the elements reported by your Oligoscan are optimal, a 3+ day “water fast” may provide additional benefits. This is not advisable with severe mineral deficiencies.
If this is your first water fast, it is generally advisable to have someone monitoring you during this time. Avoid driving vehicles, stress and excessive exertion.
Fasting protocol requirements (per day):
- No food or other supplements
- 3L water
- 5g (teaspoon) of sodium chloride (5g table salt contains 2.5g elemental sodium)
- 3g NAC (mucolytic, oxidative stress)
- 1000mg magnesium oxide (will induce diarrhoea)
Optional add-ons:
- EGCG 500mg, 3× per day
- Resveratrol 120mg, 3× per day
- Hesperidin 500mg, 2× per day
- “Upper GI biofilm flush, bind and purge recipe” (see: "2.2.3 -- Biofilm breakers"), the night before starting day 1 only.
Important safety consideration:
To break a water fast “early”, use two or more apple cider vinegar doses – without capsules – as a succinate source. This is only a requirement if EGCG has been dosed in the previous 6 hours and ketogenesis is poor. Failure to observe this safety consideration may result in rapid cyclical blackouts and convulsions until the EGCG is fully metabolised or until someone else administers apple cider vinegar. This could easily be fatal, for example if operating a motor vehicle. You have been warned.
After successfully remineralising and remediating dysbiosis sufficiently enough to enjoy a normal quality of life, you may be inclined to adopt lifestyle changes and dietary strategies to prevent sliding back down the slippery slope to poor health:
Real food, lots of coloured vegetables and diversity. Eat the right ballpark targets for carbohydrates, fats and proteins. You can use an app such as https://cronometer.com to help structure your diet and learn what micro and macronutrients are in each food until it becomes second nature.
Now that your dietary absorption is working, your micronutrients should be coming from food, rather than supplements. The protocol’s diet is still a good foundation, however you won’t need to be mindful of avoiding excessive oxalates, vitamin B6, histamine or vitamin A.
Vitamin D3 is a good supplement to maintain.
Maintenance supplement
Here are 3 product examples for very similar daily shakes with "lite" versions of the protocol ingredients, albeit in forms which aren't suitable for someone in a moderate / severe state . These could be highly appropriate as a maintenance / preventative strategy, alongside busy lifestyles and imperfect diets.
The first two products contain 75+ ingredients. Huel Daily Greens has 91 ingredients and may be a superior product (does not ship to Canada).
Athletic Greens 1 (AG1) - https://drinkag1.com/ [There have been some recent AG-1 concerns circulating on social media and this is being investigated.]
Nuzest "Good Green Vitality" - https://www.nuzest.com.au/products/good-green-vitality
Huel "Daily Greens" - https://huel.com/products/huel-daily-greens
One of the main macronutrient differences between Good Green Vitality, Daily Greens and AG1 has additional pea protein "for digestive comfort" and costs a little more.
Your hormone synthesis, methylation and immune activity are promoted by physical exertion. This benefits your energy metabolism, sleep, neurotransmitters and helps prevent disease. Posture rehabilitation and maintenance is also important.
Eat foods which degrade biofilms, such as;
Herbs and spices like turmeric and black cumin, which contain tannins, phenolics, flavonoids, aromatics, etc. Sugar replacements such as xylitol and stevia. Mushrooms, especially reishi.You can perform a periodic biofilm disruption / challenge interval – e.g. a large oral dose of eg. tetrasodium EDTA or robusta coffee (ethyl acetate) once every 2–4 weeks and a similar interval for nasal / sinus and other microbiomes, using a relevant tool where necessary. Ocean swimming can be helpful. Yearly water fasting intervals would be advantageous. Occasional "robusta coffee enemas" are also rather useful for biofilm maintenance in the large intestine.
Checking your mineral status every 3–6 months is a good way to see how your diet is performing and make corrections. It can also be used to infer your levels of inflammation and potentially dysbiosis, which could justify further testing, e.g. OAT / microbiome.
It is generally expected that many intracellular deficiencies for eg. silicon, magnesium, iodine, selenium, molybdenum, copper, zinc and others may show in your CMA and / or Oligoscan data (and that functional deficiencies for iron, manganese, copper and six others may exist in any (deprecated) HTMA data, indicating inflammation severity over time.)
Assuming inflammation and pH imbalances are correctly managed, resolving these deficiencies may take, eg.
2 or more months, via non-oral routes, eg. sublingual / transdermal / rectal, providing acidaemia and renal dumping has been resolved.
1 - 2 weeks via appropriately dosed parenteral administration, providing acidaemia and renal dumping has been resolved. This can then be easily maintained via non-oral routes.
NB. These deficiencies are likely not going to resolve at all using standard oral dosing, due to mineral transport inhibition in the duodenum.
If your Oligoscan and/or OAT data shows low phosphorus, the upstream causes for this need to be addressed as a priority, or else remineralisation will be highly problematic. Common upstream influences include the various issues affecting mitochondrial metabolism, to the point of triggering lactic acid metabolism (anaerobic glycolysis). Some of these include insufficient pacing, zinc status, oxidative stress support and oxygen transport / coagulation.
If you are using the compounded nutrients, a number of these minerals
and various vitamins are combined using a sublingual or DMSO-enhanced route, which greatly simplifies this part of the protocol. The
default formulation should suffice for most
people, unless your transferrin saturation is at or above 35-40%, in which
case you would reduce the ferritin content to zero. Where the transferrin saturation exceeds 45%, ie. "iron overload", checking for and remediating cobalt deficiency is suggested, along with excluding any causes of methemoglobinemia. (see “4.2 Compounded nutrients” section)
Please recheck your CMA / Oligoscan for progress on remineralisation regularly (and HTMA, as desired, for progress on inflammation, strontium and rubidium). Adjust mineral supplements as needed if remineralisation is slow. There appears to be a bell curve response for absorption of many metals, where around 5-10% of the total system stores is the upper limit, per day and further efforts result in active blockade. Similarly, absorbing a reasonable amount of excess minerals is not normally problematic unless you have, for example, Wilson’s disease, hemochromatosis or beta thalassemia. These diseases are rare, however need careful management.
Where an element is indicated as non-optimal, you can use these suggested (elemental) minimum daily doses below, relative to the interpreted lower threshold.
Based on our collected data, we interpret Oligoscan / SO/Check reports using different upper and lower thresholds than the provider’s report layout indicates.
For Oligoscan reports, VISUALLY, the "Low" threshold is relocated to halfway between the original Low and OK vertical lines, (ie. where the “a” in “Normal” is located, to the left of “OK”) and the "High" for all markers except fluorine is relocated to halfway between OK and original High vertical lines (ie. where the “o” in “Normal+” is located, to the right of “OK”).
Numerically, if you wanted to do this computationally, Oligoscan "Low" and "High" threshold values for each marker would be recalculated as:
Low=(((Low+High)/2)+Low)/2
High=(((Low+High)/2)+High)/2
NB. According to the 2024 Oligoscan practitioner's guide*, due to an unusual quirk in methodology / reporting, highly elevated minerals (to the right of our vertical blue line / upper threshold in the image below and usually indicated as yellow or red bar) need to be re-interpreted as highly deficient. This also applied to SO-Check reports. If you see this anomaly in your data, it would be advisable to confirm this by taking a CMA test, if possible. Otherwise, default to reinterpreting the marker as proportionally "low".
*The practitioner's guide discusses zinc transport blockade as the reason for the marker elevation. From our comparisons with CMA data, the issue also applies to other markers and appears to be something do to with the "trade secret" Oligoscan algorithm. Ultimately, I think this could be improved.
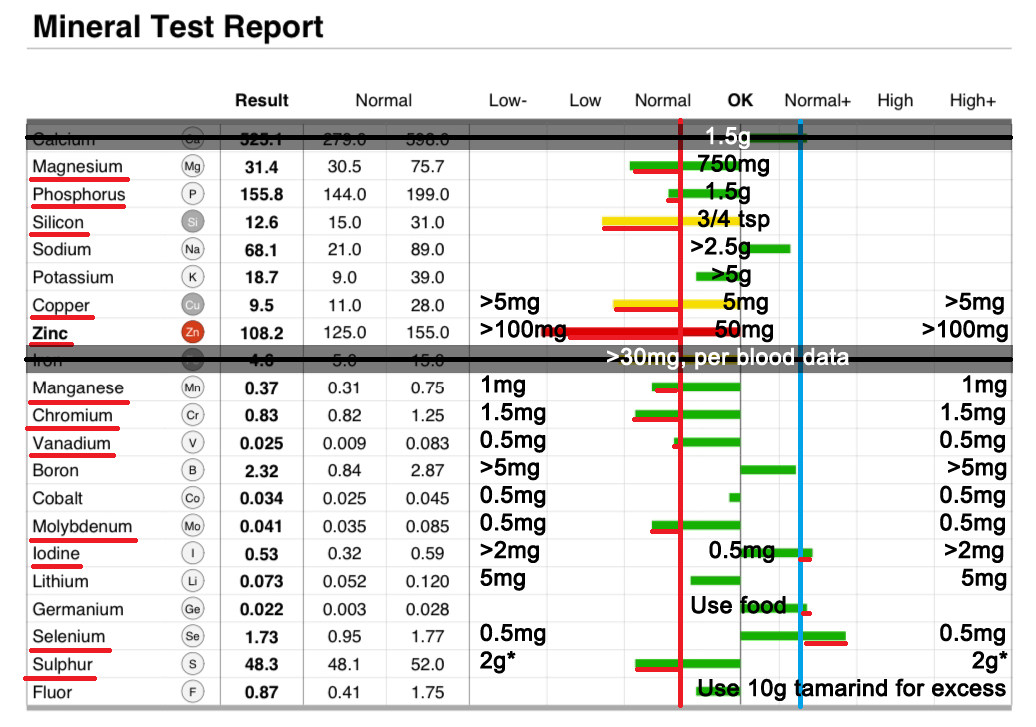
For So/Check branded reports, these have a different format / layout and markers are shown as a percentage deviation from “normal” instead of values. You can ignore this report’s two outer columns to use the dosing guide image above.
1. The same methodology "quirk" relating to elevated values in Oligoscan applies to So/Check, as do the higher sensitivity thresholds for interpretation.
2. So/Check Calcium and Iron are discarded / ignored for the same reason as Oligoscan.
3. So/Check Copper and Zinc markers may also be over-stated.
4. Numerically, the So/Check mineral and electrolyte markers have a reinterpreted lower in-range threshold of -14% and an upper in-range threshold of +14%, instead of +/-25%.
Marker values which are INSIDE the +/- 14% threshold are interpreted normally as progressively lower or higher than the ideal target, which is 0%, ie. "in-range, low" and "in-range, high".
Marker values which are OUTSIDE of these +/- 14% thresholds in either direction are both interpreted as "LOW" and are considered progressively worse on a scale, the further the value deviates from 0%, OUTSIDE of the new thresholds. For example, +/- 30% would be "VERY LOW", +/- 50% would be "CRITICALLY LOW".
5. In-range low markers should still be supported by diet and/or supplementation.
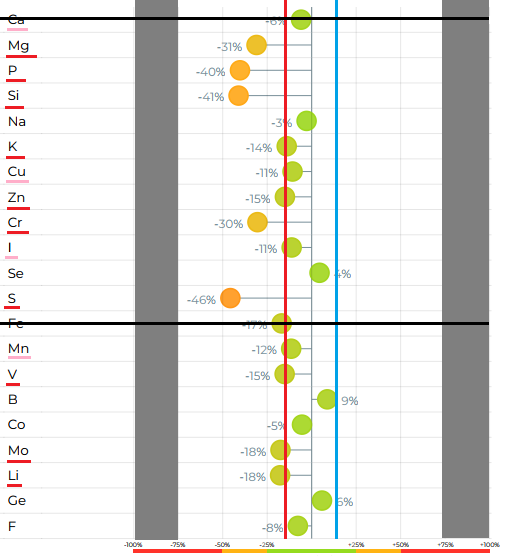
Although no longer used in this protocol, elevations of electrolyte excretion in hair tests can indicate low cellular uptake with dietary sufficiency, causing enhanced excretion. Where a hair mineral profile shows low potassium and similarly low rubidium, the rubidium deficiency will need correcting or else potassium levels may be difficult to restore. Similarly, calcium with strontium and magnesium with lithium. High zinc can indicate low histidine / insufficient protein.
An important note on hypoxia and acidosis:
Low phosphorus in Oligoscan or OAT data can indicate parathyroid issues,
acetaldehyde and/or (metabolic/respiratory or renal) acidemia.
(Lactic) acidemia is commonly seen with (chronic infection -> immune activity -> coagulation ->) hypoxia.
Elevated oxalate and/or relative elevation of lactic acid vs pyruvic acid in the OAT results are further indication for hypoxia.
If chronic hypoxia is present, additional support may well be required. (see: "2.3.3 Blood-flow, hypoxia and fibrin-amyloid")
NB. Correcting hypoxia is expected to help remove innate immune bias towards IFN-alpha response and assist IFN-gamma activity. Initial elevated immune response, fatigue and die-off symptoms could be expected when starting these interventions. Pre-protocol support items may be useful in supporting this period.
Failure to address hypoxia / acidemia will stall remineralisation and microbiome remediation. (see: "2.3.2 Remineralisation")
Low sulfur in Oligoscan or So/Check data can indicate elevated transsulfuration, sulfur metabolising microorganisms or microbial oxalate issues.
Low iodine is often observed with fluorine excess. Fluorine is found in medicines, toothpaste and town water. Consuming 10g of tamarind paste per day can dramatically increase excretion of fluorine.
If you have taken a blood test for iron, transferrin, transferrin saturation% and ferritin and the transferrin saturation% is below 18%, you have a critical need for iron supplementation before Stage 3. However most oral supplements will not absorb and can feed pathogens.
For other supplement selection criteria:
Earlier / manual guidance:
“Do I need P5P?”


38, 39, 40, 75 – where no SSRI, melatonin or 5-HTP supplement is being used, if these markers are all in the lower range, this can infer low P5P levels, via (38) aromatic L-amino decarboxylase (AADC) [+ P5P] ⇒ monoamine oxidase (MAO) [+ riboflavin as FAD], via (39) kynureninase (KYNU) [+ P5P, less oxidative stress] and via (40) kynurenine aminotransferase (KAT) [+ P5P / zinc / magnesium], via (75) as 4-aminobutyrate transaminase (4ABT) [+ P5P] ⇒ SSAL [+ NADPH] -> GHB}. Part of this pattern assumes dietary tryptophan is sufficient.

51 – Pyridoxic acid / pyridoxate is a degradation metabolite of B6 / pyridoxal, which can be used to infer pyridoxal LESS any aldehyde dehydrogenase (ALDH) activity [NAD+ / magnesium / zinc deficiency, acetaldehyde], pyridoxine 5'-phosphate oxidase (PNPO) activity [riboflavin as FMN, tissue damage / TGF-b1 inhibition, hypoxia] and aldehyde oxidase (AO) activity [riboflavin as FAD, molybdenum, heme, iron+sulphur, hypoxia].
“Do I need biotin?”

57 – Methylcitric is used to indicate biotin availability. If this marker is out-of-range in either direction, sublingual biotin will need to be carefully used.
“Do I need trimethylglycine (TMG) / betaine?”
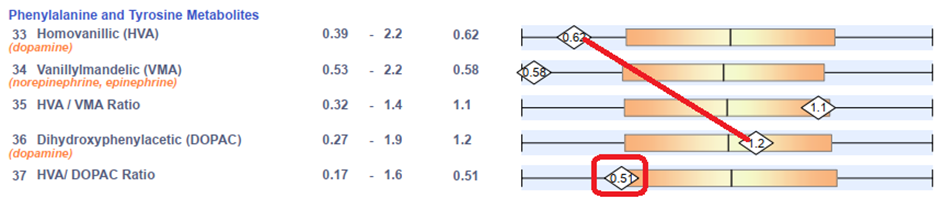
37 (36:33) – The lower the integer in 37, the more likely you are to benefit from some methylation support. 3,4-dihydroxyphenylacetic acid (DOPAC) ⇒ homovanillic acid (HVA) involves 1 enzymatic reaction – catechol O-methyltransferase (COMT), which requires S-adenosylmethionine (SAMe) as a cofactor. SAMe is produced by the methylation cycle. These markers can be confounded by overgrowth of certain bacteria and by renal synthesis of dopamine.

41:42 – This ratio can also help interpret methylation status. An unbalanced ratio of uracil:thymine can indicate low activity at thymidylate synthase OR low pentose phosphate pathway activity - > PRPP, R1P, R5P affecting uridine pyrophosphorylase, along with NAD+ synthesis, purine synthesis, glycogen synthesis, etc.. If uracil is also low, this could further indicate dietary protein insufficiency.
“Do I need Vitamin B5”

52 – This marker can help indicate a vitamin B5 deficiency, which will affect lipolysis and pathways reliant on coenzyme-A (many). Elevated 16 / HPHPA may also benefit from more B5 to produce CoA. If in doubt, include B5 - it's not known to have tolerance issues, although if you're deficient it can be stimulating at first until the pathways rebalance.
“Does my OAT and Oligoscan / CMA data correlate?”
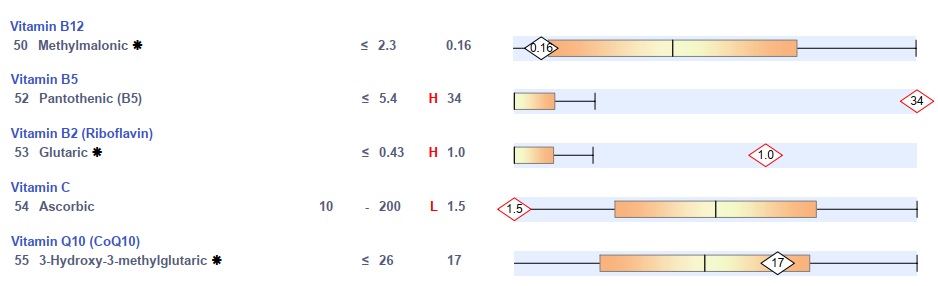
50 - Vitamin B12
52 - Vitamin B5 / pantothenic acid
53 - Vitamin B2 / riboflavin
54 - Vitamin C / Ascorbic acid
55 - CoQ10

76 – Either elevated or low (excreted) urine phosphoric acid should correlate well with a LOW (intracellular) Oligoscan phosphorus marker. If they do not, please share your data and report this in our Discord discussion group for further analysis.
Maintaining electrolytes can be challenging, due to expected renal dysfunction in this disease model. If you are suffering from any pre-existing kidney disease consult your doctor prior to supplementing any of these elements.
Maintaining your electrolytes is arguably one of the most critical goals for your daily micronutrient intake, relative to your quality of life. According to the intracellular data collected and disease modelling, these are highly problematic in many chronic diseases, yet poorly captured by standard serum testing.
Serum levels of electrolytes are tightly regulated and often fail to help indicate intracellular or systemic levels until your status reaches a level where an emergency hospital visit is required.
Electrolytes include potassium, sodium, calcium, magnesium, phosphate, chloride and bicarbonate. Electrolytes are required for ion channels / transporters, signalling pathways, blood pressure regulation any many important metabolic pathways. Electrolytes and minerals are required building blocks for ATP, GTP, UTP, TPP, FAD, NAD+, NADP, P5P, CoA, glycogen, pyruvate and many other important currencies, cofactors and metabolites.
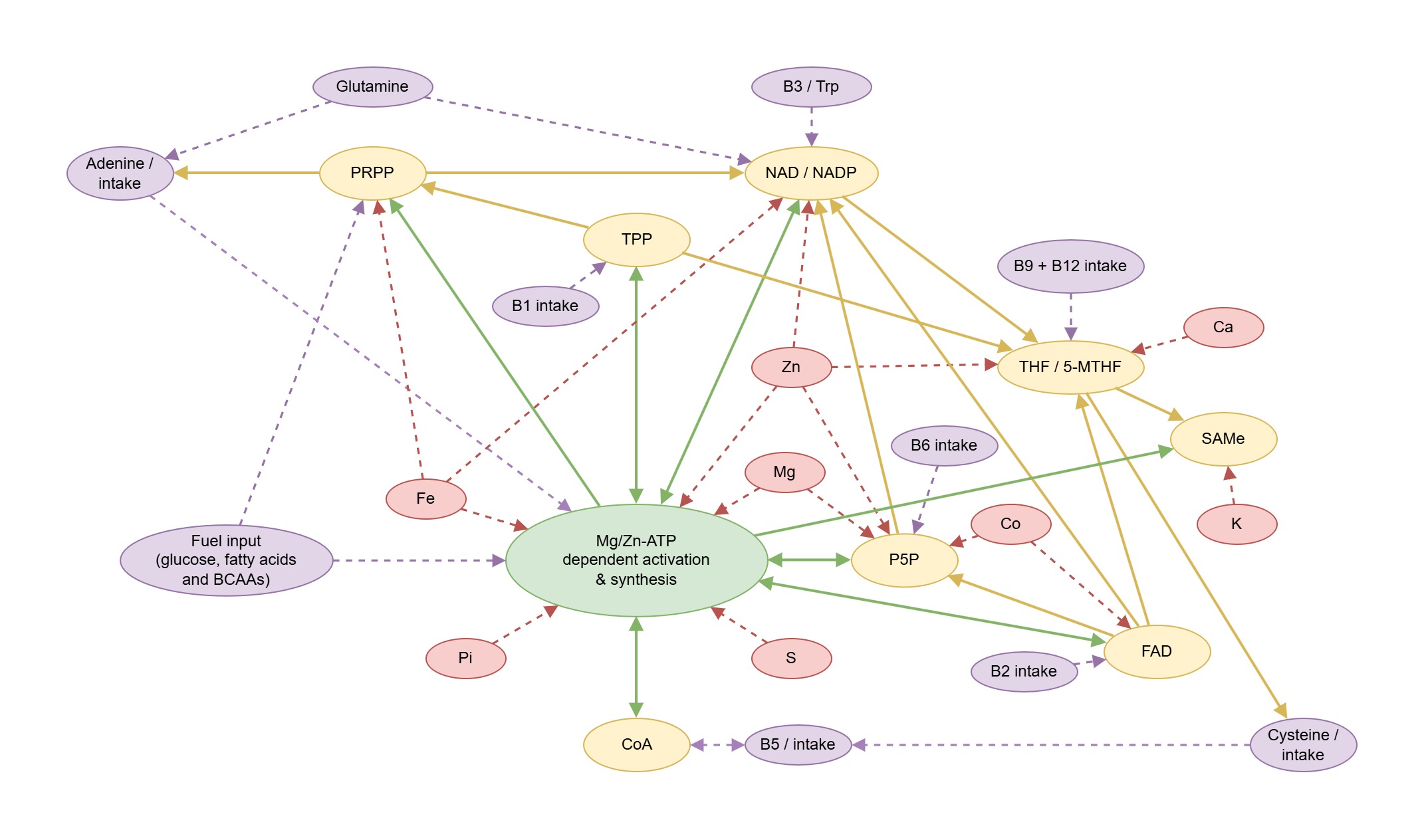
When electrolytes are deficient, neurological symptoms, fatigue, muscle spasms and pain/inflammation may occur (skeletal, smooth and cardiac tissues). Digestion and nutrient absorption may be impaired. Low electrolytes and especially low phosphate and/or magnesium, where caused by acidosis, can inhibit mineral repletion efforts.
Electrolytes can “exchange” at the cellular membrane as pairs by pumps called "ATPases", which consume approximately 2/3 of ATP produced inside the cell, to maintain functional levels of each electrolyte inside and outside the cells.
For example:
The Na+K+-ATPase exchanges sodium : potassium.
The Ca2+-Mg2+-ATPase exchanges calcium : magnesium.
Under extreme metabolic conditions, alternate exchangers, such as the Na+/Ca2+ exchanger (NCX) can exchange sodium : calcium, too.
This is not an exhaustive list.
For this reason, a deficiency of one electrolyte in the pair can create
issues absorbing and retaining the other, creating a secondary
deficiency. Ideally, deficiencies for electrolytes should be addressed as pairs, or all at once, to prevent exacerbating an existing imbalance.
Intracellular deficiencies for each electrolyte can come from various influences other than simple dietary deficiency of it and / or its "exchanging partner", eg.
Calcium deficiency can also be created by parathyroid hormone (PTH) issues downstream of eg. low iron and phosphate. Other influences include elevated oxalate synthesis, low Vitamin D, low Vitamin K2 mk7 and excessive NCX activity.
Common symptoms include low energy, low neurotransmitter synthesis, sleep disturbances, muscle tremors and osteopenia.
Magnesium deficiency can also be created by silicon deficiency and chronic diarrhoea.
Common symptoms include low energy, low neurotransmitter synthesis, sleep disturbances, muscle tremors and constipation.
Sodium deficiency can also be created by chronically elevated IFN-gamma and CYP2D6 enzyme activity in the kidneys, which produces renal dopamine and promotes renal sodium excretion. Other influences include frequent diarrhoea, vomiting or sweating. Above daily values of sodium intake are required during periods of immune activity.
Common symptoms include low energy, dizziness, nausea, muscle tremors and low blood pressure.
Potassium deficiency can be created by chronic alcohol / acetaldehyde, chronic kidney disease / infection, diabetic ketoacidosis, frequent diarrhoea, vomiting or sweating, folate deficiency, chronic elevation of aldosterone.
Common symptoms include low energy, low neurotransmitter synthesis, muscle tremors and high blood pressure.
Phosphate deficiency can also be created by chronic alcohol / acetaldehyde elevation and also acidemia, triggering renal excretion of phosphorus. This can come from metabolic or respiratory acidemia / acidosis. Elevated lactic acid + low intracellular zinc is one mechanism which can allow elevated lactic acid from an energy crisis, mineral deficiencies or hypoxia to progress to acidemia / acidosis. Low phosphate (and other electrolytes) can create broad metabolic impairments, which can spiral and lead to lowered baseline / lactate threshold.
Common symptoms include low energy, muscle tremors / poor strength, seizures, rhabdomyolysis, respiratory suppression, softening of bones and teeth.
Bicarbonate deficiency can also be created by metabolic acidosis, chronic diarrhoea, elevated oxalate levels and chronic kidney disease / infection.
Common symptoms can include tachycardia, confusion and fatigue.
Chloride deficiency has not been commonly observed.
Most electrolytes should be consumed slowly over the day. They may cause diarrhoea and other symptoms in large doses. Magnesium studies showed elevated excretion and only 10% retention from larger oral doses.
https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC1855626/
Transdermal administration has been demonstrated as a superior route for magnesium absorption due to the "slow-release" aspect. Rapid absorption and downstream elevation of serum electrolytes triggers rapid excretion to restore homeostasis, resulting in poor electrolyte retention and wasted effort. This can be exacerbated by low activity levels and intracellular deficiency of the corresponding partner in the electrolyte pair.
Electrolytes are commonly available as salts, and the second table below outlines the relative amounts of each electrolyte in these salts.
The weekly DIY "sipper/shot" recipe contains suggested amounts based on poor dietary intakes from food sources and can be adjusted where necessary. A link to an electrolyte calculator can be found at the bottom of this section.
People with a history of anxiety and / or neuropsychiatric symptoms may be sensitive to calcium and potassium repletion and need to onboard them more slowly. Monosodium phosphate can be used as an alternative phosphate source during this time at eg. >5g / day, after ramping up.
Starting magnesium and/or phosphate can improve glucose uptake and glycogen synthesis. Experiencing symptoms that resemble hypoglycaemic events or diabetic "hangry" mood alterations may indicate more dietary carbohydrates are needed.
TOTAL daily (elemental) targets from all food / supplement sources
| Element | Target Daily Amount | Notes and Sources |
| Sodium Na | >4g | (Daily value is 2300mg. More is required than normal, due to elevated excretion rate from glycogen depletion and innate immune activity cascade.) 5g (1 teaspoon) of table salt contains 1.95g Na. |
| Potassium K | >5g | (Daily value is 4700mg.) 10g of Nu-Salt (potassium chloride) contains 5g of K. 3 large potatoes (900g) contains roughly 5g of K. |
| Magnesium Mg | >500mg | Supplemental regimen should include transdermal route, where deficient. |
| Calcium Ca | >750mg | Increase supplementation to 1.5–2g if deficient. Cronometer can help visualise your calcium intake. CMA results show intracellular calcium deficiencies. Low phosphorus and also low strontium in hair testing may also infer calcium status. Oxalate dumping can be expected initially with repletion. |
| Phosphate Pi | >1g | Meat, dairy, pumpkin seeds / pumpkin seed oil, red lentils, sunflower seeds, potatoes. Supplement if deficient. Supplements which combine phosphorus with various electrolytes, e.g. calcium phosphate, may be available in some regions. Much higher intakes may be required in severely depleted states. |
| Bicarbonate HCO3 | As needed | Commonly found in sodium bicarbonate / baking soda (NOT baking powder)
and/or potassium bicarbonate. A typical dose is 1/4 teaspoon, AWAY FROM
MEALS, multiple times per day - if lactic acid / oxalic acid is elevated
and/or phosphorus is either high OR low in OAT results, or phosphorus /
sulphur is low in Oligoscan. |
Reference material: Elemental weights, by compound, for calculating servings of various electrolytes
| Electrolyte Compound | % Weight Proportions | Example Weight Proportions |
| Sodium Chloride NaCl | Na 39%, Cl 61% | 6.4g contains 2.5g sodium & 3.9g chloride |
| Potassium Chloride KCl | K 52%, Cl 48% | 9.6g contains 5g potassium & 4.6g chloride |
| Magnesium Chloride MgCl2 | Mg 26%, Cl 74% | 2g contains 520mg magnesium 1.48g chloride |
| Sodium Bicarbonate NaHCO3 | Na 27%, HCO3 73% | 5g contains 1.4g sodium & 3.6g bicarbonate |
| Potassium Bicarbonate KHCO3 | K 39%, HCO3 61% | 12g contains 4.7g potassium & 7.3g bicarbonate |
| Calcium Citrate C12H10Ca3O14 | Ca 24% | 4g contains 960mg calcium & 3g citrate |
| Potassium Citrate C6H5K3O7 | K 38% | 13g contains 4.9g potassium & 8.1g citrate |
| Monosodium Phosphate NaH2PO4 | Na 19%, P 26% | 6.6g contains 1.25g sodium & 1.7g phosphorus |
| Disodium Phosphate Na2HPO4 | Na 32%, P 22% | 7.7g contains 2.5g sodium & 1.7g phosphorus |
| Monopotassium Phosphate KH2PO4 | K 29%, P 23% | 7.5g contains 2.2g potassium & 1.7g phosphorus |
| Dipotassium Phosphate K2HPO4 | K 45%, P 18% | 10g contains 4.5g potassium & 1.8g phosphorus |
| Monocalcium Phosphate CaH4P2O8 | Ca 17%, P 26% | 5g contains 0.9g calcium & 1.3g phosphorus |
| Dicalcium Phosphate CaHPO4 | Ca 29%, P 23% | 3.8g contains 1.1g calcium & 870mg phosphorus |
| Magnesium Aspartate C8H12MgN2O8 | Mg 8% | 6g contains 500mg magnesium 5.5g aspartate |
An electrolyte calculator tool can be found here - https://bornfree.life/learn/electrolyte-calculator/
Compounded nutrients which bypass the inflammatory cascade are available from an Australian compounding pharmacy. These are available in three forms and can be customised to suit various requirements.
1. Custom compounded DMSO liquid formulation.
This is the most convenient and bioavailable form, which rather strangely must be sold and labelled "for transdermal use only" in many countries, even though oral use is logically less likely to allow environmental toxins to be carried through skin into the circulation, as people aren't normally putting eg. household cleaners into their mouths.
The regulatory stance - which is already misaligned with the decades of evidence for safety and toxicity - appears to fall short here, also.
If I was personally using any type of DMSO liquid nutrient product, rather than messily applying it to my skin, I'd be rather inclined to squirt a dose into the back of my throat using a syringe (no needle) and then swallow it - allowing oesophageal absorption, roughly 40 minutes after a meal and 15 minutes before any further food / drink.
NB. DMSO can trigger some short-lived, localised histamine responses,
especially when applied to skin in higher concentrations and where that may expose hidden pathogens to immune surveillance. This is much
less likely in mucosal tissues.
DMSO also solidifies at 18C, which means it should be stored somewhere at room temperature. Unfortunately, this is in conflict with the best practices and advice given when dispensing in Australia. The glass bottle can be gently warmed in a pot of hot water, from a tap, for 5-10 minutes. It should always be vigorously shaken before use.
2. Capsules without DMSO
These are also available for regions where import restrictions may be complicated, or where people may want to empty the capsules into their own eg. 10-50% DMSO+water-based solution.
The liquid portion can be prepared ahead of time by taking,
eg.
an empty 480mL amber glass bottle;
and mixing (using your kitchen scales and a syringe - 1mL water = 1g)
1) 50mL of pharmaceutical grade DMSO
2) 400mL of clean water (adding water to DMSO will generate some initial heat)
3) 1.5mL (30 drops) of peppermint essential oil and
4) 28mL (1 oz) of vanilla butternut or vanilla oil
This recipe would provide around 60 days of the liquid portion, if used at 4mL per each AM/PM dose. A 5mL syringe and a shot glass will be very helpful.
The ratio of DMSO:water (+ flavouring) can be adjusted between 10% to 50% DMSO, as desired.
For best results, the AM or PM capsules should be emptied into your DMSO, water and flavour solution just before use.
NB. DMSO can trigger some short-lived, localised histamine
responses,
especially when applied to skin in higher concentrations and where that
may expose hidden pathogens to immune surveillance. This is much
less likely in mucosal tissues.
3. Troches
The original sublingual troche formulations are also still available as a "multinutrient" (minus zinc) and a separate standalone zinc troche.
To order any of these research-only products, they are now available through a new website:
https://healthdispensary.au/product-category/born-free-protocol-certified/
For initial repletion, you may leave all “targets” at default values, unless your pathology data shows sufficient or excess iron levels, eg.
For a transferrin saturation above 30%, with ferritin and iron above the middle range, you can remove iron.
If transferrin saturation is >40%, also remove iron and review / remediate cobalt status, if deficient. Test/exclude/remediate methemeglobinaemia.
NB. LITHIUM CANNOT BE INCLUDED IN THESE FORMULATIONS DUE TO AN AUSTRALIAN LEGISLATIVE MISMATCH VERSUS DIETARY GUIDELINES. (Prescription only, unless <0.01%). Lithium will therefore need to be purchased and consumed separately. Oral absorption works. Cobalt and silicon are not yet included and will also need to be purchased separately.
Once mineral repletion has been confirmed in follow-up mineral testing, the dosing may be reduced to maintenance intake levels, which may be eg. 25-50% of the standard formulation.
The Good State Ionic Man product used in Stage 3 may also be sufficient for ongoing maintenance, if coupled with sufficient B vitamins, NADH, biotin, brazil nuts, etc.
Note and limitations
1. If someone experiences mouth ulcers / lesions / sores with sublingual troche use, pause for a few days and address the oral microbiome using eg. bacteriophages, antiseptic recipe, etc and follow with oral probiotics from 2.2.3 Living without chronic dysbiosis.
2. These products contain highly bioavailable nutrients which allow rapid changes to energy, neurotransmitter and immune-related metabolism, where severe deficiencies exist. This can be unnecessarily unpleasant at the beginning. Starting at eg. 1/8th (or even 1/16th) of a dose, per day may help smoothen the transition. Also see the gentle onboarding process in the Getting started section.
3. Troches aren't overly palatable and are available to use as a suppository, if desired. It is suggested to avoid peppermint flavouring if this is your intended administration route, as it can trigger bowel movements. Troche 1 now has "vanilla butternut" flavouring, which is much more tolerable for either application.
4. Sublingual ferrous fumarate may cause a black / brown hairy tongue at times, if you have inflammation.
5. Ferrous fumarate may cause a false positive for occult blood on a GI test.
6. The ferrous fumarate and riboflavin will stain biofilms / plaques orange and/or brown. These can be dissolved by using a NAC + sodium bicarbonate rinse before brushing. See the 'gentle' DIY antiseptic recipe in 2.2.3 Living without chronic dysbiosis.
For convenience, weekly batches of powder can now be prepared ahead of time to simplify dosing and improve time management. You can still adjust / modify your weekly batches around any individual dosing requirements.
The weekly DIY preparation task is best created as 2 separate weekly recipes -
a. DIY "shake" - a supplements shake, consumed 3 times per day.
b. DIY "sipper" - an electrolyte + amino acid "sipper", consumed slowly across the day, in between meals. (Shake bottle before each use, as dicalcium phosphate is insoluble).
The tables below indicate the amount of powder to be added (or capsules to be opened) and thoroughly mixed together in a suitable kitchen mixer / grinder, such as the ones used for making sauces and Indian meal preparation. Ideally this device should have a stainless steel jar, support dry materials and have at least 1.5L capacity, eg. Philips HL7759/00, Philips HL7756/00, Thermomix, etc.(see "5 Ordering products" or search Google / Amazon / eBay for "indian mixer grinder" and double-check that any imported overseas models match your power plug / input voltage, eg. AU/EU 220-240V, US 110V)
In the absence of a suitable mixer, the destination tub itself can be
filled and shaken vigorously / used as a manual dry mixer (if your
energy allows or someone can assist).

Empty 1.5L or larger tubs / buckets are needed to store the finished powders. (see "5 Ordering products")
For the DIY shake: To calculate your serving size, divide the total net weight of your finished weekly powder by 21 to reach a single serving, taken 3x/day.
For example, 615g net / 21 servings = 29.3g per serving. Large kitchen scales will be required. (see "5 Ordering products")
The DIY shake is taken 3 times per day, 15–30 minutes before meals, replacing the existing schedule for those supplements, even those which may have been previous dosed only once per day.1
In Stage 2 and 3, there are items such as NAC and Spirulina which are present in Stage 1, yet have increased doses. These differences are shown in the table.
If you are just starting out, you can still prepare a full week of powder, start with smaller servings, e.g. ¼ the normal dose and increase the serving size over time to reach a full dose.
a. DIY "shake" recipe (weekly preparation)
| Product Name | Stage 1 | Stage 2 | Stage 3 | Notes | |
|---|---|---|---|---|---|
| 2 | B8 Myo & D-Chiro Inositol | 3 caps | 3 caps | 3 caps | For AU source, 1.5g = 3 caps. DE source has 20% more per cap. |
| 3 | B5 Pantothenic Acid | 0.7-3.5g | 0.7-3.5g | 0.7-3.5g | |
| 4 | Candex | 21 caps | 21 caps | 21 caps | |
| 5 | PQQ+CoQ10 | 7 - 21 caps | 7 - 21 caps | 7 - 21 caps | |
| 6 | Apigenin | 7 - 56 caps | 7 - 56 caps | 7 - 56 caps | |
| 8 | Psyllium husk | 35g | 35g | 35g | |
| 9 | Kelp | 7g | 7g | 7g | |
| 13 | Lecithin | 77g | 77g | 77g | |
| 19 | Trimethylglycine | 3.5g | 3.5g | 3.5g | Only needed if indicated by OAT |
| 20 | L-Lysine | 14g | 14g | 14g | |
| 21 | L-Proline | 14g | 14g | 14g | |
| 22 | L-Glycine | 35g | 35g | 35g | |
| 23 | L-Serine | 14g | 14g | 14g | |
| 25 | L-Glutamine | 35g | 35g | 35g | |
| 26 | Bamboo (Silica) | 14g | 14g | 14g | |
| 27 | Green Tea (EGCG) | 1.75-3.5g | 1.75-3.5g | 1.75-3.5g | |
| 28 | R-ALA | 4.2g | 4.2g | 4.2g | |
| 30 | Spirulina | 3.5g | 3.5-35g | 3.5-35g | Slowly increase in Stage 2 |
| 31 | a-GPC | none | 3.5g | 3.5g | Pause if it creates a headache. |
| 32 | Schisandra | none | 8.3g | 8.3g | |
| 33 | Elderberry | none | 3.5g | 3.5g | |
| 34 | Apple Cider Vinegar (ACV) | none | none | 16.8g | |
| 35 | Beta-glucans | none | none | 1.75g | |
| 38 | Dihydromyricetin (DHM) | 10.5g | 10.5g | 10.5g | |
| 48 | C Ascorbate | 14g | 14g | 14g | |
| 50 | Curcumin | 7 caps | 7 caps | 7 caps | |
| 71 | Colostrum | none | 28g | 28g | |
| 112 | GI-Synergy (K-64) | none | 7 sachets | 7 sachets | 1 sachet / day. Start slowly / separately, can cause potent die-off. |
| 129 | Resveratrol | 1.5-10.5g | 10.5g | 10.5g | If substituting - note differences between trans-resveratrol and resveratrol (use trans-resveratrol at 50% dose). |
b. DIY "sipper / shot" recipe (weekly preparation)
This can be combined with eg. green or other tea, lemon juice, acai, cranberry, etc to modify the flavour of your tart "seawater-tasting" concoction and
then put into a 500mL drink bottle to be slowly consumed over the day, eg.50mL / hour,
ideally in-between meals - preferably 1 hour either side. (Shake 500mL bottle before each use.)Each 50mL serving can also be poured into a glass and topped up with another 200mL water to significantly improve palatability and form part of your recommended 2.5L daily water intake.
[If you find any particularly enjoyable combinations, please feel free to share them with the group!]
Individual electrolytes in the DIY sipper recipe can be reduced by amounts already obtained from food items, using your food logging results (see 2.1.4 Cronometer). This is relative to meeting or even somewhat exceeding the daily targets set in "4.1 Electrolytes".
For the DIY sipper:
NB.The amounts listed below for monocalcium phosphate @ >35g, potassium citrate @ 91g, etc are the amounts needed for a week (>4g and 13g, etc. per day, respectively).
To calculate your daily serving size:
1) Divide the total net weight of your finished batch of weekly powder, eg. 479.5g, by 7 to reach a single daily serving, eg. 68.5g.
2) Then, for each day, approximately 68.5g of the batch is dissolved in 500mL of water, with any flavour enhancements and sipped over the day (OR poured into a glass and topped up with 200mL water) at eg. 50ml per hour, between meals and ideally 1 hour away from them.
NB. Additional phosphate and magnesium can be required / helpful in severe depletion. Additional bicarbonate can also be helpful with severe phosphate deficiency and upstream acidosis. Consuming too much of any electrolyte at once may cause diarrhoea, headaches, nausea, water retention and/or rapid urination.
While the Oligoscan provides instant data, it will typically take 1–3 weeks to get other results (CMA, OAT, microbiomes, etc.) and a potentially similar timeframe to order / receive supplements from vendors. For time efficiency, consider ordering any/all supplements which do not require personalisation while you are still collecting your data.
Some products are not available domestically in all regions and will need to be imported from USA. As such, the order list is based around two primary USA suppliers, however some alternative local vendors / supplements for some regions have been provided where possible.
Apologies, this table is too large for mobile devices and is best viewed on a computer, where it can also be exported as a spreadsheet to aid product ordering accuracy.
The default table selection shown is for US (and international) orders. You can select a different region (eg. EU, AU) to see a merged list of US + region-specific products, where available. You can sort the table by columns. Sorting by 'Product Vendor Link', will group products by vendor.
Notes:
1. Quantities in grams or bottle counts are indicated for a 90 day supply. The products will be sold in amounts or multiples matching or somewhat exceeding 90 days.
2. Products rows in purple (where the "Custom" field is "1") are already included in the "compounded nutrients" and therefore do not need ordering if you are intending to use these compounded interventions.
3. The European Commission has unfortunately determined that use of the word "probiotic" and/or "prebiotic" on a label is making a health claim - which needs to be authorised, effectively banning import of any products with matching labels within EU countries, at least via any of the compliant online marketplaces such as Amazon and eBay. A workaround is to use https://www.shipito.com which provides a "free" US mailing address, for these or any other products with similar problems.
At this time, there are 3 products in the schedule affected where no other direct solution has been found.
These can be quickly identified by setting the Region to "EU" and entering "amazon.com" in the Search field in the area above the table below.
4. Magnesium L-Aspartate appears to have erroneous restrictions for some EU countries. The product link in the table for the EU region has the country "Austria" embedded in the link, to add it to the cart more smoothly. The correct EU destination country can be set at the checkout, or you can use https://www.shipito.com, as per Note 3.
5. A UK-based bulk powder vendor https://www.lifelabsupplements.com/ is likely to be added in the next update. They ship worldwide.. apart from EU.
Compounded nutrients
| DMSO-based liquid vitamins and minerals, DMSO-ready multivitamin/mineral capsules and sublingual vitamin/mineral troches for many key nutrients can be found in 4.2 Compounded nutrients. |
Bacteriophage product selector
Clicking on any product link symbol in the bacteriophage "Pathogen vs Product" table below will take you directly to a vendor's webpage in Belarus called Cosmoll.org. (In the event their website is unavailable, they're also contactable via WhatsApp messaging, during their business hours on +7 904 751-48-55). They have been friendly and reliable to deal with. Shipping to eg. Australia may take 2-3 weeks.
NB. Due to difficulties with cross-border payments to this region, Cosmoll uses payment processors such as Wise.com and Paysend.com to facilitate orders. The overall process is a little clunky, but much smoother if you set up a Wise or Paysend account and mobile app before placing your order. The company will try to contact you on WhatsApp or email and manually send a payment request, once the order is received and ready to be processed.
If you run into show-stopping difficulties with the order process, some of the bacteriophage products, eg. Intestifag, Sextaphag and the other bacteriophage products that come in sterile vials are also available at RU-Pills, however they use a Bitcoin intermediary for payments. Overall, access to these products needs to get simpler.
If you have a suitable budget, you can also contact the Phage Therapy Center in Georgia, who have thousands of phages in their biobank and make custom phage cocktails, based on your sample specimens.
The bacteriophage "Pathogen vs Product" table below can help you choose the correct products for your application. For online users, you can also type in (part of) the species or genus name into the search field and the table contents will shrink to just those records, eg. typing "kleb" will return all products targeting Klebsiella species.
Apologies, this table is too large for mobile devices and is best viewed on a computer.
Product notes:
1. Whilst the Viera products have very broad coverage for pathogenic species eg. combining "Spray for women" and "Hand spray", these products are sold as 'prophylactic' doses - you may need to use more of the product to achieve the same results. They also contain PEG, for anyone with sensitivity. Interestingly enough, although these are marketed as external use products, a number of the Viera sprays broadly target the Bacteroides genus. This has implications for selectively correcting elevated Bacteroides : Firmicute ratios and may be (potently) helpful at eg. 8-10 sprays per day, orally for 1-2 weeks. Anecdotal reports are favourable, accompanied by initial die-off symptoms.
2. The Micormir gel bacteriophage products, eg. Phagodent, Fagogin, Phagoderm, Otofag are 'therapeutic doses' and potent.
3. All of the bacteriophage products which come in sterile vials are extremely potent. These will require eg. 20-30ml syringes and detachable eg. 23-27G 1/2 -1" needles to draw up liquid from the vials, before removing the needle to administer them to various mucosal tissues.
4. Nebuliser usage - the Micromir Gel products contain a carbomer base which readily dissolves in water, meaning it is able to be used in a nebuliser at roughly 1mL of gel to 3mL of water. Target dose is typically 1-2mL per session. The sterile vials can be used without dilution in a nebuliser. Nebulising phages has been used in at least one study to achieve systemic distribution, also noting that circulating bacteriophages via this route would normally trigger a systemic immune response, just like IV phage administration.
https://www.mdpi.com/1999-4915/14/12/2614
https://pubmed.ncbi.nlm.nih.gov/26691737/
5. Translated product manuals from Russian to English for Sextaphag, Pyofag and Intesti-fag are provided, courtesy of ChatGPT. Original manuals, etc., can be found on the manufacturer's websites: https://www.bacteriofag.ru/, https://micromir.bio/eng, https://www.veira.net/
6. Peer-reviewed literature exists for various products, eg. https://journals.uran.ua/index.php/2307-0404/article/view/221232
This section contains an ongoing effort to curate frequently asked questions which can't be easily preempted / prevented by clarity updates to the existing protocol documentation.
You can use the search field for keywords, and / or browse through the question / answer pairs.
You can browse the changelog as-is, or use the filter tools to show only the changes between version numbers and / or date ranges by entering a value in one of the relevant "From" fields.
You can also filter by Type to eg. show only "Product" changes, which can be helpful for people already doing the protocol.