The disease model is a complex topic and although the videos and diagrams provided may be helpful if you enjoy deep biochemistry, that's not often the case. Therefore, I’ll attempt to provide a friendlier / less technical explanation for a general audience, although some biochemistry knowledge will be required to understand parts:
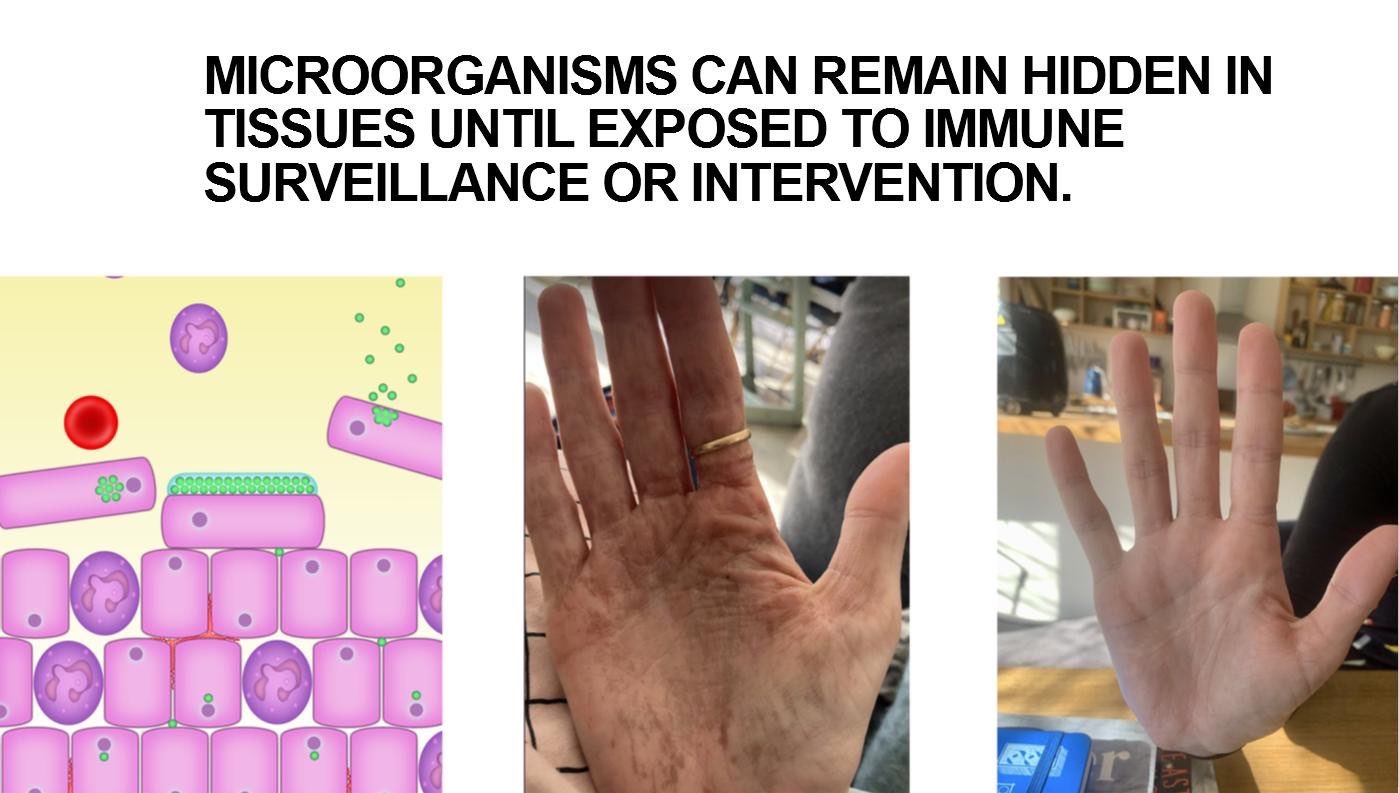
Primarily, what’s driving / allowing the disease to be created is a blind spot in the immune surveillance which allows pathogenic reservoirs to exist in biofilms created by microorganisms. These may be in your nose, mouth, lungs, gut, sex organs, etc., or even circulating.
(These "pathogenic" biofilms normally grow slowly over decades and appear to be associated with aging, also - which is another exciting part of the model).
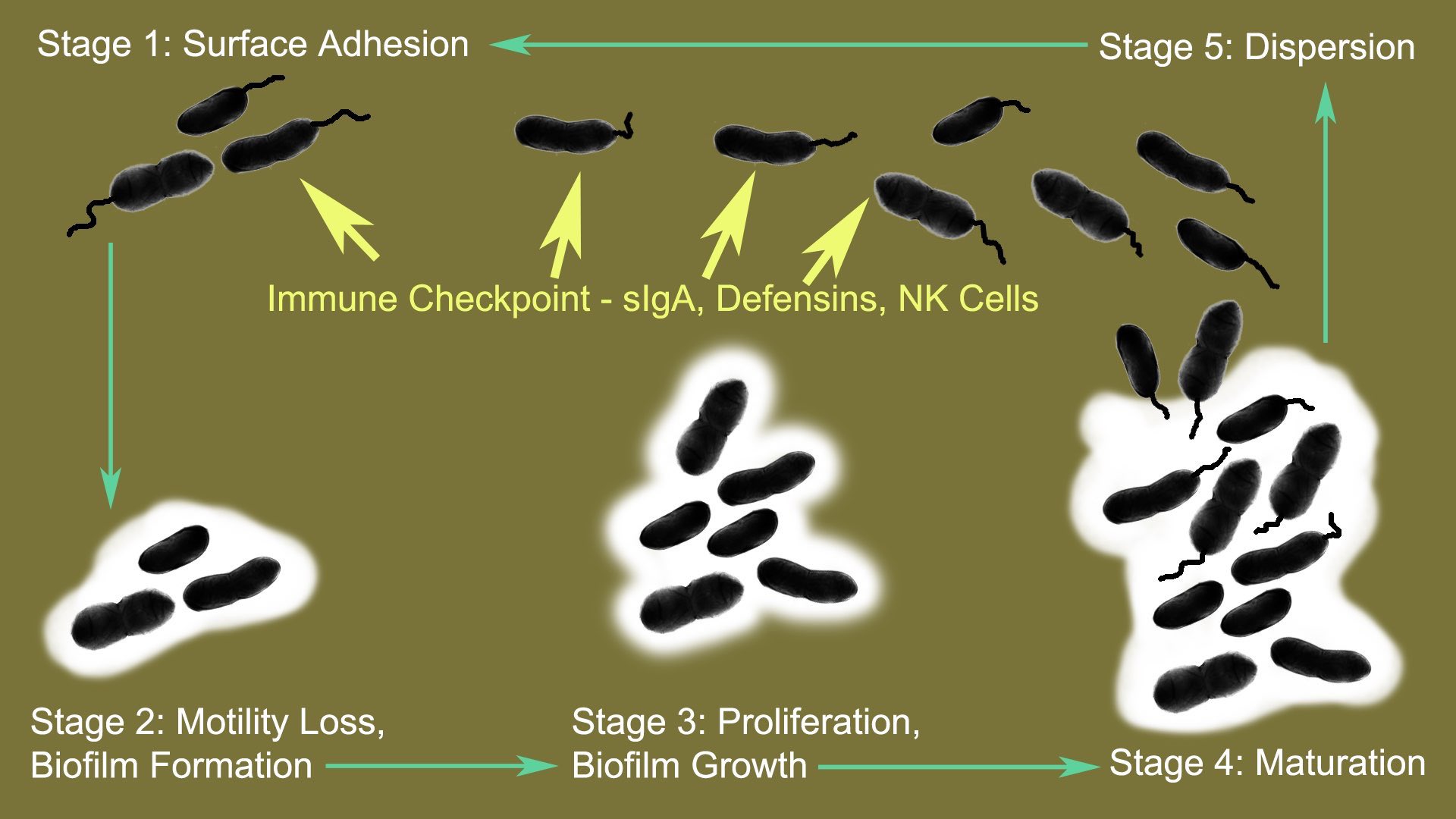
The immune system can suppress biofilm expansion by providing an immune checkpoint for the "planktonic stage" for the pathogenic microbial lifecycle, which is where the microbes are motile and disperse outside the biofilms to restart the lifecycle.. unless the immune system is distracted by another antigen (infections, injections) or dysregulated for other reasons, eg. drugs, trauma, stress.
One of the primary toxins is the primary metabolite of alcohol, acetaldehyde. The toxins produced by these pathogens interrupt energy metabolism and other pathways, affecting immune response, gut barrier integrity and triggering mast cell activation, elevated histamine, etc.
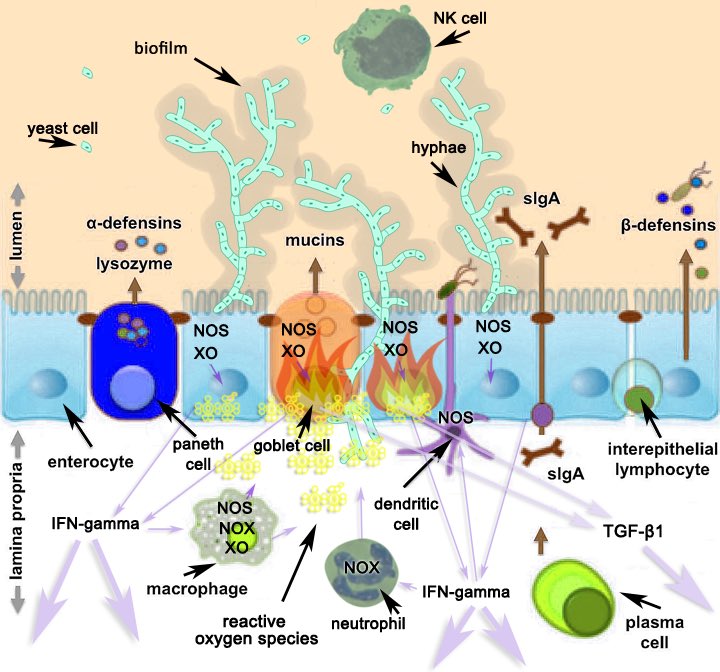
This part of the cascade allows microbial infiltration and an innate immune response pathway which uses reactive oxygen species to kill pathogens.
The immune -> inflammatory cascade causes specific mineral deficiencies, further energy and immune dysregulation (allowing collateral damage to nearby cells / epithelium) and eventually leads to severe microbiome dysbiosis.
These issues create a never-ending cycle - you are unfortunately now immunocompromised.
Once the mineral deficiency profile reaches a dysfunctional level, with particular focus on zinc, copper, selenium, manganese and iron (chromium, iodine, etc also important), the energy metabolism and oxidative stress becomes significantly problematic. The immune system becomes further compromised.
There are a number of catalysts which can trigger this persistent state, even including chronic stress, sleep deprivation and/or traumatic brain injury (TBI).
Conceptually, anything which dysregulates (or distracts) the immune response for a period of time can rapidly push someone down the slippery slope towards this type of dysbiosis. Rapid gut microbiome changes can also cause this.
Protecting you from this cascade / disease progression are eg. Bifidobacterium and Lactobacillus species which can metabolise the acetaldehyde burden into acetate (both mast cell activators) instead of your body, while degrading biofilms and inhibiting a number of the pathogenic species.
Losing the Bifidobacterium species / abundance rapidly accelerates this disease cascade and increases the endo/mycotoxin burden on the host metabolism and creates further reliance of the immune system to arrest the planktonic stage of the pathogenic lifecycle.
A slow progression is also possible - all of these issues appear in aging populations, too. We’ve historically thought of that as “normal”.
It’s also been observed in Long COVID, Post Vaccine Syndrome... and ME/CFS for some years before the pandemic. Something I pondered was “how” the Bifidobacterium can be rapidly destroyed.
All that is required is a catalyst event (virus / viral reactivation, various drugs, vaccination, etc) that creates (lactic) acidemia and kills off the Bifidobacterium, etc. to push someone rapidly into ME/CFS criteria.
One scenario involved (lactic) acidemia, where anaerobic glycolysis is being triggered by a "sensor" protein, Hypoxia Inducible Factors (HIF-1a) being stabilised / promoted - eg. IFN-alpha triggering antigen from infection / reactivated virus, vaccination, impaired glycolysis, (coagulation | anaemia | trauma ->) hypoxia, etc.
Where lactic acid is not being metabolised into pyruvate efficiently, eg. low intracellular zinc or NAD+, this creates an extracellular and circulatory pH crisis that is partially managed by excess lactic acid being secreted into the GI tract.
This lowers the pH and much like the protective effects of stomach acid, but in a different part of the bowel, inhibits pH sensitive species, such as Bifidobacterium.
In this way, a number of catalysts can trigger a rapid change to the microbiome diversity and someone can find themselves finally pushed into “ME/CFS metabolism”, as described in my disease model, albeit with their personalised array of variables on top of the primary cascade, eg. intracellular mineral profile and its effects on (energy) metabolism , “pathogenic” biofilm locations and localised effects from endotoxins / mycotoxins, etc.
Importantly, this also means that until you resolve metabolic conditions triggering anaerobic glycolysis / (lactic) acidemia, you’re going to struggle in restoring Bifidobacterium populations.
The host metabolism needs to be addressed at the same time as the microbiome or you’ll continue to go around in circles, indefinitely.
The disease progression could also be a series of smaller events over a period of time. eg. If this happens during childhood before critical developmental period, adaptation around this metabolic landscape can be expected - lactic acid also triggers neurogenesis.
I strongly suspect we’re now describing the origins for autism spectrum disorders and you may have also noticed a strong association between autism spectrum disorders (ASD) and ME/CFS patients. A recent paper, “Childhood neurodivergent traits, inflammation and chronic disabling fatigue in adolescence: a longitudinal case–control study”, observed the association.
https://bmjopen.bmj.com/content/14/7/e084203
Another prediction of my disease model is that neurodiversity is an early stage of the biofilm-related energy metabolism alterations.
The pathogenic biofilm growth is accelerated by frequent exposure to (viral) antigens, distracting the immune system from suppressing microbial proliferation / planktonic stage and biofilm surface area expansion (see image).
This mitochondrial dysfunction before critical developmental periods induces elevated lactic acid metabolism, leading to enhanced neurogenesis (and myogenesis, with exertion). It is both a blessing and a curse, depending on the circumstances.
https://frontiersin.org/journals/neuroscience/articles/10.3389/fnins.2019.00403/full
However, this lactic acid metabolism comes with elevation of endogenous oxalate production (lactate dehydrogenase elevation also converts glyoxylate to oxalate), especially if the active form of Vitamin B6, pyridoxal 5-phopsphate (P5P) is low.
https://pubmed.ncbi.nlm.nih.gov/1417880
The dysbiosis cascade described in the model also creates aldehyde metabolism impairment.
https://ncbi.nlm.nih.gov/pmc/articles/PMC4910734/
Variables inside the disease cascade control feature presentation and severity, eg. post-exertional malaise (PEM), postural orthostatic tachycardia syndrome (POTS), mast cell activation syndrome (MCAS), fatigue, renal dysfunction, collagen synthesis issues, gut and other mucosal tissue issues, sex hormone dysregulation, cortisol dysregulation, cholesterol elevation, serum Vitamin A and B6 elevation, glucose metabolism impairment/ insulin “resistance”, sleep disorders, neurotransmitter homeostasis dysregulation, body temperature regulation issues, muscle tremors and activation issues, chronic viral reactivation issues. This is not an exhaustive list - just some of the highlights.
eg.
Liver glycogen / hepatic gluconeogenesis and oxidative stress are the 2 major variables in a crash / PEM.
Muscle glycogen, electrolyte sufficiency, circulation and ATPase activity are the major variables in POTS.
These symptoms can be influenced by immune activity and/or physical activity, which present similar metabolic burdens. Acetaldehyde can significantly influence the energy metabolism involved.
Oxidative stress can be managed initially via dietary antioxidants and longterm, can be prevented by correction of the mineral deficiencies affecting metalloenzymes CuZnSOD, MnSOD, catalase (heme), glutathione reductase + peroxidase (selenium + riboflavin metabolism related mineral and cofactors, which also includes the thyroid hormone pathway - calcium, heme, magnesium, zinc, iodine and molybdenum). The pathogenic microbial species reservoirs hidden in biofilms will also need to be resolved.
Chronic viral reactivation is a common issue. Dysregulated interplay between innate immune response pathways is heavily implicated by the model.
IFN-alpha activity “primes” (eg. xanthine dehydrogenase) and then is directly inhibited by IFN-gamma activity, via a JAK/STAT related pathway.
There are influences affecting bias towards IFN-alpha vs IFN-gamma responses, eg. exertion and heat promote IFN-gamma. Elevation of IFN-gamma then inhibits IFN-alpha activity.
For IFN-alpha, apart from the baseline profile of co-infections, one of those influences relates to mitochondrial dysfunction.
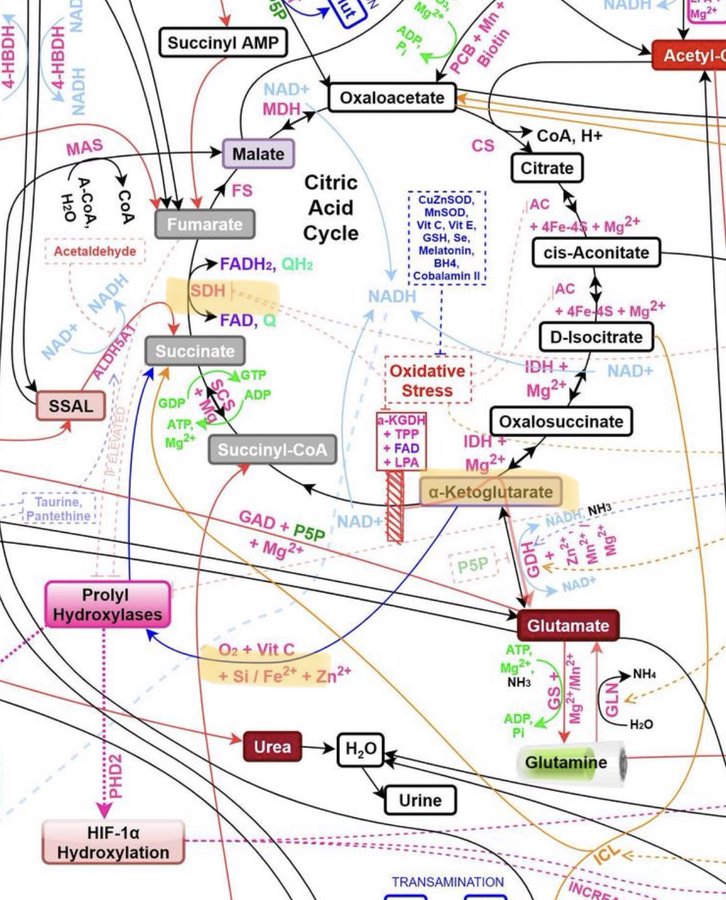
HIF stabilisation by prolyl hydroxylase inhibition leads to pyruvate dehydrogenase (PDH) inhibition and lactate dehydrogenase (LDH) promotion via transcription factor alterations.
"Anaerobic glycolysis" follows and reactivation of latent herpesviruses, providing an antigen that triggers an IFN-alpha response.
If the metabolic issues affecting prolyl hydroxylase activity are not resolved, you can expect chronic reactivating human herpesviruses, etc.
eg.
1. Insufficiency of substrate, alpha-ketoglutarate for various reasons (low TCA cycle flux in early reactions, low Mg, elevated transamination activity, etc)
2. Elevation of succinate (perhaps via inhibition of succinate dehydrogenase - low FAD, itaconate, etc)
3. Hypoxia.
4. Oxidative stress / low vitamin C.
5. Low Fe/Si /Zn.
These factors are readily quantifiable and reversible.
Overall, reversing the disease trajectory requires targeting multiple issues -
1. Quantifying and correcting the mineral and other deficiencies to restore parts of the metabolism, especially glycolysis and for oxidative stress, but much, much more. Oral doses of minerals are inhibited by the cascade, so alternate routes are needed. Resolving these issues also halts issues with chronic reactivating human herpesviruses, etc.
2. Correcting the dysbiosis, biofilms and infections in all mucosal interfaces and circulation.
3. Managing / rehabilitating structural issues, lymphatic system, etc
4. Dealing with the trauma / PTSD.