Maintaining electrolytes can be challenging, due to expected renal dysfunction in this disease model. If you are suffering from any pre-existing kidney disease consult your doctor prior to supplementing any of these elements.
Maintaining your electrolytes is arguably one of the most critical goals for your daily micronutrient intake, relative to your quality of life. According to the intracellular data collected and disease modelling, these are highly problematic in many chronic diseases, yet poorly captured by standard serum testing.
Serum levels of electrolytes are tightly regulated and often fail to help indicate intracellular or systemic levels until your status reaches a level where an emergency hospital visit is required.
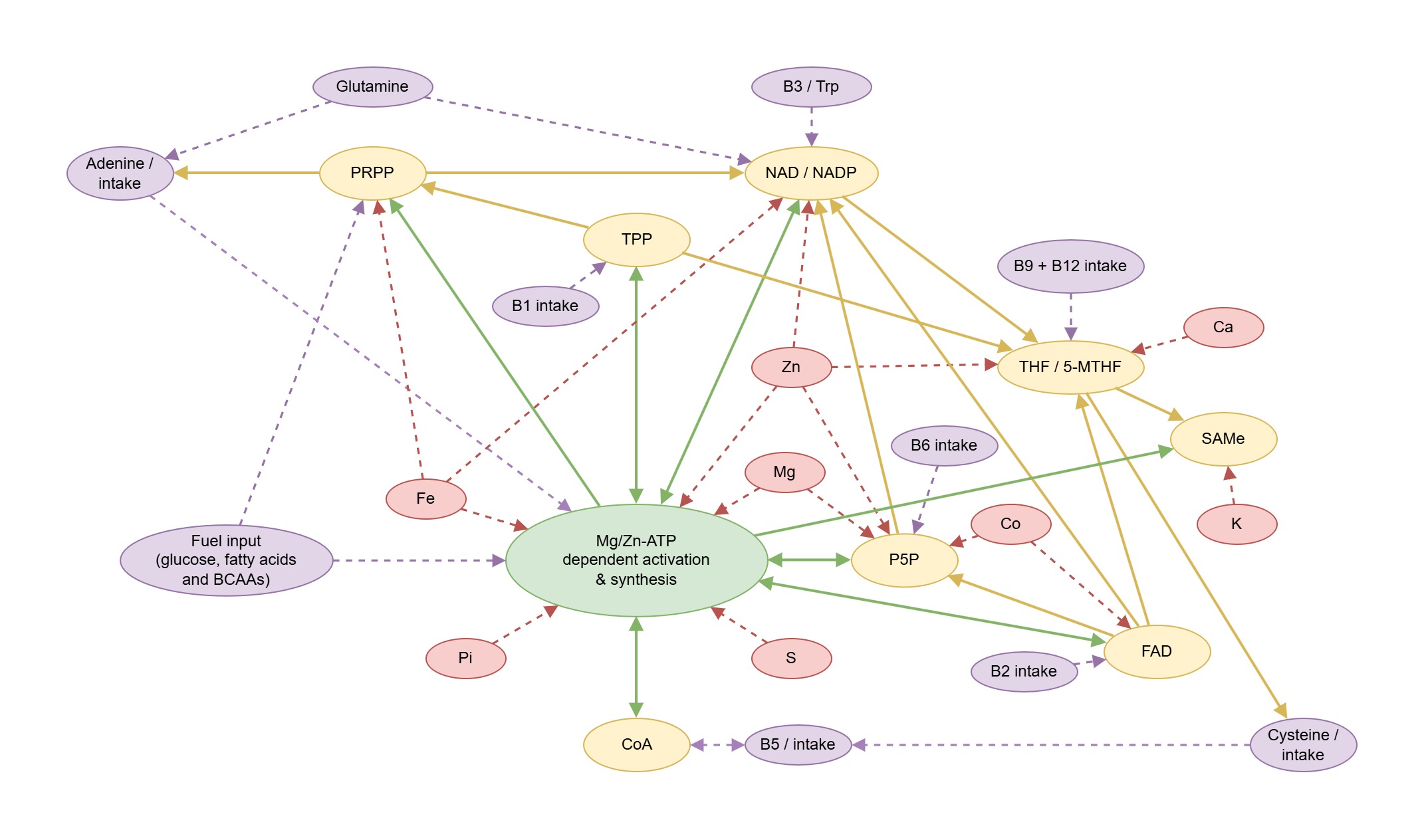
Electrolytes include potassium, sodium, calcium, magnesium, phosphate, chloride and bicarbonate. Electrolytes are required for ion channels / transporters, signalling pathways, blood pressure regulation any many important metabolic pathways. Electrolytes and minerals are required building blocks for ATP, GTP, UTP, TPP, FAD, NAD+, NADP, P5P, CoA, glycogen, pyruvate and many other important currencies, cofactors and metabolites.
When electrolytes are deficient, neurological symptoms, fatigue, muscle spasms and pain/inflammation may occur (skeletal, smooth and cardiac tissues). Digestion and nutrient absorption may be impaired. Low electrolytes and especially low phosphate and/or magnesium, where caused by acidosis, can inhibit mineral repletion efforts.
Electrolytes can “exchange” at the cellular membrane as pairs by pumps called "ATPases", which consume approximately 2/3 of ATP produced inside the cell, to maintain functional levels of each electrolyte inside and outside the cells.
For example:
The Na+K+-ATPase exchanges sodium : potassium.
The Ca2+-Mg2+-ATPase exchanges calcium : magnesium.
Under extreme metabolic conditions, alternate exchangers, such as the Na+/Ca2+ exchanger (NCX) can exchange sodium : calcium, too.
This is not an exhaustive list.
For this reason, a deficiency of one electrolyte in the pair can create
issues absorbing and retaining the other, creating a secondary
deficiency. Ideally, deficiencies for electrolytes should be addressed as pairs, or all at once, to prevent exacerbating an existing imbalance.
Intracellular deficiencies for each electrolyte can come from various influences other than simple dietary deficiency of it and / or its "exchanging partner", eg.
Calcium deficiency can also be created by parathyroid hormone (PTH) issues downstream of eg. low iron and phosphate. Other influences include elevated oxalate synthesis, low Vitamin D, low Vitamin K2 mk7 and excessive NCX activity.
Common symptoms include low energy, low neurotransmitter synthesis, sleep disturbances, muscle tremors and osteopenia.
Magnesium deficiency can also be created by silicon deficiency and chronic diarrhoea.
Common symptoms include low energy, low neurotransmitter synthesis, sleep disturbances, muscle tremors and constipation.
Sodium deficiency can also be created by chronically elevated IFN-gamma and CYP2D6 enzyme activity in the kidneys, which produces renal dopamine and promotes renal sodium excretion. Other influences include frequent diarrhoea, vomiting or sweating. Above daily values of sodium intake are required during periods of immune activity.
Common symptoms include low energy, dizziness, nausea, muscle tremors and low blood pressure.
Potassium deficiency can be created by chronic alcohol / acetaldehyde, chronic kidney disease / infection, diabetic ketoacidosis, frequent diarrhoea, vomiting or sweating, folate deficiency, chronic elevation of aldosterone.
Common symptoms include low energy, low neurotransmitter synthesis, muscle tremors and high blood pressure.
Phosphate deficiency can also be created by chronic alcohol / acetaldehyde elevation and also acidemia, triggering renal excretion of phosphorus. This can come from metabolic or respiratory acidemia / acidosis. Elevated lactic acid + low intracellular zinc is one mechanism which can allow elevated lactic acid from an energy crisis, mineral deficiencies or hypoxia to progress to acidemia / acidosis. Low phosphate (and other electrolytes) can create broad metabolic impairments, which can spiral and lead to lowered baseline / lactate threshold.
Common symptoms include low energy, muscle tremors / poor strength, seizures, rhabdomyolysis, respiratory suppression, softening of bones and teeth.
Bicarbonate deficiency can also be created by metabolic acidosis, chronic diarrhoea, elevated oxalate levels and chronic kidney disease / infection.
Common symptoms can include tachycardia, confusion and fatigue.
Chloride deficiency has not been commonly observed.
Most electrolytes should be consumed slowly over the day. They may cause diarrhoea and other symptoms in large doses. Magnesium studies showed elevated excretion and only 10% retention from larger oral doses.
https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC1855626/
Transdermal administration has been demonstrated as a superior route for magnesium absorption due to the "slow-release" aspect. Rapid absorption and downstream elevation of serum electrolytes triggers rapid excretion to restore homeostasis, resulting in poor electrolyte retention and wasted effort. This can be exacerbated by low activity levels and intracellular deficiency of the corresponding partner in the electrolyte pair.
Electrolytes are commonly available as salts, and the second table below outlines the relative amounts of each electrolyte in these salts.
The weekly DIY "sipper/shot" recipe contains suggested amounts based on poor dietary intakes from food sources and can be adjusted where necessary. A link to an electrolyte calculator can be found at the bottom of this section.
People with a history of anxiety and / or neuropsychiatric symptoms may be sensitive to calcium and potassium repletion and need to onboard them more slowly. Monosodium phosphate can be used as an alternative phosphate source during this time at eg. >5g / day, after ramping up.
Starting magnesium and/or phosphate can improve glucose uptake and glycogen synthesis. Experiencing symptoms that resemble hypoglycaemic events or diabetic "hangry" mood alterations may indicate more dietary carbohydrates are needed.
TOTAL daily (elemental) targets from all food / supplement sources
| Element | Target Daily Amount | Notes and Sources |
| Sodium Na | >4g | (Daily value is 2300mg. More is required than normal, due to elevated excretion rate from glycogen depletion and innate immune activity cascade.) 5g (1 teaspoon) of table salt contains 1.95g Na. |
| Potassium K | >5g | (Daily value is 4700mg.) 10g of Nu-Salt (potassium chloride) contains 5g of K. 3 large potatoes (900g) contains roughly 5g of K. |
| Magnesium Mg | >500mg | Supplemental regimen should include transdermal route, where deficient. |
| Calcium Ca | >750mg | Increase supplementation to 1.5–2g if deficient. Cronometer can help visualise your calcium intake. CMA results show intracellular calcium deficiencies. Low phosphorus and also low strontium in hair testing may also infer calcium status. Oxalate dumping can be expected initially with repletion. |
| Phosphate Pi | >1g | Meat, dairy, pumpkin seeds / pumpkin seed oil, red lentils, sunflower seeds, potatoes. Supplement if deficient. Supplements which combine phosphorus with various electrolytes, e.g. calcium phosphate, may be available in some regions. Much higher intakes may be required in severely depleted states. |
| Bicarbonate HCO3 | As needed | Commonly found in sodium bicarbonate / baking soda (NOT baking powder)
and/or potassium bicarbonate. A typical dose is 1/4 teaspoon, AWAY FROM
MEALS, multiple times per day - if lactic acid / oxalic acid is elevated
and/or phosphorus is either high OR low in OAT results, or phosphorus /
sulphur is low in Oligoscan. |
Reference material: Elemental weights, by compound, for calculating servings of various electrolytes
| Electrolyte Compound | % Weight Proportions | Example Weight Proportions |
| Sodium Chloride NaCl | Na 39%, Cl 61% | 6.4g contains 2.5g sodium & 3.9g chloride |
| Potassium Chloride KCl | K 52%, Cl 48% | 9.6g contains 5g potassium & 4.6g chloride |
| Magnesium Chloride MgCl2 | Mg 26%, Cl 74% | 2g contains 520mg magnesium 1.48g chloride |
| Sodium Bicarbonate NaHCO3 | Na 27%, HCO3 73% | 5g contains 1.4g sodium & 3.6g bicarbonate |
| Potassium Bicarbonate KHCO3 | K 39%, HCO3 61% | 12g contains 4.7g potassium & 7.3g bicarbonate |
| Calcium Citrate C12H10Ca3O14 | Ca 24% | 4g contains 960mg calcium & 3g citrate |
| Potassium Citrate C6H5K3O7 | K 38% | 13g contains 4.9g potassium & 8.1g citrate |
| Monosodium Phosphate NaH2PO4 | Na 19%, P 26% | 6.6g contains 1.25g sodium & 1.7g phosphorus |
| Disodium Phosphate Na2HPO4 | Na 32%, P 22% | 7.7g contains 2.5g sodium & 1.7g phosphorus |
| Monopotassium Phosphate KH2PO4 | K 29%, P 23% | 7.5g contains 2.2g potassium & 1.7g phosphorus |
| Dipotassium Phosphate K2HPO4 | K 45%, P 18% | 10g contains 4.5g potassium & 1.8g phosphorus |
| Monocalcium Phosphate CaH4P2O8 | Ca 17%, P 26% | 5g contains 0.9g calcium & 1.3g phosphorus |
| Dicalcium Phosphate CaHPO4 | Ca 29%, P 23% | 3.8g contains 1.1g calcium & 870mg phosphorus |
| Magnesium Aspartate C8H12MgN2O8 | Mg 8% | 6g contains 500mg magnesium 5.5g aspartate |
An electrolyte calculator tool can be found here - https://bornfree.life/learn/electrolyte-calculator/