This protocol involves several steps that require multiple tests and a wide range of important supplements. While the expected results are unlikely to be realized without completing all these steps, efforts have been made to simplify them as much as possible. The steps are as follows:
- Collect your data
- (Optional) Pre-protocol support
- Lifestyle changes, plus ongoing transition from sympathetic overdrive -> parasympathetic balance, as the metabolism allows
- Stage 1: Remineralisation, increasing collagen synthesis rates, and performing a controlled initial “die-off” (at least two weeks)
- Stage 2: Enhanced gastrointestinal and mucosal interventions (at least two weeks)
- Stage 3: Stimulate and support a strong immune response while breaking (circulating) biofilms (at least four weeks)
- Optional follow-up
- Ongoing preventative maintenance
"Be thankful for your triggers, for they show where you are not free."
We fully anticipate that individuals exploring this protocol may be highly sensitive to supplements. The reasons for this sensitivity are detailed in the disease model and have been accounted for within the protocol. The sensitivity to supplements and foods is expected to resolve as part of the protocol.
One of the most important lessons learned through this process is that ultimately, whenever a basic, essential nutrient triggers an initial reaction - either good or bad - you need it, although you may also unmask other deficiencies / compensations in the process of correcting one.
That stated, blindly charging your way through barriers is not a sensible way to achieve success, and there is a structured process to follow which makes nutrient repletion much more tolerable.
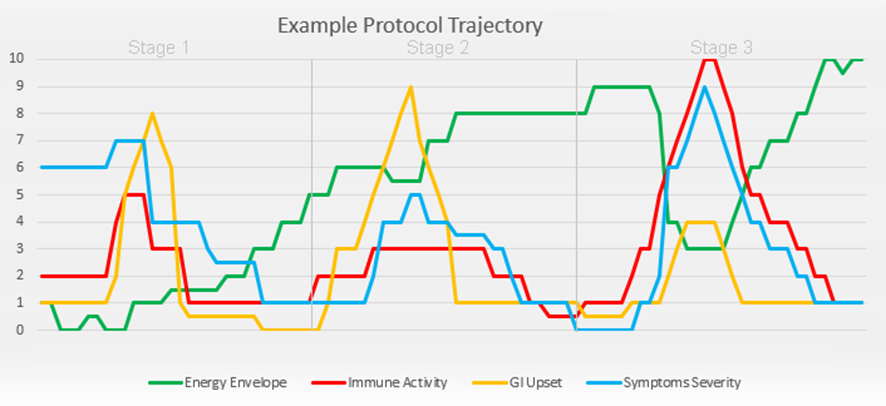
This protocol is designed to stimulate immune activity and may produce a “J-curve” trajectory, meaning you might feel progressively "quite sick" at the beginning of each stage. Increasing energy availability allows for heightened immune activity, which prioritizes energy metabolism toward these goals and can temporarily intensify symptoms. Carefully maintaining levels of electrolytes, copper, zinc, iron, manganese, selenium, glycogen, and B vitamins may help prevent severe symptoms and post-exertional malaise (PEM) or "crashing."
Your individual experience may vary based on factors such as the pace of protocol implementation, the pathogens involved, your initial baseline condition, and the consistency and accuracy of your daily participation. Avoiding or delaying parts of the protocol can hinder progress and potentially lead to unnecessary discomfort. Support is available through our Discord discussion group.
Before beginning, assess your lymphatic system as described in the “2.2.2 Lymphatic Maintenance” section. Note any tissues that have been or continue to be sore, stiff, or inflamed—these areas are expected to flare during increased immune activity and may be adjacent to other infected tissues.
To help reduce expected symptoms when correcting deficiencies and experiencing Herxheimer reactions (microbial die-off effects) due to improved immune activity, a recommended starting sequence has been provided.
The "die-off effect" can cause a range of temporary but highly debilitating symptoms, including headaches, nausea, additional fatigue, dizziness, swollen glands, bloating, gas, constipation or diarrhea, joint or muscle pain, tachycardia, chills, cold hands or feet, itchiness, rashes, sweating, and fever resembling the "disulfiram effect."
A schedule of specific products is available, with vendor website links provided for different regions (see “5. Ordering Products”). These are not affiliate marketing links. With the exception of the Oxalobacter.com
website (which was created out of necessity to address worldwide supply issues for
"Oxalobacter formigenes" probiotics and is not intended as a for-profit
endeavor), there are no financial incentives or benefits from providing links to products or tests. If you encounter supply shortages, please try to find the same product from another vendor or ask for help in the online Discord discussion group.
Deviating from the recommended starting order or substituting products may lead to avoidable and unpleasant symptoms or may simply be ineffective. You can space out the stages further if needed. Despite the extensive list of supplements—aside from one or two items included to make your experience more tolerable—all are necessary. Attempts to create a "lite" version of this protocol by swapping or omitting items have consistently resulted in failure.
Stage 1 focuses on delivering missing minerals and other nutrients to the body, sometimes via non-oral routes, to resolve measurable deficiencies caused by inhibited oral absorption of these micronutrients at levels typically found in foods. While this helps restore normal metabolism, these nutrients are also accessible to the microorganisms inhabiting your body. Therefore, an additional goal of selectivity is required, targeted by a combination of probiotics and antimicrobial interventions. Some of these interventions are included in Stage 1, while others are introduced in Stages 2 and 3.
It is not advisable to take the Stage 1 metabolic support supplements for an extended period without progressing to the parts of the protocol that address microbiome dysbiosis, such as dietary optimisation. Otherwise, you may feel increasingly better at first, but over time this may lead to amplification of existing microbiome issues. Nutrients that benefit your cells also benefit microorganisms that depend on you, and vice versa.
Fulvic acid is used extensively in Stage 3 of the protocol. Due to its potent ability to "liberate" and recirculate metals sequestered during chronic inflammation; it is recommended to test your response to a single drop of Good State Ionic Man (fulvic acid multi-mineral) diluted in a glass of water during Stage 2. Increase the dosage slowly. Fulvic acid is also a potent biofilm breaker. If you experience any unpleasant effects, take a few days to gradually increase from a smaller dose—for example, place a drop in a bottle of water, mix it, and then transfer a drop from this first dilution into another glass of water—until you can consume a standard serving without adverse effects.
If you have nasal inflammation or notice any airway resistance or restriction when breathing, it may be appropriate to perform a nasal microbiome test and investigate for environmental mould issues. Unwanted microorganisms such as Candida, Aspergillus, Streptococcus, Staphylococcus, and Klebsiella species are sometimes found in the nasopharynx. These tests may also indicate the susceptibility of detected strains to interventions like fluconazole, itraconazole, voriconazole, or amoxicillin.
If your levels of magnesium, zinc, molybdenum, selenium, iron, iodine, or calcium are low, you may experience additional symptoms related to aldehyde metabolism insufficiency. These symptoms can be exacerbated by consuming excess alcohol, histamine, polyethylene glycol (PEG), vitamin A, or vitamin B6.
Issues with neurotransmitter metabolism, histamine regulation, and gut function are common and to be expected.
Correcting severe electrolyte deficiencies can temporarily create paradoxical effects, including increased metabolism rates and heart rate. Consuming certain minerals like copper or zinc on an empty stomach can easily induce nausea.
If taurine or magnesium affects your sleep or causes palpitations, tremors, or if you feel worse upon starting them, this may indicate a calcium deficiency. Adding 1–2 grams of elemental calcium per day, along with vitamin D3 and vitamin K2 MK-7, may help correct this. Be aware that addressing a calcium deficiency can initiate the process of oxalate dumping, which is necessary but may cause muscle pain. Low calcium levels may coincide with strontium and phosphorus deficiencies. The tests included in this protocol will help identify these issues. Low strontium levels in hair testing may serve as a proxy indication for calcium deficiency.
Correcting an iodine deficiency is likely to temporarily increase anti-thyroid peroxidase antibodies (anti-TPO) and Thyroid Stimulating Hormone (TSH), enhancing the activity of the sodium-iodide symporter (NIS) while improving levels of triiodothyronine (T3) and thyroxine (T4).
We recognise that the extensive list of individual supplements required for this protocol presents a new challenge. We are collaborating with compounding pharmacies to simplify this process - transforming most of Stage 1 into sublingual lozenges (troches) or DMSO-based multivitamin, and a tub or bag of premixed powder. A DIY powder recipe is also included for those who prefer to mix their own.
Consuming mixed inositols will signal your cells to increase glucose uptake and glycogen synthesis, promoting glycolysis over other energy pathways. Inositol inhibits catalase, which may decrease your capacity to handle oxidative stress during immune activity, necessitating additional antioxidant support. If your liver and muscle glycogen stores are low - which is expected - you may initially feel extremely hungry or experience hypoglycemic symptoms such as dizziness, depression, and extreme fatigue. Consuming up to 500 grams of additional net carbohydrates and water over two to three days to replenish glycogen stores should help you feel significantly better. Glycogen binds with water at a 1:3 ratio, so your total body mass may increase by around 2 kilograms. Note that inositol can be problematic if you are following a ketogenic diet. D-chiro-inositol should be started at approximately 2.5 mg and very slowly increased as tolerated.
(Optional) Pre-protocol support
Remineralisation Will Alter (Restore) Neurotransmitter Homeostasis or "Managing Transitional Neuropsychiatric Symptoms"
It's critical to note that most of the enzymes responsible for synthesising, degrading, or recycling neurotransmitters are B-vitamin dependent, and their active forms, such as FMN, FAD, TPP, P5P, and methylcobalamin, are functionally deficient in the data of people with chronic illness. This is not always due to dietary inadequacy, even relative to general population requirements. The applied data shows this is due to cofactor bottlenecks, impaired enzymatic activation, oxidative degradation, and zinc- / magnesium-dependent enzyme instability.
This is evident, for example, in the metabolism of vitamin B6. As shown in this detailed diagram of B6 metabolism, converting dietary B6 into its active form P5P involves a cascade of steps: alkaline phosphatase (ALP) activity outside the cell, membrane transport, and intracellular phosphorylation via pyridoxal kinase (PK). Each of these steps is dependent on magnesium and zinc, and many are redox-sensitive. Acetaldehyde, chronic inflammation, and low ATP all interfere. It's no surprise, then, that functional P5P levels are low, even when blood levels of pyridoxine or pyridoxal appear normal or highly elevated.
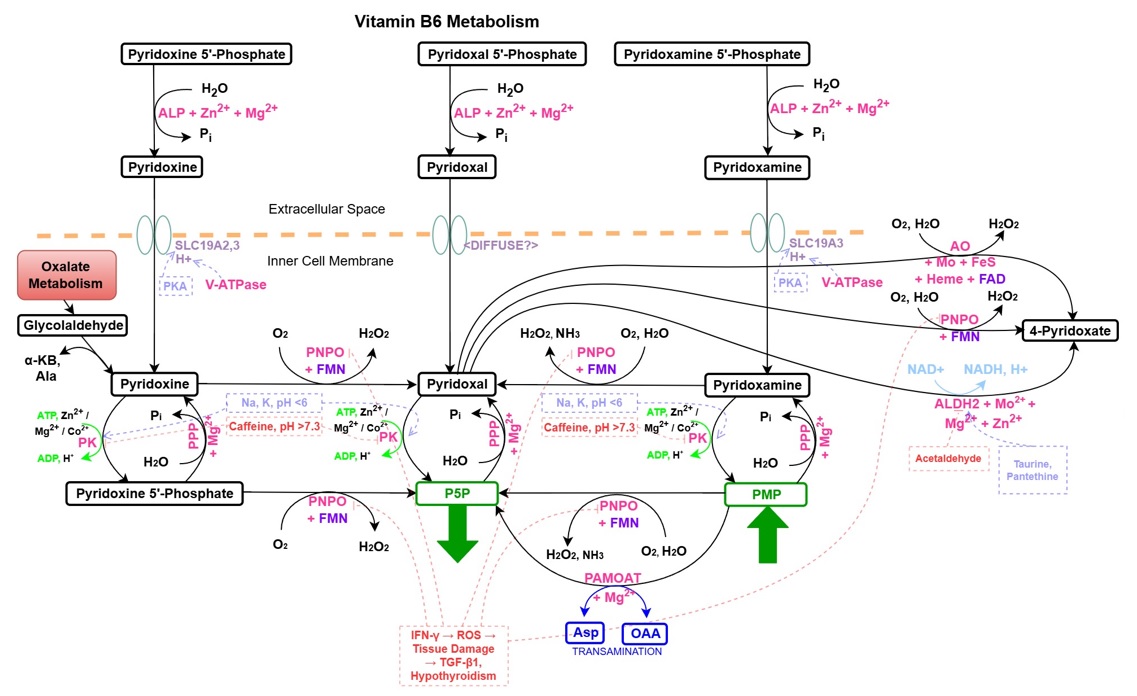
However, this problem isn’t limited to Vitamin B6.
eg. Riboflavin must be converted to FMN and FAD, a process impaired by low ATP, oxidative stress, zinc or magnesium loss. Thyroid synthesis and related minerals, substrates also influence this.

Thiamine must become TPP via thiamine pyrophosphokinase. B12 must be converted to methylcobalamin, a zinc- and glutathione-sensitive step. These are often affected by chronic acetaldehyde, either directly or indirectly.
Acetaldehyde burden affects not only ALDH directly, but also indirectly interferes with zinc-dependent enzymes, magnesium availability, and redox-sensitive pathways throughout this entire cascade. It also stimulates mast cell activation, promoting histamine release, while simultaneously impairing histamine degradation through inhibition of ALDH and depletion of cofactors like P5P and copper. This can disrupt the balance of neurotransmitters by overactivating histamine receptors, and indirectly suppressing dopamine synthesis via H₃-mediated inhibition of tyrosine hydroxylase. It acts as both a primary disruptor and a multiplier of vulnerability in neurotransmitter and cofactor systems.
The result is that small efforts to stimulate or correct neurotransmitter production can trigger paradoxical responses, including overshooting, agitation, anxiety, "brain on fire", insomnia, sedation, getting "stoned" / "high", or what many patients call a “weird” or “off” feeling.
| wdt_ID | wdt_created_by | wdt_created_at | wdt_last_edited_by | wdt_last_edited_at | Compound | General Effect | Sensations When Low | Sensations When Excessive | Relationship | Notes |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 3dghs | 20/04/2025 04:24 AM | 3dghs | 20/04/2025 04:24 AM | Dopamine | Motivation, reward, goal-directed behaviour | Apathy, low motivation, anhedonia, fatigue | Anxiety (if ALDH inhibited / "Disulfiram effect"), hyperfocus, paranoia, addictive behaviour | Upstream: Tyrosine, Tyrosine Hydroxylase (TH); Downstream: DOPAC, HVA, THP | Synthesis inhibited by low [(Zinc, Magnesium->) P5P, (Queuine->) BH4, Tyrosine | Iron | Copper | Calcium | Potassium | Lithium | Oxygen], elevated [Histamine, oxidative stress] |
| 2 | 3dghs | 20/04/2025 04:24 AM | 3dghs | 20/04/2025 04:24 AM | Serotonin | Mood regulation, satiety, sensory filtering | Irritability, insomnia, gut discomfort, sensory sensitivity | Emotional numbness, lethargy, flattened affect | Upstream: Tryptophan, Tryptophan Hydroxylase (TPH); Downstream: 5-HIAA, Melatonin | Tied to Oestrogen, gut microbiota, Tryptophan metabolism. Influenced by IDO1/TDO activation during innate immune responses. |
| 3 | 3dghs | 20/04/2025 04:24 AM | 3dghs | 20/04/2025 04:24 AM | Norepinephrine | Alertness, arousal, vigilance | Brain fog, low energy, insomnia, poor concentration | Panic, insomnia, sympathetic overdrive | Upstream: Dopamine, Dopamine Beta-Hydroxylase (DBH); Downstream: Normetanephrine, VMA | DBH is sensitive to oxidative stress and low Copper. |
| 4 | 3dghs | 20/04/2025 04:24 AM | 3dghs | 20/04/2025 04:24 AM | Epinephrine | Acute stress response, mobilisation | Low physical energy, poor response to stress | Hyperarousal, restlessness, palpitations | Upstream: Norepinephrine, Phenylethanolamine N-Methyltransferase (PNMT); Downstream: Metanephrine, VMA | PNMT sensitive to elevated Cortisol, low Vitamin D, stress immobilisation (rats). |
| 5 | 3dghs | 20/04/2025 04:24 AM | 3dghs | 20/04/2025 04:24 AM | GABA | Inhibition, calm, anti-seizure, muscle relaxation | Anxiety, restlessness, insomnia | Sedation, reduced alertness, depression | Upstream: Glutamate, Glutamate Decarboxylase (GAD); Downstream: SSA, Succinate | Synthesised from Glutamate; linked to P5P and ALDH5A1 |
| 6 | 3dghs | 20/04/2025 04:24 AM | 3dghs | 20/04/2025 04:24 AM | Glutamate | Excitation, memory, learning | Poor focus, cognitive fatigue, low learning retention | Neurotoxicity, anxiety, agitation, excitotoxicity | Upstream: Glutamine; Downstream: GABA, α-KG (via Glutamate Dehydrogenase (GDH)) | Requires P5P, Magnesium, Zinc and GSH balance |
| 7 | 3dghs | 20/04/2025 04:24 AM | 3dghs | 20/04/2025 04:24 AM | Acetylcholine | Learning, attention, parasympathetic tone | Memory loss, low attention, dry mouth, poor digestion | Overstimulation, cramps, sweating, nausea | Upstream: Choline, Acetyl-CoA; Downstream: Acetate, Choline | Synthesised from Choline and Acetyl-CoA. Degradation inhibited by Aflatoxin B1, Territrem B, p-Cresol. |
| 8 | 3dghs | 20/04/2025 04:24 AM | 3dghs | 20/04/2025 04:42 AM | Histamine | Arousal, immune modulation, gastric secretion | Sedation, poor gastric acid, low immune alertness | Itching, hives, insomnia, irritability | Upstream: Histidine, Histidine Decarboxylase (HDC); Downstream: Imidazole acetaldehyde, Methylhistamine | Released by Acetaldehyde. Degraded by Diamine Oxidase (DAO) - requiring Copper, then ALDH2 (inhibited by Acetaldehyde) and Histamine-N-Methyltransferase (HNMT) - requiring SAMe, MAO - requiring FAD, then ALDH3A1 (inhibited by Acetaldehyde); Inhibits TH. |
| 9 | 3dghs | 20/04/2025 04:24 AM | 3dghs | 20/04/2025 04:24 AM | Endorphins / Enkephalins | Pleasure, pain suppression, emotional buffer | Pain sensitivity, low mood, emotional lability | Emotional blunting, addiction potential, hormonal suppression | Upstream: Proopiomelanocortin (Proopiomelanocortin (POMC)); Downstream: μ-opioid receptor binding | Linked to Dopamine, Oxytocin, and μ-opioid tone |
| 10 | 3dghs | 20/04/2025 04:24 AM | 3dghs | 20/04/2025 04:24 AM | Anandamide / 2-AG | Stress modulation, appetite, mood, memory | Anxiety, heightened stress response | Amotivation, reduced memory, low arousal | Upstream: Arachidonic acid, N-Acylphosphatidylethanolamine (NAPE); Downstream: CB1/CB2 receptor activity | Part of endocannabinoid system; modulates Dopamine and GABA |
| 11 | 3dghs | 20/04/2025 04:24 AM | 3dghs | 20/04/2025 04:24 AM | Melatonin | Circadian rhythm regulation, antioxidant | Insomnia, poor sleep quality, circadian disruption | Drowsiness, fatigue, vivid dreams | Upstream: Serotonin, Serotonin N-Acetyltransferase (SNAT)/Acetylserotonin O-Methyltransferase (ASMT); Downstream: Sulfated/oxidised metabolites | Synthesised from Serotonin; impacted by light and inflammation |
| 12 | 3dghs | 20/04/2025 04:24 AM | 3dghs | 20/04/2025 04:24 AM | DOPAL | Dopamine catabolite, redox-sensitive aldehyde | N/A | Neurotoxicity, mitochondrial stress, Monoamine Oxidase (MAO) overload | Upstream: Dopamine via Monoamine Oxidase (MAO); Downstream: THP, DOPAC | Implicated in Parkinson’s, ALDH1A1/1A2/2 sensitivity, Tyrosine Hydroxylase (TH) inhibition. |
| 13 | 3dghs | 20/04/2025 04:24 AM | 3dghs | 20/04/2025 04:24 AM | THP | Tetrahydropapaveroline, opioid-like dopamine derivative | N/A | μ-opioid effects, suppression of Tyrosine Hydroxylase (TH), altered mood perception | Upstream: DOPAL + dopamine; Downstream: opioid receptor influence | Formed under ALDH1A1/1A2/2 inhibition, increases under Acetaldehyde burden |
| 14 | 3dghs | 20/04/2025 04:24 AM | 3dghs | 20/04/2025 04:24 AM | GHB | CNS depressant, GABAergic mimic | Anxiety, agitation, hypersensitivity | Sedation, dissociation, altered consciousness | Upstream: SSAL via 4-HBDH; Downstream: GHB receptor, GABA-B | Built up during ALDH5A1 inhibition / low NAD+; depresses respiration and cAMP |
| 15 | 3dghs | 20/04/2025 04:24 AM | 3dghs | 20/04/2025 04:24 AM | Tyramine | Indirect sympathomimetic, displaces norepinephrine | N/A | Headache, hypertension, panic episodes | Upstream: Tyrosine decarboxylation; Downstream: Monoamine Oxidase A (MAO-A) degradation | High in fermented foods; sensitive to Monoamine Oxidase (MAO) inhibitor levels |
| 16 | 3dghs | 20/04/2025 04:24 AM | 3dghs | 21/04/2025 03:08 AM | Autoantibodies (Receptor-Modulating) | Variable; modulates neurotransmitter receptor function | N/A | Receptor overstimulation, desensitisation, or rebound suppression | Targets: dopamine, serotonin, histamine, GABA, others; Modulate signalling dynamics | Typically IgG-based; estimated half-life ~21 days; may enhance or inhibit receptor signalling based on binding site and context. Likely represent an adaptive attempt to restore homeostasis in failing or suppressed pathways. |
Onboarding
The fix isn’t to push harder, it’s to intervene smarter - a staged approach works better.
For severe cases / people with elevated susceptibility to (neuropsychiatric) symptoms from supplements, etc., a very gentle ramp up with tiny doses of non-methylated B vitamins can be very helpful, before moving to the compounded multi-mineral products. Metabolics (UK) produce a range of liquid B vitamins which are ideal for these purposes, although they don't carry all products and some other vendors are required.
You can find these in the "Onboarding (Severe)" category in product lists below.
A schedule of "essential" products and dosing can be found below, in "Getting started".
Use non-oral routes to bypass known bottlenecks. Transdermal, sublingual, or parenteral delivery helps sidestep transporter saturation, liver metabolism, or dysregulated GI environments. Dissolving nutrients in DMSO is another useful strategy.
P5P in DMSO is one example of an advanced strategy - dissolving P5P in a DMSO solution bypasses multiple upstream steps: it does not rely on ALP, avoids compromised membrane transporters, and skips over PK activation. This makes it ideal in states where P5P is known to be low despite B6 repletion. It may also enter intracellular compartments more efficiently, including mitochondria. The same effect applies to most compounds needing to be absorbed and distributed systemically.
In this context, neurotransmitter restoration is more about kinetics, cofactor availability, and redox context. A patient may be taking all the right nutrients, but if those nutrients are stuck upstream, degraded by peroxynitrite, or unable to bind to their target enzymes due to low zinc, the net effect is failure. Worse, poorly timed repletion can destabilise the system further.
The half-life of each vitamin is frequently overlooked. Dosing vitamins 2-4 times per day is often necessary to achieve sufficient benefit and this is reflected in the schedule.
eg. Vitamins B1, B2, B3, B5, B6, B7/H, B8, B9, B12 and C are taken 2-3x/day, often sublingually.
In the context of restoring severe deficiencies, strategic sequencing matters. B vitamins are powerful, especially in active forms, however they also act as signals in a complex control system. If introduced out of order or in isolation, they may trigger compensatory reactions that mimic toxicity, when in fact they are just unmasking hidden dysfunction.
Many of these mechanisms may also help explain why certain neuropsychiatric conditions appear during chronic illness and how they can act as precursor states to systemic collapse.
ADHD, for instance, is often characterised by signs of noradrenaline and dopamine dysregulation, impaired impulse control, and chronic restlessness, traits which may reflect an early-stage compensation for failing neurotransmitter recycling or low-grade redox and metabolic dysfunction, downstream of chronic endogenous acetaldehyde and opioid synthesis. If these compensations begin to fail, especially under stress, infection, or prolonged nutritional depletion downstream of chronic lactic acid metabolism and mineral transporter alterations, the system may tip into a more energy-conserving, downregulated state, as observed in ME/CFS, long COVID, post vaccination syndrome, etc.
Bipolar disorder may reflect a different kind of instability, one in which neurotransmitter tone swings between overcompensation and collapse, and this too may be compounded by aldehyde load, especially acetaldehyde, which inhibits ALDH enzymes responsible for clearing dopamine breakdown products like DOPAL.
Dietary contributions to acetaldehyde burden, such as excessive intake of alcohol, sugar, or fermentable carbohydrates, can further amplify this inhibition by fuelling microbial overgrowth and endogenous ethanol production in the gut. When ALDH function is compromised, neurotoxic intermediates accumulate, further impairing redox balance and downstream dopamine synthesis. Over time, this may shift the system toward an oscillatory or collapsing state, where any attempt to stabilise mood or energy is undermined by bottlenecks in detoxification and neurotransmitter recycling These cycles could, in part, emerge from fluctuating availability of critical cofactors like P5P, B2, or SAMe, or episodic redox crashes that disrupt normal mood-regulating feedback.
However, the protocol also spans over 250 printable pages - so it's also completely understandable if you find yourself feeling a bit overwhelmed by the volume of new information needing to be absorbed.. likely while still battling brain fog and energy envelope issues, chronic feelings of fight/flight and other challenges.
Removing some or all of these debilitating issues should help improve the absorption and retention of new information. The focus of this section is to order and integrate JUST the essential items needed to get started on stabilising the key metabolic pathways. You can integrate them using the order described below, also noted in the daily schedules / run-sheets provided at the end of this section, along with a product ordering spreadsheet.
Ideally after sending off your baseline tests, you may help stabilise critical parts of the metabolism and help avoid unwanted MCAS + other symptoms by;
Notes:
i) Failure to maintain lymphatic flow can result in compartment-specific pressure buildup, eg. intracranial pressure.
ii) For severe patients, this may need to be actioned by carers and/or professionals. Sensitivity to touch may initially prevent performing this necessary step, however it should be actioned as soon as possible.
Notes:
i) Eat strategically to ensure glycogen stores are being appropriately supported - this may easily be >150-180g of net carbohydrates / day, as insulin sensitivity / glycogen synthesis improves - absorbed over 3-6 meals / snacks. Carbohydrate needs reflect (immune) activity levels and other factors. A number of the supplements included below will help glycogen homeostasis.
ii) The initial goal is a low-inflammatory, low-histamine, low-oxalate diet - ideally, one that avoids triggering foods - however this doesn't need to be "perfect", just "good enough". This will later expand to include a wide array of plants, their helpful polyphenols, microbiome nourishing fibres / starches and numerous other useful compounds, whilst accompanying targeted, staged probiotics that focus on butyrate production and epithelial integrity, before repopulating lactobacillus, bifidobacterium, oxalobacter and other helpful species.
4. Stabilise the redox and mineral terrain. This includes VERY SLOWLY introducing :
a) electrolytes (see 4.1 Electrolytes), taken slowly over the day, by making a daily / weekly recipe of
specific electrolytes and amino acids to put in a 500ml drink bottle
and slowly sip / pour a "shot" into a glass, top up with water and drink
between meals (see 4.3 DIY "sipper / shots").
You can start at eg. 1/8 daily doses and slowly increase.
The daily targets for each electrolyte compound used are (these are also listed in the daily schedules at the end of this page). These allow for minimal dietary intakes and can be further adjusted around consistent dietary norms, using this calculator tool:
Magnesium Aspartate - 5.5g total powder (440mg elemental magnesium) / day.
Monocalcium Phosphate - 5g total powder (850mg elemental calcium & 1300mg elemental phosphorous) / day.
Potassium Citrate - 13g total powder (4940mg elemental potassium) / day.
Sodium Bicarbonate - 5g total powder (1350mg elemental sodium & 3650mg bicarbonate) / day.
Sodium Chloride - 5-7g total powder (2730mg elemental sodium & 4270mg chloride) / day.
Resveratrol can be slowly added here (taken separately) 3x/day - initially starting at 50mg and increasing to 500mg per dose, to help protect against additional lactic acid being created by unblocking bottlenecks in glycolysis (correcting phosphate, magnesium, etc) while the TCA cycle is less efficient.
Liberally applying the magnesium gel after showering, can be highly effective for magnesium absorption and is included in the schedule.
Notes:
i) Consuming too much at once may cause diarrhoea, headaches, nausea, water retention and/or rapid urination.
ii) Calcium and to a lesser extent, potassium may temporarily
increase adreneric / glutaminergic sensitivity and need to be increased
more slowly than others. Calcium
sensitivity needs to be tested and managed carefully. Adrenergic, dopaminergic and related auto-antibodies predict sensitivity and delay calcium repletion. Sodium phosphate can be used as an alternate phosphate source during careful calcium titration. (see 4.1 Electrolytes)
iii) Starting magnesium and/or phosphate can improve glucose uptake and glycogen synthesis. Experiencing symptoms that resemble hypoglycaemic events or diabetic "hangry" mood alterations may indicate more dietary carbohydrates are needed.
iv) This recipe can also be combined with eg. green or other tea, lemon juice, lime juice, acai, berry, etc for flavour.
v) Shake before each use.
b) antioxidants and mitochondrial cofactors (Vitamin C, Vitamin E, R-ALA, CoQ10, GSH donors like NAC), taken 2-3x/day.
Notes:
i) These may need TINY doses, initially, eg. 50mg of Vitamin C, NAC and CoQ10. Introduce these individually.
ii) Vitamin E and R-ALA are normally less sensitive. R-ALA may increase insulin sensitivity.
c) (usually less slowly) L-carnitine / acetyl L-carnitine, creatine (for fatty acid transport and ATP-PC pathway), uridine monophosphate (sublingually - ramping up from 10, to typically 50-100mg, 2x/day) and similar slowly ramp up of D-ribose, starting at 500mg, to 10g, added to the daily DIY "sipper/shot" recipe. SLOWLY titrate a morning sublingual dose of inosine from 50-100mg (weeks 1-2 or until ready for an immune activity phase) to 500mg.
Notes:
i) Expect insulin sensitivity and glycogen synthesis to increase with uridine, D-ribose and inosine - be prepared to increase intakes of carbohydrates to facilitate glycogen synthesis and potentially sodium + other electrolytes, towards their daily targets.
ii) Inosine is also an immune stimulant, and may trigger some initial immune activity - keep the dose low, eg. 50-100mg for the first 1-2 weeks, or until metabolically stable enough to sustain a phase of initial immune activity.
d) Adding mineral cofactors like zinc, copper, iron, manganese, selenium, iodine, lithium, rubidium, cobalt, boron, and molybdenum, etc. This helps balance the neurotransmitter synthesis pathway (and precursors), lowers the burden on ALDH and MAO pathways and reduces oxidative stress, allowing safer processing of neurotransmitter metabolites. (see 2.3.2 Remineralisation).
Notes:
i) Many of the minerals require non-standard routes for absorption, eg. sublingual, liposomal, DMSO-carrier.
ii) Remineralisation will be severely limited if acidaemia / acidosis is still present.
e) Introducing vitamins B1 and B2 in active or near-active forms - such as TPP / cocarboxylase and FMN / R5P. These support mitochondrial redox balance, glycolysis, and the Pentose Phosphate Pathway. Depending on the severity of dysbiosis / acetaldehyde burden, the total daily B1 dosing can range from 50-600mg of the active form, cocarboxylase (not to be confused with eg. thiamine or thiamine HCL which would require much higher doses), starting from a low dose.
Notes:
i) Compounded nutrients are available (see 4.2 Compounded nutrients) and replace a wide range of individual supplements. The compounded nutrients are potent, therefore starting at eg. 1/8th doses,
may be helpful to soften / slow the metabolic shift when restoring
severe deficiencies.
ii) B vitamin titration options for patients with severe
neuropsychiatric sensitivity are also discussed.
iii) Additional B1, in any form, can be added for further
acetaldehyde adduct-forming and detoxification support, later - noting the impact of rapid removal of acetaldehyde -> endogenous morphine. (see 2.3.4 Rapid withdrawal, hypo/hypermetabolism)
iv) Adding B1 can increase B9 transporter activity and SAMe availability,
allowing some adrenergic signalling increase unless B2 and NAD+ are
restored in balance - start slowly.
f) Slowly layer in vitamins B5, B6 (as P5P), biotin, D-chiro inositol, B9 and B12 (as methylcobalamin or
hydroxocobalamin) only after upstream redox stress is under better control.
Notes:
i) B1, B9 and B12 can increase methylation -> SAMe availability, unblocking epinephrine synthesis at PNMT and also COMT activity, leading to hyper-adrenergic signalling if TOO MUCH is introduced quickly, ie. without sufficient B2 for MAO and NAD+ (and redox) for ALDH.
ii) In
the context of unresolved aldehyde or monoamine overload, these can also be
disruptive (unless P5P is eg. dissolved in DMSO, bypassing impaired alkaline phosphatase (ALP) and pyridoxal kinase (PK) steps) and BH4 synthesis (dietary queuine - see "Vitamin Q deficiency").
NB. Reducing acetaldehyde and/or restoring NAD+:NADH status corrects a wide array of impaired metabolism, including the pathway issue which promotes endogenous morphine synthesis.
Stay keenly observant for rapid withdrawal symptoms and manage them proactively.
Then;
g) Introducing NAD+ pool support (apigenin - P38
inhibitor), NAD+:NADH redox support (0.05-0.3mg of methylene blue, once per day), and
Notes:
i) Start at 0.05mg (50mcg) of methylene blue per day and slowly increase every 2-3 days until ANY metabolic shift is observed. Hold at that dose and look to decrease towards 50mcg, when appropriate.
ii) "MORE IS NOT MORE." THE MITOCHONDRIAL SUPPORTING EFFECT OF METHYLENE BLUE IS LOST AT HIGHER DOSE RANGES.
iii) Expect and watch for alcohol / opioid withdrawal symptoms. Manage them proactively.
h) Adding active vitamin B3, as sublingual NAD+ / NADH (NOT precursors - niacin, nicotinamide / niacinamide, nicotinamide riboside / mononucleotide) at 5-10mg doses, 2x/day and increase to 20-40mg 2x/day.
Notes:
i) Expect and watch for alcohol / opioid withdrawal symptoms. Manage them proactively. (see 2.3.4 Rapid withdrawal, hypo / hyper metabolism)
6. Start working on identifying and addressing any/all other influences affecting histamine and/or sympathetic overdrive (see 2.2.6 Cortisol, limbic system, glycogen and IFN-γ).
Notes:
i) Unrestricted, deep nasal breathing without localised inflammation is a basic requirement for parasympathetic signalling (see also 2.2.3 Living without chronic dysbiosis - Nasopharynx).
"Starter" daily schedule / run-sheet
Once you have sufficiently stabilised, you can continue onboarding and progressing through Stages 1, 2 and 3. The daily schedule options for the full protocol can be found in 2.3 Daily supplement schedule.
However, to keep things more manageable for now - you can also download and print a simpler / more focused daily "starter" schedule / run-sheet - and there are two versions available:
You can choose this version (opens on a new page) if you intend on using the compounded nutrients,
OR
you can choose this version (opens on a new page) if you intend on using separate store-bought supplements.
"Starter" product ordering links
If you are already committed to completing the whole protocol, the product ordering links for the primary pathway of the full protocol can be found in 5 Ordering products. However, you can also download a time-and-money saving spreadsheet of the starter items ONLY, before committing to the whole process:
For starter product ordering, you can simply choose your shipping region from the drop-down box and click on the Excel or CSV icon to download a spreadsheet of some starter items, with product ordering links and relevant information for preparation of time/effort-saving weekly recipes. This particular table is too complex to fit onto a webpage and easily manipulate, however works well in eg. Excel or Google Sheets, etc.
| wdt_ID | wdt_created_by | wdt_created_at | wdt_last_edited_by | wdt_last_edited_at | purpose | category | product | weekly recipe amount | stage2diy | stage3diy | weekly recipe notes | in custom nutrients | isdiypowder | isdiydrink | isothersupplement | isstarteritem | issevereitem | getting started desc | forwdtid | sortorder | region | producttype | isantiseptic | istool | per 90 days | product link | rationale for inclusion | more information |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 19/08/2024 05:01 AM | [DIY SHAKE] | Vitamins | B8 Myo & D-Chiro Inositol | 3 caps | 3 caps | 3 caps | For AU source, 1.5g = 3 caps. DE source has 20% more per cap. | 1 | 1 | Start with a target dose around 2.5mg D-chiro inositol (approx 1/4 capsule) and increase. | 2 | US | Vitamins | 1 | https://iherb.com/pr/wholesome-story-myo-d-chiro-inositol-120-vegetarian-capsules/114887 | Myo-inositol + D-chiro inositol. Glucose uptake and glycogen synthesis. | https://bornfree.life/learn/4-3-diy-powder | |||||||
| 2 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 25/09/2024 06:18 AM | [DIY SHAKE] | Vitamins | B5 Pantothenic Acid | 0.7-3.5g | 0.7-3.5g | 0.7-3.5g | 1 | 1 | Normally well-tolerated | 3 | US | Vitamins | 9g-45g | https://www.bulksupplements.com/products/vitamin-b5-calcium-pantothenate-pantothenic-acid-powder?variant=32133465342063 | Required for coenzyme A (CoA) and helps regulate lipolysis at VNN1. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 4 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [DIY SHAKE] | Supplements | PQQ+CoQ10 | 7 - 21 caps | 7 - 21 caps | 7 - 21 caps | 1 | 1 | Normally well-tolerated. Amount needed depends on mineral deficiency data / dose response | 5 | US | Supplements | 3–9 | https://iherb.com/pr/lake-avenue-nutrition-coq10-with-pqq-100-mg-60-veggie-capsules/97389 | DBH promoter, Electron Transport Chain support. CoQ10 can promote fungal growth. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 5 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [DIY SHAKE] | Supplements | Apigenin | 7 - 56 caps | 7 - 56 caps | 7 - 56 caps | 1 | 1 | Normally well tolerated. Amount required depends on mineral deficiency data and dose response | 6 | US | Supplements | 1–8 | https://iherb.com/pr/codeage-liposomal-apigenin-non-gmo-vegan-90-capsules/114120 | ALDH, p38 MAPK inhibitor, TGF-b1 modulator and NADase inhibitor. Start at ¼ dose and increase. Upper threshold for effective dose may be 400mg/day. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 7 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 23/11/2025 05:59 AM | [DIY SHAKE] | Minerals | Kelp | 7g | 7g | 7g | 1 | 1 | Target daily dose 1g. Start slowly and increase to daily values, as tolerated | 9 | US | Minerals | 90g | https://iherb.com/pr/now-foods-organic-kelp-pure-powder-8-oz-227-g/16668 | Bromine and iodine source. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 11 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 17/11/2025 02:55 AM | [DIY SIPPER/SHOTS] | Electrolytes | Monocalcium Phosphate | 35g | 35g | 35g | 5g / day | 1 | 1 | 1 | 5g / day. Correcting calcium deficiency can unblock adrenergic signallng bottlenecks and expose temporary receptor hypersensitivity. Substitute for monosodium phosphate + alternate calcium for very slow calcium titration | 14 | US | Electrolytes | 450g | https://rhbulk.com/products/monocalcium-phosphate-anhydrous-v-90 | Calcium - critical electrolyte. Oral dosing works but can feed biofilms. Phosphate - critical electrolyte for energy metabolism (e.g. P5P, glycolysis, etc). Oral dosing is “okay”. Low phosphorus may indicate acidemia - add bicarb. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 12 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 11/09/2024 07:23 AM | [DIY SIPPER/SHOTS] | Electrolytes | Magnesium Aspartate | 38.5g | 38.5g | 38.5g | 5.5g / day | 1 | 1 | 1 | 5.5g / day | 15 | US | Electrolytes | 500g | https://www.bulksupplements.com/products/magnesium-aspartate-powder?variant=32133428117615 | Critical electrolyte for energy metabolism, etc. Low magnesium can also cause arrhythmia, muscle spasms. Aspartate assists with urea cycle and energy metabolism. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 13 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 11/08/2024 11:29 AM | [DIY SIPPER/SHOTS] | Electrolytes | Potassium Citrate | 91g | 91g | 91g | 13g / day | 1 | 1 | 1 | 13g / day. Correcting potassium deficiency can unblock adrenergic signallng bottlenecks and expose temporary receptor hypersensitivity. Start slowly | 16 | US | Electrolytes | 900g | https://www.bulksupplements.com/products/potassium-citrate-powder | Critical electrolyte. Oral dosing is okay. Low potassium can cause high blood pressure, arrhythmia, muscle spasms, low glutamate and dopamine synthesis, impaired glycolysis. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 14 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [DIY SIPPER/SHOTS] | Amino Acids | Taurine | 84g | 84g | 84g | 12g / day. Can be taken sublingually if sulphur reducing bacteria suspected. Start low / find tolerable dose and increase. | 1 | 1 | 1 | 12g / day. Can be used sublingually, if gut microbiome dysbiosis is severe. Start low / find tolerable dose and increase | 17 | US | Amino Acids | 1.08kg | https://www.bulksupplements.com/products/taurine | GLUT2, glycogen synthesis, promotes ALDH for aldehyde degradation, adrenaline inhibition. TUDCA synthesis. Note: can feed Bilophila wadsworthia, etc. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 15 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 18/03/2026 09:00 AM | [DIY SIPPER/SHOTS] | Amino Acids | Acetyl L-Carnitine | 28g | 28g | 28g | 4g / day. Can be used sublingually, if gut microbiome dysbiosis is severe. | 1 | 1 | 1 | 4g / day. Can be used sublingually, if gut microbiome dysbiosis is severe. | 18 | US | Amino Acids | 360g | https://www.bulksupplements.com/products/l-carnitine-base-powder?variant=32133418188911 | Fatty acid transport, dopamine synthesis promoter. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 21 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [DIY SIPPER/SHOTS] | Amino Acids | Creatine | 35g | 35g | 35g | 5g / day | 1 | 1 | 1 | 5g / day | 24 | US | Amino Acids | 450g | https://www.bulksupplements.com/products/creatine-monohydrate | GLUT4, ATP, SAMe metabolism efficiency. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 23 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [DIY SHAKE] | Minerals | Bamboo (Silica) | 14g | 14g | 14g | 1 | 1 | Start slowly and increase to protocol doses, as tolerated | 26 | US | Minerals | 180g | https://www.bulksupplements.com/products/bamboo-extract-powder | Silicon deficiency – HIF-1a. Antiviral. Magnesium uptake. Collagen. Silica will also be heavily used to excrete acetaldehyde and toxic metals. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 25 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 13/09/2024 06:44 AM | [DIY SHAKE] | Supplements | R-ALA | 4.2g | 4.2g | 4.2g | 1 | 1 | Start slowly - can break biofilm and trigger some herxheimer reactions. | 28 | US | Supplements | 50.4g | https://www.bulksupplements.com/products/r-alpha-lipoic-acid-r-ala-powder | ALDH2 promoter. AMPK promoter – insulin sensitivity. Biofilm breaker. Toxic metal chelator. TCA cycle support.. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 26 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [DIY SIPPER/SHOTS] | Supplements | NAC | 3.5-7g | 3.5-7g | 21g | 0.5-1g / day. In Stage 3, cycle an increased dose of 3g / day for 3 weeks, then revert for 3 weeks, indefinitely. | 1 | 1 | 1 | 0.5-1g / day. Start slowly | 29 | US | Amino Acids | 97.5–132g | https://www.bulksupplements.com/products/n-acetyl-l-cysteine-nac | Thrombolytic, mucolytic, antioxidant, detoxifier, biofilm breaker and metal chelator. Can cause die-off in large doses. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 33 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 11/08/2024 11:30 AM | [DIY SIPPER/SHOTS] | Electrolytes | Sodium Chloride | 35-50g | 35-50g | 35-50g | 5-7.1g/day | 1 | 1 | 1 | 5-7g / day | 37 | US | Electrolytes | 450-900g | https://www.amazon.com/Amazon-Brand-Happy-Ground-Ounces/dp/B07QW1G8MW | Critical electrolyte. Oral dosing is okay. Low sodium can cause low blood pressure and low dopamine transport. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 37 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 12/03/2026 10:58 AM | [REPLETION] | Vitamins | B1 Thiamine | 1 | 1 | (Also found in the compounded minerals) Equivalent to 1-2 x 500mg Thiamine HCL or more, 2x/day | 44 | US | Vitamins | 3 | https://iherb.com/pr/source-naturals-high-potency-b-1-500-mg-100-tablets/980 | TPP / energy metabolism, affected by acetaldehyde. Increase from a tenth dose. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 38 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 17/09/2024 02:08 AM | [REPLETION] | Vitamins | B9 5-MTHF | 1 | 1 | Start very slowly - may unblock methylation -> SAMe -> epinephrine synthesis and only parts of the degradation pathway, if taken in isolation. | 45 | US | Vitamins | 1 | https://iherb.com/pr/life-extension-optimized-folate-1-700-mcg-dfe-100-vegetarian-tablets/63828 | Methylation cycle, BH4. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 41 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 29/09/2024 04:42 AM | [DIY SHAKE] | Vitamins | C Ascorbate | 14g | 14g | 14g | 1 | 1 | Start slowly and increase. Can be a bumpy start | 48 | US | Vitamins | 1 | https://iherb.com/pr/california-gold-nutrition-gold-c-usp-grade-vitamin-c-1-000-mg-240-veggie-capsules/61865 | Antioxidant. HIF-1a, DBH, collagen synthesis. Use away from copper dosing. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 49 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 11/08/2024 11:35 AM | [OTHER SUPPLEMENTS] | Electrolytes | Magnesium Spray | 1 | 1 | Apply after showering | 56 | US | Electrolytes | 4 | https://iherb.com/pr/life-flo-magnesium-oil-sport-spray-8-fl-oz-237-ml/49247 | Critical electrolyte for energy metabolism, etc. Low magnesium can also cause arrhythmia, muscle spasms. Transdermal absorption provides a slow release profile. | https://bornfree.life/learn/4-1-electrolytes/ | |||||||||||
| 50 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 12/09/2024 02:12 AM | [REPLETION] | Minerals | Vanadium | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 57 | US | Minerals | 1 | https://iherb.com/pr/source-naturals-vanadyl-sulfate-10-mg-100-tablets/1477 | (Sublingual) Required for glucose transport and insulin sensitivity. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 51 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [REPLETION] | Minerals | Lithium | 1 | 1 | Start slowly and increase to protocol doses, as tolerated | 58 | US | Minerals | 1 | https://iherb.com/pr/kal-lithium-orotate-5-mg-120-vegcaps/85528 | Adrenergic metabolism / inhibition. Glycogen‑Synthase‑Kinase‑3β inhibition.. Magnesium reabsorption. Immunity. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 52 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [REPLETION] | Minerals | Molybdenum | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 59 | US | Minerals | 1 | https://iherb.com/pr/source-naturals-reduced-glutathione-complex-orange-50-mg-100-lozenges/1407 | (Sublingual) RIboflavin metabolism. B6 degradation. Taurine metabolism. ALDH. XO. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 53 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [REPLETION] | Minerals | Selenium | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 60 | US | Minerals | 1 | https://iherb.com/pr/california-gold-nutrition-selenium-yeast-free-200-mcg-180-veggie-capsules/90416 | (Sublingual) Thyroid and glutathione metabolism. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 54 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 12/03/2026 11:30 PM | [REPLETION] | Minerals | Chromium | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 61 | US | Minerals | 1 | https://iherb.com/pr/solaray-chromium-picolinate-lozenges-natural-lemon-raspberry-1-000-mcg-100-lozenges/124399 | (Sublingual) Required for glucose transport and insulin sensitivity. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 55 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [REPLETION] | Minerals | Sulphur | 1 | 1 | Start slowly and increase to protocol doses, as tolerated | 62 | US | Minerals | 3 | https://iherb.com/pr/doctor-s-best-msm-with-optimsm-1-500-mg-120-tablets/3 | Iron-sulphur clusters. Oxalate transport. Transsulfuration pathway | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 56 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [REPLETION] | Minerals | Zinc | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 63 | US | Minerals | 3 | https://iherb.com/pr/source-naturals-wellness-zinc-lozenges-peach-raspberry-23-mg-120-lozenges/1476 | (Sublingual) Catabolic pathways. Glycolysis. HIF-1a. Methylation + folate transport. BH4. ALDH. LDH. NOS. RK. P5P. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 57 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [REPLETION] | Minerals | Copper | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 64 | US | Minerals | 2 | https://iherb.com/pr/solaray-copper-2-mg-100-vegcaps/70102 | (Sublingual) Dopamine precursors. Dopamine beta hydroxylase. CuZnSOD. Glycolysis. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 58 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 27/08/2024 05:26 AM | [REPLETION] | Vitamins | B7 Biotin | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 65 | US | Vitamins | 1 | https://iherb.com/pr/solaray-biotin-natural-orange-1-000-mcg-100-lozenges/123883 | (Sublingual) Required for normal energy metabolism, however will feed fungal infections and promote fungal bloom, if infections are not sufficiently inhibited / managed. Oral dosing fails in alcoholism. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 59 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 19/08/2024 05:02 AM | [REPLETION] | Vitamins | B6 P5P | 1 | 1 | (Sublingual, also found in the compounded minerals) Generally well tolerated | 66 | US | Vitamins | 1 | https://iherb.com/pr/swanson-p-5-p-pyridoxal-5-phosphate-20-mg-60-capsules/117697 | Problematic when ALDH deficiency exists, but a critical coenzyme for metabolism. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 65 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 12/03/2026 10:55 AM | [REPLETION] | Minerals | Manganese | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 74 | US | Minerals | 1 | https://iherb.com/pr/bodybio-liquid-mineral-manganese-2-fl-oz-59-ml/150520 | (Sublingual) 2 drops. Supports MnSOD. Folate metabolism. Glycocalyx. GDH. Gluconeogenesis (PCB. ME1. PLD). | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 66 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 04/03/2026 01:18 AM | [REPLETION] | Vitamins | B2 FMN Riboflavin | 1 | 1 | (Sublingual, also found in the compounded minerals) 25mg, 3x/day | 75 | US | Vitamins | 7g | https://prescribedforlife.com/products/riboflavin-5-phosphate-riboflavin-5-phosphate-sodium-powder-html | (Sublingual) Absorbable FMN and FAD support. Has antimicrobial functions. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 67 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 29/11/2025 04:11 AM | [REPLETION] | Vitamins | B3 NAD+/H | 1 | 1 | (Sublingual) 5-40mg, 2x/day | 76 | US | Vitamins | 7.2g | https://www.bulksupplements.com/products/nad-supplement | (Sublingual) NAD+:NADH pool support for wide array of metabolic pathways. IFN-γ activity. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 68 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 19/08/2024 05:14 AM | [REPLETION] | Vitamins | B12 Cobalamin | Sublingual | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to 1-2mg, as tolerated | 77 | US | Vitamins | 1 | https://vimergy.com/products/organic-b12 | (Sublingual) Methylation. Antioxidant. Catabolic pathways -> TCA cycle. | https://bornfree.life/learn/2-3-2-remineralisation/ | ||||||||||
| 75 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 07/01/2026 10:04 PM | [REPLETION] | Minerals | Cobalt | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 84 | US | Minerals | 1 | https://www.amazon.com/dp/B0DPNDVKFR | (Sublingual) EPO regulation. Iron homeostasis. B12 synthesis (microbial). FAD synthesis, P5P synthesis | ||||||||||||
| 76 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [REPLETION] | Minerals | Germanium GE-132 | 1 | 1 | Start slowly and increase to daily values, as tolerated | 85 | US | Minerals | 2 | https://www.nutricology.com/organo-germanium-50-vegetarian-capsules | Antioxidant and other functions. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 90 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 11/08/2024 11:28 AM | [TOOLS] | Tools | Empty Bottles | 1 | 99 | US | Antiseptic | 1 | 1 | https://www.amazon.com/PrettyCare-Measured-Pipettes-Tincture-Essential/dp/B07RK5SFYH | Required for temporary storage and dosing of various recipes. | https://bornfree.life/learn/2-2-3-living-without-chronic-dysbiosis/#DIY-antiseptic | ||||||||||||
| 92 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 11/08/2024 11:30 AM | [TOOLS] | Tools | Milligram Scales | 1 | 102 | US | Tools | 1 | https://www.amazon.com/dp/B07TBJBFRK | For measuring small quantities of supplements. | ||||||||||||||
| 93 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 12/03/2026 12:08 PM | [TOOLS] | Tools | Measuring Spoons | 1 | 103 | US | Tools | 1 | https://www.amazon.com/dp/B0D5LH3K1H | For quickly measuring small quantities supplements. | ||||||||||||||
| 99 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [DIY SHAKE] | Minerals | Bamboo (Silica) | 14g | 14g | 14g | 1 | 1 | Start slowly and increase to protocol doses, as tolerated | 26 | ALT | Minerals | 9 | https://iherb.com/pr/solaray-bamboo-vital-extract-600-mg-60-vegcaps/24423 | Silicon deficiency – HIF-1a. Antiviral. Magnesium uptake. Collagen. Silica will also be heavily used to excrete acetaldehyde and toxic metals. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 101 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 13/09/2024 06:45 AM | [DIY SHAKE] | Supplements | R-ALA | 4.2g | 4.2g | 4.2g | 1 | 1 | Start slowly - can break biofilm and trigger some herxheimer reactions. | 28 | ALT | Supplements | 3 | https://iherb.com/pr/allmax-r-ala-60-capsules/67927 | ALDH2 promoter. AMPK promoter – insulin sensitivity. Biofilm breaker. Toxic metal chelator. TCA cycle support.. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 107 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 12/03/2026 10:57 AM | [REPLETION] | Vitamins | B1 Thiamine | 1 | 1 | (Also found in the compounded minerals) Equivalent to 1-2 x 500mg Thiamine HCL or more, 2x/day | 44 | ALT | Vitamins | 3 | https://iherb.com/pr/source-naturals-coenzymated-b-1-60-lozenges/1077 | TPP / energy metabolism, affected by acetaldehyde. Increase from a tenth dose. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 108 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 11/08/2024 11:35 AM | [OTHER SUPPLEMENTS] | Electrolytes | Magnesium Spray | 1 | 1 | Apply after showering | 56 | ALT | Electrolytes | 4 | https://goodstate.com/collections/ionic-magnesium/products/good-state-ionic-magnesium-oil-professional-grade-8-oz | Critical electrolyte for energy metabolism, etc. Low magnesium can also cause arrhythmia, muscle spasms. Transdermal absorption provides a slow release profile. | https://bornfree.life/learn/4-1-electrolytes/ | |||||||||||
| 138 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 12/03/2026 11:59 AM | [DIY SHAKE] | Vitamins | B8 Myo & D-Chiro Inositol | 3 caps | 3 caps | 3 caps | For AU source, 1.5g = 3 caps. DE source has 20% more per cap. | 1 | 1 | Start with a target dose around 2.5mg D-chiro inositol (approx 1/4 capsule) and increase. | 2 | EU | Vitamins | 1 | https://www.amazon.de/dp/B09SBSWCQ6/ | Myo-inositol + D-chiro inositol. Glucose uptake and glycogen synthesis. | https://bornfree.life/learn/4-3-diy-powder | |||||||
| 139 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 25/09/2024 06:19 AM | [DIY SHAKE] | Vitamins | B5 Pantothenic Acid | 0.7-3.5g | 0.7-3.5g | 0.7-3.5g | 1 | 1 | Normally well-tolerated | 3 | EU | Vitamins | 9g-45g | https://www.bulksupplements.com/products/vitamin-b5-calcium-pantothenate-pantothenic-acid-powder?variant=32133465342063 | Required for coenzyme A (CoA) and helps regulate lipolysis at VNN1. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 141 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [DIY SHAKE] | Supplements | PQQ+CoQ10 | 7 - 21 caps | 7 - 21 caps | 7 - 21 caps | 1 | 1 | Normally well-tolerated. Amount needed depends on mineral deficiency data / dose response | 5 | EU | Supplements | 3–9 | https://www.sunday.de/en/polyphenol-21-komplex.html | DBH promoter, Electron Transport Chain support. CoQ10 can promote fungal growth. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 142 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [DIY SHAKE] | Supplements | Apigenin | 7 - 56 caps | 7 - 56 caps | 7 - 56 caps | 1 | 1 | Normally well tolerated. Amount required depends on mineral deficiency data and dose response | 6 | EU | Supplements | 1–8 | https://iherb.com/pr/codeage-liposomal-apigenin-non-gmo-vegan-90-capsules/114120 | ALDH, p38 MAPK inhibitor, TGF-b1 modulator and NADase inhibitor. Start at ¼ dose and increase. Upper threshold for effective dose may be 400mg/day. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 144 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 11/09/2024 06:37 AM | [DIY SHAKE] | Minerals | Kelp | 7g | 7g | 7g | 1 | 1 | Target daily dose 1g. Start slowly and increase to daily values, as tolerated | 9 | EU | Minerals | 90g | https://www.amazon.de/dp/B07JGZDRBQ/ | Bromine and iodine source. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 148 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 17/11/2025 02:56 AM | [DIY SIPPER/SHOTS] | Electrolytes | Monocalcium Phosphate | 35g | 35g | 35g | 5g / day | 1 | 1 | 1 | 5g / day. Correcting calcium deficiency can unblock adrenergic signallng bottlenecks and expose temporary receptor hypersensitivity. Substitute for monosodium phosphate + alternate calcium for very slow calcium titration | 14 | EU | Electrolytes | 450g | https://www.ebay.de/itm/166972586329 | Calcium - critical electrolyte. Oral dosing works but can feed biofilms. Phosphate - critical electrolyte for energy metabolism (e.g. P5P, glycolysis, etc). Oral dosing is “okay”. Low phosphorus may indicate acidemia - add bicarb. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 149 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 18/09/2024 01:15 PM | [DIY SIPPER/SHOTS] | Electrolytes | Magnesium Aspartate | 38.5g | 38.5g | 38.5g | 5.5g / day | 1 | 1 | 1 | 5.5g / day | 15 | EU | Electrolytes | 500g | https://www.bulksupplements.com/products/magnesium-aspartate-powder?country=AT | Critical electrolyte for energy metabolism, etc. Low magnesium can also cause arrhythmia, muscle spasms. Aspartate assists with urea cycle and energy metabolism. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 150 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 11/08/2024 11:29 AM | [DIY SIPPER/SHOTS] | Electrolytes | Potassium Citrate | 91g | 91g | 91g | 13g / day | 1 | 1 | 1 | 13g / day. Correcting potassium deficiency can unblock adrenergic signallng bottlenecks and expose temporary receptor hypersensitivity. Start slowly | 16 | EU | Electrolytes | 900g | https://www.bulksupplements.com/products/potassium-citrate-powder | Critical electrolyte. Oral dosing is okay. Low potassium can cause high blood pressure, arrhythmia, muscle spasms, low glutamate and dopamine synthesis, impaired glycolysis. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 151 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [DIY SIPPER/SHOTS] | Amino Acids | Taurine | 84g | 84g | 84g | 12g / day. Can be taken sublingually if sulphur reducing bacteria suspected. Start low / find tolerable dose and increase. | 1 | 1 | 1 | 12g / day. Can be used sublingually, if gut microbiome dysbiosis is severe. Start low / find tolerable dose and increase | 17 | EU | Amino Acids | 1.08kg | https://www.bulksupplements.com/products/taurine | GLUT2, glycogen synthesis, promotes ALDH for aldehyde degradation, adrenaline inhibition. TUDCA synthesis. Note: can feed Bilophila wadsworthia, etc. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 152 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 18/03/2026 09:00 AM | [DIY SIPPER/SHOTS] | Amino Acids | Acetyl L-Carnitine | 28g | 28g | 28g | 4g / day. Can be used sublingually, if gut microbiome dysbiosis is severe. | 1 | 1 | 1 | 4g / day. Can be used sublingually, if gut microbiome dysbiosis is severe. | 18 | EU | Amino Acids | 360g | https://www.bulksupplements.com/products/l-carnitine-base-powder?variant=32133418188911 | Fatty acid transport, dopamine synthesis promoter. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 158 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [DIY SIPPER/SHOTS] | Amino Acids | Creatine | 35g | 35g | 35g | 5g / day | 1 | 1 | 1 | 5g / day | 24 | EU | Amino Acids | 450g | https://www.bulksupplements.com/products/creatine-monohydrate | GLUT4, ATP, SAMe metabolism efficiency. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 160 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [DIY SHAKE] | Minerals | Bamboo (Silica) | 14g | 14g | 14g | 1 | 1 | Start slowly and increase to protocol doses, as tolerated | 26 | EU | Minerals | 180g | https://www.bulksupplements.com/products/bamboo-extract-powder | Silicon deficiency – HIF-1a. Antiviral. Magnesium uptake. Collagen. Silica will also be heavily used to excrete acetaldehyde and toxic metals. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 162 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 13/09/2024 06:44 AM | [DIY SHAKE] | Supplements | R-ALA | 4.2g | 4.2g | 4.2g | 1 | 1 | Start slowly - can break biofilm and trigger some herxheimer reactions. | 28 | EU | Supplements | 50.4g | https://www.bulksupplements.com/products/r-alpha-lipoic-acid-r-ala-powder | ALDH2 promoter. AMPK promoter – insulin sensitivity. Biofilm breaker. Toxic metal chelator. TCA cycle support.. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 163 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [DIY SIPPER/SHOTS] | Supplements | NAC | 3.5-7g | 3.5-7g | 21g | 0.5-1g / day. In Stage 3, cycle an increased dose of 3g / day for 3 weeks, then revert for 3 weeks, indefinitely. | 1 | 1 | 1 | 0.5-1g / day. Start slowly | 29 | EU | Amino Acids | 97.5–132g | https://www.amazon.de/N-Acetyl-L-Cysteine-Powder-Sulphur-Containing-Fermentation-Additives/dp/B07D3722WS | Thrombolytic, mucolytic, antioxidant, detoxifier, biofilm breaker and metal chelator. Can cause die-off in large doses. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 170 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 11/08/2024 11:30 AM | [DIY SIPPER/SHOTS] | Electrolytes | Sodium Chloride | 35-50g | 35-50g | 35-50g | 5-7.1g/day | 1 | 1 | 1 | 5-7g / day | 37 | EU | Electrolytes | 450-900g | https://www.amazon.de/-/en/dp/B07PBJG722 | Critical electrolyte. Oral dosing is okay. Low sodium can cause low blood pressure and low dopamine transport. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 174 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 12/03/2026 10:58 AM | [REPLETION] | Vitamins | B1 Thiamine | 1 | 1 | (Also found in the compounded minerals) Equivalent to 1-2 x 500mg Thiamine HCL or more, 2x/day | 44 | EU | Vitamins | 3 | https://iherb.com/pr/source-naturals-high-potency-b-1-500-mg-100-tablets/980 | TPP / energy metabolism, affected by acetaldehyde. Increase from a tenth dose. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 175 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 17/09/2024 02:08 AM | [REPLETION] | Vitamins | B9 5-MTHF | 1 | 1 | Start very slowly - may unblock methylation -> SAMe -> epinephrine synthesis and only parts of the degradation pathway, if taken in isolation. | 45 | EU | Vitamins | 1 | https://iherb.com/pr/life-extension-optimized-folate-1-700-mcg-dfe-100-vegetarian-tablets/63828 | Methylation cycle, BH4. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 178 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 29/09/2024 04:42 AM | [DIY SHAKE] | Vitamins | C Ascorbate | 14g | 14g | 14g | 1 | 1 | Start slowly and increase. Can be a bumpy start | 48 | EU | Vitamins | 1 | https://iherb.com/pr/california-gold-nutrition-gold-c-usp-grade-vitamin-c-1-000-mg-240-veggie-capsules/61865 | Antioxidant. HIF-1a, DBH, collagen synthesis. Use away from copper dosing. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 186 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 11/08/2024 11:35 AM | [OTHER SUPPLEMENTS] | Electrolytes | Magnesium Spray | 1 | 1 | Apply after showering | 56 | EU | Electrolytes | 4 | https://iherb.com/pr/life-flo-magnesium-oil-sport-spray-8-fl-oz-237-ml/49247 | Critical electrolyte for energy metabolism, etc. Low magnesium can also cause arrhythmia, muscle spasms. Transdermal absorption provides a slow release profile. | https://bornfree.life/learn/4-1-electrolytes/ | |||||||||||
| 187 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 12/09/2024 02:12 AM | [REPLETION] | Minerals | Vanadium | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 57 | EU | Minerals | 1 | https://iherb.com/pr/source-naturals-vanadyl-sulfate-10-mg-100-tablets/1477 | (Sublingual) Required for glucose transport and insulin sensitivity. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 188 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [REPLETION] | Minerals | Lithium | 1 | 1 | Start slowly and increase to protocol doses, as tolerated | 58 | EU | Minerals | 1 | https://iherb.com/pr/kal-lithium-orotate-5-mg-120-vegcaps/85528 | Adrenergic metabolism / inhibition. Glycogen‑Synthase‑Kinase‑3β inhibition.. Magnesium reabsorption. Immunity. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 189 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [REPLETION] | Minerals | Molybdenum | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 59 | EU | Minerals | 1 | https://iherb.com/pr/source-naturals-reduced-glutathione-complex-orange-50-mg-100-lozenges/1407 | (Sublingual) RIboflavin metabolism. B6 degradation. Taurine metabolism. ALDH. XO. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 190 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [REPLETION] | Minerals | Selenium | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 60 | EU | Minerals | 1 | https://iherb.com/pr/california-gold-nutrition-selenium-yeast-free-200-mcg-180-veggie-capsules/90416 | (Sublingual) Thyroid and glutathione metabolism. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 191 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 12/03/2026 11:30 PM | [REPLETION] | Minerals | Chromium | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 61 | EU | Minerals | 1 | https://iherb.com/pr/solaray-chromium-picolinate-lozenges-natural-lemon-raspberry-1-000-mcg-100-lozenges/124399 | (Sublingual) Required for glucose transport and insulin sensitivity. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 192 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [REPLETION] | Minerals | Sulphur | 1 | 1 | Start slowly and increase to protocol doses, as tolerated | 62 | EU | Minerals | 3 | https://iherb.com/pr/doctor-s-best-msm-with-optimsm-1-500-mg-120-tablets/3 | Iron-sulphur clusters. Oxalate transport. Transsulfuration pathway | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 193 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [REPLETION] | Minerals | Zinc | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 63 | EU | Minerals | 3 | https://iherb.com/pr/source-naturals-wellness-zinc-lozenges-peach-raspberry-23-mg-120-lozenges/1476 | (Sublingual) Catabolic pathways. Glycolysis. HIF-1a. Methylation + folate transport. BH4. ALDH. LDH. NOS. RK. P5P. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 194 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [REPLETION] | Minerals | Copper | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 64 | EU | Minerals | 2 | https://iherb.com/pr/solaray-copper-2-mg-100-vegcaps/70102 | (Sublingual) Dopamine precursors. Dopamine beta hydroxylase. CuZnSOD. Glycolysis. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 195 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 27/08/2024 05:26 AM | [REPLETION] | Vitamins | B7 Biotin | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 65 | EU | Vitamins | 1 | https://iherb.com/pr/solaray-biotin-natural-orange-1-000-mcg-100-lozenges/123883 | (Sublingual) Required for normal energy metabolism, however will feed fungal infections and promote fungal bloom, if infections are not sufficiently inhibited / managed. Oral dosing fails in alcoholism. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 196 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 19/08/2024 05:03 AM | [REPLETION] | Vitamins | B6 P5P | 1 | 1 | (Sublingual, also found in the compounded minerals) Generally well tolerated | 66 | EU | Vitamins | 1 | https://iherb.com/pr/swanson-p-5-p-pyridoxal-5-phosphate-20-mg-60-capsules/117697 | Problematic when ALDH deficiency exists, but a critical coenzyme for metabolism. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 202 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 12/03/2026 10:53 AM | [REPLETION] | Minerals | Manganese | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 74 | EU | Minerals | 1 | https://iherb.com/pr/bodybio-liquid-mineral-manganese-2-fl-oz-59-ml/150520 | (Sublingual) 2 drops. Supports MnSOD. Folate metabolism. Glycocalyx. GDH. Gluconeogenesis (PCB. ME1. PLD). | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 203 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 04/03/2026 01:18 AM | [REPLETION] | Vitamins | B2 FMN Riboflavin | 1 | 1 | (Sublingual, also found in the compounded minerals) 25mg, 3x/day | 75 | EU | Vitamins | 7g | https://prescribedforlife.com/products/riboflavin-5-phosphate-riboflavin-5-phosphate-sodium-powder-html | (Sublingual) Absorbable FMN and FAD support. Has antimicrobial functions. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 204 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 29/11/2025 04:11 AM | [REPLETION] | Vitamins | B3 NAD+/H | 1 | 1 | (Sublingual) 5-40mg, 2x/day | 76 | EU | Vitamins | 7.2g | https://www.bulksupplements.com/products/nad-supplement | (Sublingual) NAD+:NADH pool support for wide array of metabolic pathways. IFN-γ activity. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 205 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 19/08/2024 05:14 AM | [REPLETION] | Vitamins | B12 Cobalamin | Sublingual | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to 1-2mg, as tolerated | 77 | EU | Vitamins | 1 | https://vimergy.com/products/organic-b12 | (Sublingual) Methylation. Antioxidant. Catabolic pathways -> TCA cycle. | https://bornfree.life/learn/2-3-2-remineralisation/ | ||||||||||
| 212 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 07/01/2026 10:04 PM | [REPLETION] | Minerals | Cobalt | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 84 | EU | Minerals | 1 | https://www.biolaboratorium.com/products/kobalt-acetat-4hydrat-czda-100g | (Sublingual) EPO regulation. Iron homeostasis. B12 synthesis (microbial). FAD synthesis, P5P synthesis | ||||||||||||
| 213 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [REPLETION] | Minerals | Germanium GE-132 | 1 | 1 | Start slowly and increase to daily values, as tolerated | 85 | EU | Minerals | 2 | https://www.nutricology.com/organo-germanium-50-vegetarian-capsules | Antioxidant and other functions. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 227 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 11/08/2024 11:28 AM | [TOOLS] | Tools | Empty Bottles | 1 | 99 | EU | Antiseptic | 1 | 1 | https://www.amazon.de/HandsUnity-Pipette-Bottle-Small-Glass/dp/B094DFK7F5 | Required for temporary storage and dosing of various recipes. | https://bornfree.life/learn/2-2-3-living-without-chronic-dysbiosis/#DIY-antiseptic | ||||||||||||
| 229 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 12/03/2026 12:06 PM | [TOOLS] | Tools | Milligram Scales | 1 | 102 | EU | Tools | 1 | https://www.amazon.de/dp/B0F9YHJD8F | For measuring small quantities of supplements. | ||||||||||||||
| 230 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 12/03/2026 12:07 PM | [TOOLS] | Tools | Measuring Spoons | 1 | 103 | EU | Tools | 1 | https://www.amazon.de/dp/B0876LFM9Y | For quickly measuring small quantities supplements. | ||||||||||||||
| 233 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 13/03/2026 07:13 AM | [DIY SHAKE] | Vitamins | B8 Myo & D-Chiro Inositol | 3 caps | 3 caps | 3 caps | For AU source, 1.5g = 3 caps. DE source has 20% more per cap. | 1 | 1 | Start with a target dose around 2.5mg D-chiro inositol (approx 1/4 capsule) and increase. | 2 | AU | Vitamins | 1 | https://www.woolworths.com.au/shop/productdetails/1122169455/switch-nutrition-myo-d-chiro-inositol-150g | Myo-inositol + D-chiro inositol. Glucose uptake and glycogen synthesis. | https://bornfree.life/learn/4-3-diy-powder | |||||||
| 234 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 25/09/2024 06:19 AM | [DIY SHAKE] | Vitamins | B5 Pantothenic Acid | 0.7-3.5g | 0.7-3.5g | 0.7-3.5g | 1 | 1 | Normally well-tolerated | 3 | AU | Vitamins | 9g-45g | https://www.bulksupplements.com/products/vitamin-b5-calcium-pantothenate-pantothenic-acid-powder?variant=32133465342063 | Required for coenzyme A (CoA) and helps regulate lipolysis at VNN1. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 236 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 15/10/2024 12:13 PM | [DIY SHAKE] | Supplements | PQQ+CoQ10 | 7 - 21 caps | 7 - 21 caps | 7 - 21 caps | 1 | 1 | Normally well-tolerated. Amount needed depends on mineral deficiency data / dose response | 5 | AU | Supplements | 3–9 | https://iherb.com/pr/lake-avenue-nutrition-coq10-with-pqq-100-mg-60-veggie-capsules/97389 | DBH promoter, Electron Transport Chain support. CoQ10 can promote fungal growth. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 237 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [DIY SHAKE] | Supplements | Apigenin | 7 - 56 caps | 7 - 56 caps | 7 - 56 caps | 1 | 1 | Normally well tolerated. Amount required depends on mineral deficiency data and dose response | 6 | AU | Supplements | 1–8 | https://iherb.com/pr/codeage-liposomal-apigenin-non-gmo-vegan-90-capsules/114120 | ALDH, p38 MAPK inhibitor, TGF-b1 modulator and NADase inhibitor. Start at ¼ dose and increase. Upper threshold for effective dose may be 400mg/day. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 239 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 23/11/2025 05:59 AM | [DIY SHAKE] | Minerals | Kelp | 7g | 7g | 7g | 1 | 1 | Target daily dose 1g. Start slowly and increase to daily values, as tolerated | 9 | AU | Minerals | 90g | https://iherb.com/pr/now-foods-organic-kelp-pure-powder-8-oz-227-g/16668 | Bromine and iodine source. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 243 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 17/11/2025 02:57 AM | [DIY SIPPER/SHOTS] | Electrolytes | Monocalcium Phosphate | 35g | 35g | 35g | 5g / day | 1 | 1 | 1 | 5g / day. Correcting calcium deficiency can unblock adrenergic signallng bottlenecks and expose temporary receptor hypersensitivity. Substitute for monosodium phosphate + alternate calcium for very slow calcium titration | 14 | AU | Electrolytes | 450g | https://allchemical.com.au/shop/monocalcium-phosphate-anhydrous-food-grade/ | Calcium - critical electrolyte. Oral dosing works but can feed biofilms. Phosphate - critical electrolyte for energy metabolism (e.g. P5P, glycolysis, etc). Oral dosing is “okay”. Low phosphorus may indicate acidemia - add bicarb. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 244 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 11/09/2024 07:22 AM | [DIY SIPPER/SHOTS] | Electrolytes | Magnesium Aspartate | 38.5g | 38.5g | 38.5g | 5.5g / day | 1 | 1 | 1 | 5.5g / day | 15 | AU | Electrolytes | 500g | https://www.amazon.com.au/dp/B0D6TGQZXM | Critical electrolyte for energy metabolism, etc. Low magnesium can also cause arrhythmia, muscle spasms. Aspartate assists with urea cycle and energy metabolism. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 245 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 11/08/2024 11:29 AM | [DIY SIPPER/SHOTS] | Electrolytes | Potassium Citrate | 91g | 91g | 91g | 13g / day | 1 | 1 | 1 | 13g / day. Correcting potassium deficiency can unblock adrenergic signallng bottlenecks and expose temporary receptor hypersensitivity. Start slowly | 16 | AU | Electrolytes | 900g | https://www.bulksupplements.com/products/potassium-citrate-powder | Critical electrolyte. Oral dosing is okay. Low potassium can cause high blood pressure, arrhythmia, muscle spasms, low glutamate and dopamine synthesis, impaired glycolysis. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 246 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [DIY SIPPER/SHOTS] | Amino Acids | Taurine | 84g | 84g | 84g | 12g / day. Can be taken sublingually if sulphur reducing bacteria suspected. Start low / find tolerable dose and increase. | 1 | 1 | 1 | 12g / day. Can be used sublingually, if gut microbiome dysbiosis is severe. Start low / find tolerable dose and increase | 17 | AU | Amino Acids | 1.08kg | https://www.bulknutrients.com.au/products/taurine | GLUT2, glycogen synthesis, promotes ALDH for aldehyde degradation, adrenaline inhibition. TUDCA synthesis. Note: can feed Bilophila wadsworthia, etc. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 247 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 18/03/2026 09:00 AM | [DIY SIPPER/SHOTS] | Amino Acids | Acetyl L-Carnitine | 28g | 28g | 28g | 4g / day. Can be used sublingually, if gut microbiome dysbiosis is severe. | 1 | 1 | 1 | 4g / day. Can be used sublingually, if gut microbiome dysbiosis is severe. | 18 | AU | Amino Acids | 360g | https://www.bulksupplements.com/products/l-carnitine-base-powder?variant=32133418188911 | Fatty acid transport, dopamine synthesis promoter. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 253 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [DIY SIPPER/SHOTS] | Amino Acids | Creatine | 35g | 35g | 35g | 5g / day | 1 | 1 | 1 | 5g / day | 24 | AU | Amino Acids | 450g | https://www.bulknutrients.com.au/products/creatine-monohydrate | GLUT4, ATP, SAMe metabolism efficiency. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 255 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 13/03/2026 01:43 AM | [DIY SHAKE] | Minerals | Bamboo (Silica) | 14g | 14g | 14g | 1 | 1 | Start slowly and increase to protocol doses, as tolerated | 26 | AU | Minerals | 12 | https://swansonaustralia.com/products/buy-now-foods-solutions-bamboo-silica-beauty-90-veg-capsules-online-from-swanson-australia | Silicon deficiency – HIF-1a. Antiviral. Magnesium uptake. Collagen. Silica will also be heavily used to excrete acetaldehyde and toxic metals. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 257 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 13/09/2024 06:44 AM | [DIY SHAKE] | Supplements | R-ALA | 4.2g | 4.2g | 4.2g | 1 | 1 | Start slowly - can break biofilm and trigger some herxheimer reactions. | 28 | AU | Supplements | 50.4g | https://www.bulksupplements.com/products/r-alpha-lipoic-acid-r-ala-powder | ALDH2 promoter. AMPK promoter – insulin sensitivity. Biofilm breaker. Toxic metal chelator. TCA cycle support.. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 258 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [DIY SIPPER/SHOTS] | Supplements | NAC | 3.5-7g | 3.5-7g | 21g | 0.5-1g / day. In Stage 3, cycle an increased dose of 3g / day for 3 weeks, then revert for 3 weeks, indefinitely. | 1 | 1 | 1 | 0.5-1g / day. Start slowly | 29 | AU | Amino Acids | 97.5–132g | https://www.ebay.com.au/itm/204114762944 | Thrombolytic, mucolytic, antioxidant, detoxifier, biofilm breaker and metal chelator. Can cause die-off in large doses. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 265 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 11/08/2024 11:30 AM | [DIY SIPPER/SHOTS] | Electrolytes | Sodium Chloride | 35-50g | 35-50g | 35-50g | 5-7.1g/day | 1 | 1 | 1 | 5-7g / day | 37 | AU | Electrolytes | 450-900g | https://www.woolworths.com.au/shop/productdetails/320992/mckenzie-s-natural-salt-sea | Critical electrolyte. Oral dosing is okay. Low sodium can cause low blood pressure and low dopamine transport. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 269 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 12/03/2026 10:58 AM | [REPLETION] | Vitamins | B1 Thiamine | 1 | 1 | (Also found in the compounded minerals) Equivalent to 1-2 x 500mg Thiamine HCL or more, 2x/day | 44 | AU | Vitamins | 3 | https://iherb.com/pr/source-naturals-high-potency-b-1-500-mg-100-tablets/980 | TPP / energy metabolism, affected by acetaldehyde. Increase from a tenth dose. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 270 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 17/09/2024 02:08 AM | [REPLETION] | Vitamins | B9 5-MTHF | 1 | 1 | Start very slowly - may unblock methylation -> SAMe -> epinephrine synthesis and only parts of the degradation pathway, if taken in isolation. | 45 | AU | Vitamins | 1 | https://iherb.com/pr/life-extension-optimized-folate-1-700-mcg-dfe-100-vegetarian-tablets/63828 | Methylation cycle, BH4. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 273 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 29/09/2024 04:43 AM | [DIY SHAKE] | Vitamins | C Ascorbate | 14g | 14g | 14g | 1 | 1 | Start slowly and increase. Can be a bumpy start | 48 | AU | Vitamins | 1 | https://iherb.com/pr/california-gold-nutrition-gold-c-usp-grade-vitamin-c-1-000-mg-240-veggie-capsules/61865 | Antioxidant. HIF-1a, DBH, collagen synthesis. Use away from copper dosing. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 281 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 11/08/2024 11:35 AM | [OTHER SUPPLEMENTS] | Electrolytes | Magnesium Spray | 1 | 1 | Apply after showering | 56 | AU | Electrolytes | 4 | https://www.mrvitamins.com.au/products/nts-magsorb-mg-oil | Critical electrolyte for energy metabolism, etc. Low magnesium can also cause arrhythmia, muscle spasms. Transdermal absorption provides a slow release profile. | https://bornfree.life/learn/4-1-electrolytes/ | |||||||||||
| 282 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 12/09/2024 02:12 AM | [REPLETION] | Minerals | Vanadium | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 57 | AU | Minerals | 1 | https://iherb.com/pr/source-naturals-vanadyl-sulfate-10-mg-100-tablets/1477 | (Sublingual) Required for glucose transport and insulin sensitivity. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 283 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [REPLETION] | Minerals | Lithium | 1 | 1 | Start slowly and increase to protocol doses, as tolerated | 58 | AU | Minerals | 1 | https://iherb.com/pr/kal-lithium-orotate-5-mg-120-vegcaps/85528 | Adrenergic metabolism / inhibition. Glycogen‑Synthase‑Kinase‑3β inhibition.. Magnesium reabsorption. Immunity. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 284 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [REPLETION] | Minerals | Molybdenum | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 59 | AU | Minerals | 1 | https://iherb.com/pr/source-naturals-reduced-glutathione-complex-orange-50-mg-100-lozenges/1407 | (Sublingual) RIboflavin metabolism. B6 degradation. Taurine metabolism. ALDH. XO. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 285 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [REPLETION] | Minerals | Selenium | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 60 | AU | Minerals | 1 | https://iherb.com/pr/california-gold-nutrition-selenium-yeast-free-200-mcg-180-veggie-capsules/90416 | (Sublingual) Thyroid and glutathione metabolism. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 286 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 12/03/2026 11:31 PM | [REPLETION] | Minerals | Chromium | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 61 | AU | Minerals | 1 | https://iherb.com/pr/solaray-chromium-picolinate-lozenges-natural-lemon-raspberry-1-000-mcg-100-lozenges/124399 | (Sublingual) Required for glucose transport and insulin sensitivity. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 287 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [REPLETION] | Minerals | Sulphur | 1 | 1 | Start slowly and increase to protocol doses, as tolerated | 62 | AU | Minerals | 3 | https://iherb.com/pr/doctor-s-best-msm-with-optimsm-1-500-mg-120-tablets/3 | Iron-sulphur clusters. Oxalate transport. Transsulfuration pathway | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 288 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [REPLETION] | Minerals | Zinc | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 63 | AU | Minerals | 3 | https://iherb.com/pr/source-naturals-wellness-zinc-lozenges-peach-raspberry-23-mg-120-lozenges/1476 | (Sublingual) Catabolic pathways. Glycolysis. HIF-1a. Methylation + folate transport. BH4. ALDH. LDH. NOS. RK. P5P. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 289 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [REPLETION] | Minerals | Copper | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 64 | AU | Minerals | 2 | https://iherb.com/pr/solaray-copper-2-mg-100-vegcaps/70102 | (Sublingual) Dopamine precursors. Dopamine beta hydroxylase. CuZnSOD. Glycolysis. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 290 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 27/08/2024 05:26 AM | [REPLETION] | Vitamins | B7 Biotin | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 65 | AU | Vitamins | 1 | https://iherb.com/pr/solaray-biotin-natural-orange-1-000-mcg-100-lozenges/123883 | (Sublingual) Required for normal energy metabolism, however will feed fungal infections and promote fungal bloom, if infections are not sufficiently inhibited / managed. Oral dosing fails in alcoholism. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 291 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 19/08/2024 05:04 AM | [REPLETION] | Vitamins | B6 P5P | 1 | 1 | (Sublingual, also found in the compounded minerals) Generally well tolerated | 66 | AU | Vitamins | 1 | https://iherb.com/pr/swanson-p-5-p-pyridoxal-5-phosphate-20-mg-60-capsules/117697 | Problematic when ALDH deficiency exists, but a critical coenzyme for metabolism. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 297 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 12/03/2026 10:53 AM | [REPLETION] | Minerals | Manganese | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 74 | AU | Minerals | 1 | https://iherb.com/pr/bodybio-liquid-mineral-manganese-2-fl-oz-59-ml/150520 | (Sublingual) 2 drops. Supports MnSOD. Folate metabolism. Glycocalyx. GDH. Gluconeogenesis (PCB. ME1. PLD). | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 298 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 04/03/2026 01:18 AM | [REPLETION] | Vitamins | B2 FMN Riboflavin | 1 | 1 | (Sublingual, also found in the compounded minerals) 25mg, 3x/day | 75 | AU | Vitamins | 7g | https://prescribedforlife.com/products/riboflavin-5-phosphate-riboflavin-5-phosphate-sodium-powder-html | (Sublingual) Absorbable FMN and FAD support. Has antimicrobial functions. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 299 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 29/11/2025 04:11 AM | [REPLETION] | Vitamins | B3 NAD+/H | 1 | 1 | (Sublingual) 5-40mg, 2x/day | 76 | AU | Vitamins | 7.2g | https://www.bulksupplements.com/products/nad-supplement | (Sublingual) NAD+:NADH pool support for wide array of metabolic pathways. IFN-γ activity. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 300 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 19/08/2024 05:15 AM | [REPLETION] | Vitamins | B12 Cobalamin | Sublingual | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to 1-2mg, as tolerated | 77 | AU | Vitamins | 1 | https://vimergy.com/products/organic-b12 | (Sublingual) Methylation. Antioxidant. Catabolic pathways -> TCA cycle. | https://bornfree.life/learn/2-3-2-remineralisation/ | ||||||||||
| 307 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 12/03/2026 11:44 PM | [REPLETION] | Minerals | Cobalt | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to protocol doses, as tolerated | 84 | AU | Minerals | 1 | https://www.ebay.com.au/itm/175475038064 | (Sublingual) EPO regulation. Iron homeostasis. B12 synthesis (microbial). FAD synthesis, P5P synthesis | ||||||||||||
| 308 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 10/08/2024 09:44 AM | [REPLETION] | Minerals | Germanium GE-132 | 1 | 1 | Start slowly and increase to daily values, as tolerated | 85 | AU | Minerals | 2 | https://www.nutricology.com/organo-germanium-50-vegetarian-capsules | Antioxidant and other functions. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 322 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 11/08/2024 11:28 AM | [TOOLS] | Tools | Empty Bottles | 1 | 99 | AU | Antiseptic | 1 | 1 | https://www.amazon.com.au/Magic-Season-Boston-Bottles-Dropper/dp/B09919MRFD | Required for temporary storage and dosing of various recipes. | https://bornfree.life/learn/2-2-3-living-without-chronic-dysbiosis/#DIY-antiseptic | ||||||||||||
| 324 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 11/08/2024 11:30 AM | [TOOLS] | Tools | Milligram Scales | 1 | 102 | AU | Tools | 1 | https://www.ebay.com.au/itm/294932194562 | For measuring small quantities of supplements. | ||||||||||||||
| 325 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 12/03/2026 12:09 PM | [TOOLS] | Tools | Measuring Spoons | 1 | 103 | AU | Tools | 1 | https://www.amazon.com.au/dp/B0DFM1DMKD | For quickly measuring small quantities supplements. | ||||||||||||||
| 332 | 3dghs | 18/08/2024 09:09 AM | 3dghs | 18/08/2024 09:09 AM | [DIY SIPPER/SHOTS] | Electrolytes | Sodium Bicarbonate | 35g | 35g | 35g | 5g / day. Must be taken away from meals. | 1 | 1 | 1 | 5g / day | 107 | AU | Electrolytes | 1 | https://www.woolworths.com.au/shop/productdetails/251189/essentials-bicarbonate-soda | Electrolyte. Helpful for buffering lactic acid metabolism and balancing pH. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 333 | 3dghs | 18/08/2024 09:15 AM | 3dghs | 18/08/2024 09:15 AM | [DIY SIPPER/SHOTS] | Electrolytes | Sodium Bicarbonate | 35g | 35g | 35g | 5g / day. Must be taken away from meals. | 1 | 1 | 1 | 5g / day | 107 | EU | Electrolytes | 1 | https://www.amazon.de/dp/B0C14Y71QY/ | Electrolyte. Helpful for buffering lactic acid metabolism and balancing pH. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 334 | 3dghs | 18/08/2024 09:21 AM | 3dghs | 18/08/2024 09:21 AM | [DIY SIPPER/SHOTS] | Electrolytes | Sodium Bicarbonate | 35g | 35g | 35g | 5g / day. Must be taken away from meals. | 1 | 1 | 1 | 5g / day | 107 | US | Electrolytes | 1 | https://www.amazon.com/dp/B008LBAECE/ | Electrolyte. Helpful for buffering lactic acid metabolism and balancing pH. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 344 | 3dghs | 27/08/2024 05:30 AM | 3dghs | 27/08/2024 05:30 AM | [OTHER SUPPLEMENTS] | Vitamins | Gamma E Complex | 1 | 1 | Normally well-tolerated @ 1-2 servings per day | 111 | US | Vitamins | 2 | https://iherb.com/pr/now-foods-gamma-e-complex-advanced-120-softgels/299 | Provides mixed tocopherols and tocotrienols, where diet is lacking or CMA indicates deficiency. | ||||||||||||
| 345 | 3dghs | 27/08/2024 05:30 AM | 3dghs | 27/08/2024 05:30 AM | [OTHER SUPPLEMENTS] | Vitamins | Gamma E Complex | 1 | 1 | Normally well-tolerated @ 1-2 servings per day | 111 | AU | Vitamins | 2 | https://iherb.com/pr/now-foods-gamma-e-complex-advanced-120-softgels/299 | Provides mixed tocopherols and tocotrienols, where diet is lacking or CMA indicates deficiency. | ||||||||||||
| 346 | 3dghs | 27/08/2024 05:30 AM | 3dghs | 27/08/2024 05:31 AM | [OTHER SUPPLEMENTS] | Vitamins | Gamma E Complex | 1 | 1 | Normally well-tolerated @ 1-2 servings per day | 111 | EU | Vitamins | 2 | https://iherb.com/pr/now-foods-gamma-e-complex-advanced-120-softgels/299 | Provides mixed tocopherols and tocotrienols, where diet is lacking or CMA indicates deficiency. | ||||||||||||
| 350 | 3dghs | 11/08/2024 10:43 AM | 3dghs2 | 08/03/2026 08:05 AM | [TOOLS] | Tools | Kitchen Scales | 1 | 113 | AU | Tools | 1 | https://www.ebay.com.au/itm/336101572619 | Assists with measuring food item and supplement weights | https://bornfree.life/learn/4-3-diy-powder/ | |||||||||||||
| 351 | 3dghs | 11/08/2024 10:43 AM | 3dghs | 17/09/2024 12:38 AM | [TOOLS] | Tools | Kitchen Scales | 1 | 113 | US | Tools | 1 | https://www.amazon.com/dp/B0811RX62R/ | Assists with measuring food item and supplement weights | https://bornfree.life/learn/4-3-diy-powder/ | |||||||||||||
| 352 | 3dghs | 11/08/2024 10:43 AM | 3dghs | 17/09/2024 12:40 AM | [TOOLS] | Tools | Kitchen Scales | 1 | 113 | EU | Tools | 1 | https://www.amazon.de//dp/B0817LMPDX/ | Assists with measuring food item and supplement weights | https://bornfree.life/learn/4-3-diy-powder/ | |||||||||||||
| 353 | 3dghs | 11/08/2024 10:43 AM | 3dghs | 17/09/2024 12:42 AM | [TOOLS] | Tools | Empty Buckets | 1 | 114 | AU | Tools | 1 | https://www.ebay.com.au/itm/334715304879 | For DIY shake and sipper preparation | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | |||||||||||||
| 354 | 3dghs | 11/08/2024 10:43 AM | 3dghs2 | 12/03/2026 11:49 AM | [TOOLS] | Tools | Empty Buckets | 1 | 114 | US | Tools | 1 | https://www.amazon.com/dp/B0D9PV3S4B | For DIY shake and sipper preparation | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | |||||||||||||
| 355 | 3dghs | 11/08/2024 10:43 AM | 3dghs | 17/09/2024 12:51 AM | [TOOLS] | Tools | Empty Buckets | 1 | 114 | EU | Tools | 1 | https://www.amazon.de/dp/B08DRKF4QX/ | For DIY shake and sipper preparation | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | |||||||||||||
| 359 | 3dghs | 10/08/2024 09:44 AM | 3dghs | 25/09/2024 06:17 AM | [DIY SHAKE] | Vitamins | B5 Pantothenic Acid | 0.7-3.5g | 0.7-3.5g | 0.7-3.5g | 1 | 1 | Normally well-tolerated | 3 | ALT | Vitamins | 1 | https://iherb.com/pr/source-naturals-pantothenic-acid-100-mg-250-tablets/1357 | Required for coenzyme A (CoA) and helps regulate lipolysis at VNN1. | https://bornfree.life/learn/4-3-diy-powder | ||||||||
| 360 | 3dghs | 03/04/2025 02:12 AM | 3dghs | 03/04/2025 02:12 AM | [DIY SIPPER/SHOTS] | Supplements | N-AcetylGlucosamine | 21g | 21g | 21g | 2.5-3g / day. Well-tolerated, although supports growth of some microorganisms. Can be started / consumed sublingually. Vegan / non-shellfish selected. Alternate available. | 1 | 1 | 1 | 2.5-3g / day. Well-tolerated, although supports growth of some microorganisms - start sublingually, if in doubt | 116 | US | Supplements | 3 | https://iherb.com/pr/jarrow-formulas-n-a-g-700-mg-120-veggie-capsules/131 | Support glycocalyx assembly, inflammation and leaky junctions, where glycolysis and glutamine are impaired. Promotes microbials species - see list in 2.2.3 -- Glycocalyx. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 361 | 3dghs | 03/04/2025 02:12 AM | 3dghs | 03/04/2025 02:14 AM | [DIY SIPPER/SHOTS] | Supplements | N-AcetylGlucosamine | 21g | 21g | 21g | 2.5-3g / day. Well-tolerated, although supports growth of some microorganisms. Can be started / consumed sublingually. Vegan / non-shellfish selected. Alternate available. | 1 | 1 | 1 | 2.5-3g / day. Well-tolerated, although supports growth of some microorganisms - start sublingually, if in doubt | 116 | EU | Supplements | 4.5 | https://www.sunday.de/en/n-acetylglucosamine-capsules.html | Support glycocalyx assembly, inflammation and leaky junctions, where glycolysis and glutamine are impaired. Promotes microbials species - see list in 2.2.3 -- Glycocalyx. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 362 | 3dghs | 03/04/2025 02:12 AM | 3dghs | 03/04/2025 02:15 AM | [DIY SIPPER/SHOTS] | Supplements | N-AcetylGlucosamine | 21g | 21g | 21g | 2.5-3g / day. Well-tolerated, although supports growth of some microorganisms. Can be started / consumed sublingually. Vegan / non-shellfish selected. Alternate available. | 1 | 1 | 1 | 2.5-3g / day. Well-tolerated, although supports growth of some microorganisms - start sublingually, if in doubt | 116 | AU | Supplements | 3 | https://iherb.com/pr/jarrow-formulas-n-a-g-700-mg-120-veggie-capsules/131 | Support glycocalyx assembly, inflammation and leaky junctions, where glycolysis and glutamine are impaired. Promotes microbials species - see list in 2.2.3 -- Glycocalyx. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 363 | 3dghs | 03/04/2025 02:12 AM | 3dghs | 03/04/2025 02:21 AM | [DIY SIPPER/SHOTS] | Supplements | N-AcetylGlucosamine (shellfish) | 21g | 21g | 21g | 2.5-3g / day. Well-tolerated, although supports growth of some microorganisms. Can be started / consumed sublingually. Vegan / non-shellfish selected. Alternate available. | 1 | 1 | 1 | 2.5-3g / day. Well-tolerated, although supports growth of some microorganisms - start sublingually, if in doubt | 116 | ALT | Supplements | 270g | https://www.bulksupplements.com/products/n-acetyl-d-glucosamine-nag-powder/ | Support glycocalyx assembly, inflammation and leaky junctions, where glycolysis and glutamine are impaired. Promotes microbials species - see list in 2.2.3 -- Glycocalyx. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 364 | 3dghs | 03/04/2025 02:19 AM | 3dghs | 03/04/2025 02:19 AM | [DIY SIPPER/SHOTS] | Supplements | Hyaluronic Acid | 3.5g | 3.5g | 3.5g | 500mg / day. Well-tolerated. | 1 | 1 | 1 | 500mg / day. Well-tolerated | 117 | US | Supplements | 90g | https://www.bulksupplements.com/products/hyaluronic-acid-sodium-hyaluronate-powder | Support glycocalyx assembly, inflammation and leaky junctions, where glycolysis and glutamine are impaired. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 365 | 3dghs | 03/04/2025 02:19 AM | 3dghs | 03/04/2025 02:20 AM | [DIY SIPPER/SHOTS] | Supplements | Hyaluronic Acid | 3.5g | 3.5g | 3.5g | 500mg / day. Well-tolerated. | 1 | 1 | 1 | 500mg / day. Well-tolerated | 117 | EU | Supplements | 90g | https://www.bulksupplements.com/products/hyaluronic-acid-sodium-hyaluronate-powder | Support glycocalyx assembly, inflammation and leaky junctions, where glycolysis and glutamine are impaired. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 366 | 3dghs | 03/04/2025 02:19 AM | 3dghs | 03/04/2025 02:20 AM | [DIY SIPPER/SHOTS] | Supplements | Hyaluronic Acid | 3.5g | 3.5g | 3.5g | 500mg / day. Well-tolerated. | 1 | 1 | 1 | 500mg / day. Well-tolerated | 117 | AU | Supplements | 90g | https://purewellness.com.au/product/hyaluronic-acid-powder/ | Support glycocalyx assembly, inflammation and leaky junctions, where glycolysis and glutamine are impaired. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 367 | 3dghs | 03/04/2025 02:19 AM | 3dghs | 03/04/2025 02:21 AM | [DIY SIPPER/SHOTS] | Supplements | Hyaluronic Acid | 3.5g | 3.5g | 3.5g | 500mg / day. Well-tolerated. | 1 | 1 | 1 | 500mg / day. Well-tolerated | 117 | ALT | Supplements | 2 | https://iherb.com/pr/nutricost-hyaluronic-acid-unflavored-1-8-oz-50-g/147244 | Support glycocalyx assembly, inflammation and leaky junctions, where glycolysis and glutamine are impaired. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 368 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 29/11/2025 04:13 AM | [REPLETION] | Vitamins | B3 NADH | 1 | 1 | (Sublingual) 5-40mg, 2x/day | 76 | ALT | Vitamins | 7.2g (1.5) | https://nootropicsdepot.com/nadh-powder/ | (Sublingual) NAD+:NADH pool support for wide array of metabolic pathways. IFN-γ activity. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 369 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 18/11/2025 02:52 AM | [REPLETION] | Supplements | Uridine Monophosphate | 1 | 1 | 50-100mg, sublingually, 2x/day | 118 | US | Supplements | 18g | https://nootropicsdepot.com/uridine-monophosphate-disodium-salt-powder/ | (Sublingual) Supports glycogen synthesis, phosphatidylcholine, neural lipid membrane repair, dopamine homeostasis. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 370 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 18/11/2025 02:52 AM | [REPLETION] | Supplements | Uridine Monophosphate | 1 | 1 | 50-100mg, sublingually, 2x/day | 118 | EU | Supplements | 18g | https://nootropicsdepot.com/uridine-monophosphate-disodium-salt-powder/ | (Sublingual) Supports glycogen synthesis, phosphatidylcholine, neural lipid membrane repair, dopamine homeostasis. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 371 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 18/11/2025 02:52 AM | [REPLETION] | Supplements | Uridine Monophosphate | 1 | 1 | 50-100mg, sublingually, 2x/day | 118 | AU | Supplements | 18g | https://nootropicsdepot.com/uridine-monophosphate-disodium-salt-powder/ | (Sublingual) Supports glycogen synthesis, phosphatidylcholine, neural lipid membrane repair, dopamine homeostasis. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 372 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 12/03/2026 10:17 AM | [DIY SIPPER/SHOTS] | Supplements | D-Ribose | 70g | 70g | 70g | Start slowly and increase to potentially 10g total, over the day. Can increase glucose uptake -> glycogen synthesis, exposing dietary carbohydrate insufficency. | 1 | 1 | 1 | Start slowly and increase to potentially 10g total, over the day. Can increase glucose uptake -> glycogen synthesis, exposing dietary carbohydrate insufficency | 119 | US | Supplements | 900g | https://www.bulksupplements.com/products/d-ribose-powder?variant=32133394595951 | PRPP / R1P / R5P synthesis, required for NAD+, purine and pyrimidine homeostasis. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 373 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 12/03/2026 10:17 AM | [DIY SIPPER/SHOTS] | Supplements | D-Ribose | 70g | 70g | 70g | Start slowly and increase to potentially 10g total, over the day. Can increase glucose uptake -> glycogen synthesis, exposing dietary carbohydrate insufficency. | 1 | 1 | 1 | Start slowly and increase to potentially 10g total, over the day. Can increase glucose uptake -> glycogen synthesis, exposing dietary carbohydrate insufficency | 119 | EU | Supplements | 900g | https://www.bulksupplements.com/products/d-ribose-powder?variant=32133394595951 | PRPP / R1P / R5P synthesis, required for NAD+, purine and pyrimidine homeostasis. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 374 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 12/03/2026 10:17 AM | [DIY SIPPER/SHOTS] | Supplements | D-Ribose | 70g | 70g | 70g | Start slowly and increase to potentially 10g total, over the day. Can increase glucose uptake -> glycogen synthesis, exposing dietary carbohydrate insufficency. | 1 | 1 | 1 | Start slowly and increase to potentially 10g total, over the day. Can increase glucose uptake -> glycogen synthesis, exposing dietary carbohydrate insufficency | 119 | AU | Supplements | 900g | https://www.bulksupplements.com/products/d-ribose-powder?variant=32133394595951 | PRPP / R1P / R5P synthesis, required for NAD+, purine and pyrimidine homeostasis. | https://bornfree.life/learn/4-3-diy-powder/#4.3-DIY-sipper | ||||||
| 375 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 19/11/2025 05:38 AM | [REPLETION] | Minerals | Rubidium | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to 5-10mg, as tolerated | 120 | US | Minerals | 0.45g | https://pglchem.com/product/rubidium-chloride/ | Catecholamine homeostasis, copper metabolism. Typical daily intake is 5mg. | ||||||||||||
| 376 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 19/11/2025 05:38 AM | [REPLETION] | Minerals | Rubidium | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to 5-10mg, as tolerated | 120 | EU | Minerals | 0.45g | https://pglchem.com/product/rubidium-chloride/ | Catecholamine homeostasis, copper metabolism. Typical daily intake is 5mg. | ||||||||||||
| 377 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 19/11/2025 05:38 AM | [REPLETION] | Minerals | Rubidium | 1 | 1 | (Sublingual, also found in the compounded minerals) Start slowly and increase to 5-10mg, as tolerated | 120 | AU | Minerals | 0.45g | https://pglchem.com/product/rubidium-chloride/ | Catecholamine homeostasis, copper metabolism. Typical daily intake is 5mg. | ||||||||||||
| 378 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 13/03/2026 12:18 PM | [REPLETION] | Minerals | Compounded Nutrients | 1 | 1 | Used INSTEAD of separate B1,2,6,9,12 and zinc + many other minerals (currently excludes cobalt, lithium). Contains wide range of potent optimised B vitamins and minerals that bypass standard oral route. Slowly titrate. | 121 | US | Minerals | 3 months | https://healthdispensary.au/product/customised-dmso-multivitamin-transdermal-born-free-protocol-certified/ | Bypasses oral absorption issues during chronic inflammation. Convenience. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 379 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 13/03/2026 12:19 PM | [REPLETION] | Minerals | Compounded Nutrients | 1 | 1 | Used INSTEAD of separate B1,2,6,9,12 and zinc + many other minerals (currently excludes cobalt, lithium). Contains wide range of potent optimised B vitamins and minerals that bypass standard oral route. Slowly titrate. | 121 | EU | Minerals | 3 months | https://healthdispensary.au/product/customised-dmso-multivitamin-transdermal-born-free-protocol-certified/ | Bypasses oral absorption issues during chronic inflammation. Convenience. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 380 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 13/03/2026 12:19 PM | [REPLETION] | Minerals | Compounded Nutrients | 1 | 1 | Used INSTEAD of separate B1,2,6,9,12 and zinc + many other minerals (currently excludes cobalt, lithium). Contains wide range of potent optimised B vitamins and minerals that bypass standard oral route. Slowly titrate. | 121 | AU | Minerals | 3 months | https://healthdispensary.au/product/customised-dmso-multivitamin-transdermal-born-free-protocol-certified/ | Bypasses oral absorption issues during chronic inflammation. Convenience. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 381 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 19/11/2025 05:33 AM | [OTHER SUPPLEMENTS] | Supplements | Methylene Blue | 1 | 1 | 50(-300mcg) in water, 1x/day | 122 | US | Supplements | 0.1 | https://www.amazon.com/Methylene-Blue-Solution-3-4-Heiltropfen%C2%AE/dp/B0DJZB5VP7/ | Microdosing provides support for Mitochondrial Complex I -> Cytc | https://bornfree.life/learn/2-3-1-herxheimer-die-off-acetaldehyde-support/#mb-nad-pool | |||||||||||
| 382 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 12/03/2026 11:54 AM | [OTHER SUPPLEMENTS] | Supplements | Methylene Blue | 1 | 1 | 50(-300mcg) in water, 1x/day | 122 | EU | Supplements | 0.1 | https://www.amazon.de/dp/B0D8W5CWDK | Microdosing provides support for Mitochondrial Complex I -> Cytc | https://bornfree.life/learn/2-3-1-herxheimer-die-off-acetaldehyde-support/#mb-nad-pool | |||||||||||
| 383 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 19/11/2025 05:34 AM | [OTHER SUPPLEMENTS] | Supplements | Methylene Blue | 1 | 1 | 50(-300mcg) in water, 1x/day | 122 | AU | Supplements | 0.1 | https://www.amazon.com/dp/B0DXDH5SGH/ | Microdosing provides support for Mitochondrial Complex I -> Cytc | https://bornfree.life/learn/2-3-1-herxheimer-die-off-acetaldehyde-support/#mb-nad-pool | |||||||||||
| 384 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 23/11/2025 05:26 AM | [SEVERE ONLY] | Onboarding (Severe) | (Titrating) B1 / TPP | 1 | 1 | 1 | (Sublingual) Start at 1 drop in the morning and increase or pause, as tolerable. | 123 | US | Onboarding (Severe) | 1 | https://www.metabolics.com/products/vitamin-b1-thiamine-pyrophosphate | (Sublingual) For onboarding Vitamin B1 with severe / neuropsychiatric symptoms susceptibility. | https://bornfree.life/learn/2-the-protocol/#severe | ||||||||||
| 385 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 23/11/2025 05:26 AM | [SEVERE ONLY] | Onboarding (Severe) | (Titrating) B1 / TPP | 1 | 1 | 1 | (Sublingual) Start at 1 drop in the morning and increase or pause, as tolerable. | 123 | EU | Onboarding (Severe) | 1 | https://www.metabolics.com/products/vitamin-b1-thiamine-pyrophosphate | (Sublingual) For onboarding Vitamin B1 with severe / neuropsychiatric symptoms susceptibility. | https://bornfree.life/learn/2-the-protocol/#severe | ||||||||||
| 386 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 23/11/2025 05:26 AM | [SEVERE ONLY] | Onboarding (Severe) | (Titrating) B1 / TPP | 1 | 1 | 1 | (Sublingual) Start at 1 drop in the morning and increase or pause, as tolerable. | 123 | AU | Onboarding (Severe) | 1 | https://www.metabolics.com/products/vitamin-b1-thiamine-pyrophosphate | (Sublingual) For onboarding Vitamin B1 with severe / neuropsychiatric symptoms susceptibility. | https://bornfree.life/learn/2-the-protocol/#severe | ||||||||||
| 387 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 23/11/2025 05:26 AM | [SEVERE ONLY] | Onboarding (Severe) | (Titrating) B2 / FMN | 1 | 1 | 1 | (Sublingual) Start at 1 drop in the morning and increase or pause, as tolerable.Start at 1 drop in the morning and increase or pause, as tolerable. | 124 | US | Onboarding (Severe) | 1 | https://www.metabolics.com/products/riboflavin-5-phosphate | (Sublingual) For onboarding Vitamin B2 with severe / neuropsychiatric symptoms susceptibility. | https://bornfree.life/learn/2-the-protocol/#severe | ||||||||||
| 388 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 23/11/2025 05:26 AM | [SEVERE ONLY] | Onboarding (Severe) | (Titrating) B2 / FMN | 1 | 1 | 1 | (Sublingual) Start at 1 drop in the morning and increase or pause, as tolerable.Start at 1 drop in the morning and increase or pause, as tolerable. | 124 | EU | Onboarding (Severe) | 1 | https://www.metabolics.com/products/riboflavin-5-phosphate | (Sublingual) For onboarding Vitamin B2 with severe / neuropsychiatric symptoms susceptibility. | https://bornfree.life/learn/2-the-protocol/#severe | ||||||||||
| 389 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 23/11/2025 05:26 AM | [SEVERE ONLY] | Onboarding (Severe) | (Titrating) B2 / FMN | 1 | 1 | 1 | (Sublingual) Start at 1 drop in the morning and increase or pause, as tolerable.Start at 1 drop in the morning and increase or pause, as tolerable. | 124 | AU | Onboarding (Severe) | 1 | https://www.metabolics.com/products/riboflavin-5-phosphate | (Sublingual) For onboarding Vitamin B2 with severe / neuropsychiatric symptoms susceptibility. | https://bornfree.life/learn/2-the-protocol/#severe | ||||||||||
| 390 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 23/11/2025 05:25 AM | [SEVERE ONLY] | Onboarding (Severe) | (Titrating) B6 / P5P | 1 | 1 | 1 | (Sublingual) Start at 1 drop in the morning and increase or pause, as tolerable.Start at 1 drop in the morning and increase or pause, as tolerable. | 125 | US | Onboarding (Severe) | 1 | https://www.metabolics.com/products/vitamin-b6-pyridoxal-5-phosphate | (Sulingual) For onboarding Vitamin B6 with severe / neuropsychiatric symptoms susceptibility. | https://bornfree.life/learn/2-the-protocol/#severe | ||||||||||
| 391 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 23/11/2025 05:25 AM | [SEVERE ONLY] | Onboarding (Severe) | (Titrating) B6 / P5P | 1 | 1 | 1 | (Sublingual) Start at 1 drop in the morning and increase or pause, as tolerable.Start at 1 drop in the morning and increase or pause, as tolerable. | 125 | EU | Onboarding (Severe) | 1 | https://www.metabolics.com/products/vitamin-b6-pyridoxal-5-phosphate | (Sulingual) For onboarding Vitamin B6 with severe / neuropsychiatric symptoms susceptibility. | https://bornfree.life/learn/2-the-protocol/#severe | ||||||||||
| 392 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 23/11/2025 05:25 AM | [SEVERE ONLY] | Onboarding (Severe) | (Titrating) B6 / P5P | 1 | 1 | 1 | (Sublingual) Start at 1 drop in the morning and increase or pause, as tolerable.Start at 1 drop in the morning and increase or pause, as tolerable. | 125 | AU | Onboarding (Severe) | 1 | https://www.metabolics.com/products/vitamin-b6-pyridoxal-5-phosphate | (Sulingual) For onboarding Vitamin B6 with severe / neuropsychiatric symptoms susceptibility. | https://bornfree.life/learn/2-the-protocol/#severe | ||||||||||
| 393 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 23/11/2025 05:25 AM | [SEVERE ONLY] | Onboarding (Severe) | (Titrating) B9 / Folinic Acid | 1 | 1 | 1 | Start at 1/10th of 1 drop (dissolve 1 drop in eg. 100ml water and use 1/10th of 100ml/day) in the morning and increase or pause, as tolerable. | 126 | US | Onboarding (Severe) | 1 | https://www.amazon.com/dp/B08FM5Y7JK/ | For onboarding Vitamin B9 with severe / neuropsychiatric symptoms susceptibility. | https://bornfree.life/learn/2-the-protocol/#severe | ||||||||||
| 394 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 23/11/2025 05:25 AM | [SEVERE ONLY] | Onboarding (Severe) | (Titrating) B9 / Folinic Acid | 1 | 1 | 1 | Start at 1/10th of 1 drop (dissolve 1 drop in eg. 100ml water and use 1/10th of 100ml/day) in the morning and increase or pause, as tolerable. | 126 | EU | Onboarding (Severe) | 1 | https://mandimart.eu/en-nl/products/folinic-acid-30mls-alcohol-free-by-california-gold-nutrition | For onboarding Vitamin B9 with severe / neuropsychiatric symptoms susceptibility. | https://bornfree.life/learn/2-the-protocol/#severe | ||||||||||
| 395 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 23/11/2025 05:25 AM | [SEVERE ONLY] | Onboarding (Severe) | (Titrating) B9 / Folinic Acid | 1 | 1 | 1 | Start at 1/10th of 1 drop (dissolve 1 drop in eg. 100ml water and use 1/10th of 100ml/day) in the morning and increase or pause, as tolerable. | 126 | AU | Onboarding (Severe) | 1 | https://alchepharma.com/products/folic-acid-667-mcg-folinate-yielding-400-mcg-of-folinic-acid-800-servings | For onboarding Vitamin B9 with severe / neuropsychiatric symptoms susceptibility. | https://bornfree.life/learn/2-the-protocol/#severe | ||||||||||
| 396 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 23/11/2025 05:25 AM | [SEVERE ONLY] | Onboarding (Severe) | (Titrating) B12 / Hydroxycobalamin | 1 | 1 | 1 | Start at 1 drop in the morning and increase or pause, as tolerable. | 127 | US | Onboarding (Severe) | 1 | https://www.metabolics.com/products/vitamin-b12-hydroxocobalamin | For onboarding Vitamin B12 with severe / neuropsychiatric symptoms susceptibility. | https://bornfree.life/learn/2-the-protocol/#severe | ||||||||||
| 397 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 23/11/2025 05:25 AM | [SEVERE ONLY] | Onboarding (Severe) | (Titrating) B12 / Hydroxycobalamin | 1 | 1 | 1 | Start at 1 drop in the morning and increase or pause, as tolerable. | 127 | EU | Onboarding (Severe) | 1 | https://www.metabolics.com/products/vitamin-b12-hydroxocobalamin | For onboarding Vitamin B12 with severe / neuropsychiatric symptoms susceptibility. | https://bornfree.life/learn/2-the-protocol/#severe | ||||||||||
| 398 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 05/03/2026 03:18 AM | [OTHER SUPPLEMENTS] | Supplements | Inosine | 1 | 1 | 500mg, 1x/day AM (start slowly, eg. 50-100mg, sublingually) | 128 | US | Supplements | 45g | https://purebulk.com/products/inosine?variant=41954108080325 | (Sublingual) Calms extracellular ATP "alarm signal" P2X7 purinergic relay / Cell Danger Response. Rescues TRPV1 in peripheral neuropathy | https://bornfree.life/learn/2-2-6-cortisol-limbic-system-glycogen/#phobic-loop | |||||||||||
| 399 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 05/03/2026 03:18 AM | [OTHER SUPPLEMENTS] | Supplements | Inosine | 1 | 1 | 500mg, 1x/day AM (start slowly, eg. 50-100mg, sublingually) | 128 | EU | Supplements | 45g | https://purebulk.com/products/inosine?variant=41954108080325 | (Sublingual) Calms extracellular ATP "alarm signal" P2X7 purinergic relay / Cell Danger Response. Rescues TRPV1 in peripheral neuropathy | https://bornfree.life/learn/2-2-6-cortisol-limbic-system-glycogen/#phobic-loop | |||||||||||
| 400 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 05/03/2026 03:18 AM | [OTHER SUPPLEMENTS] | Supplements | Inosine | 1 | 1 | 500mg, 1x/day AM (start slowly, eg. 50-100mg, sublingually) | 128 | AU | Supplements | 45g | https://purebulk.com/products/inosine?variant=41954108080325 | (Sublingual) Calms extracellular ATP "alarm signal" P2X7 purinergic relay / Cell Danger Response. Rescues TRPV1 in peripheral neuropathy | https://bornfree.life/learn/2-2-6-cortisol-limbic-system-glycogen/#phobic-loop | |||||||||||
| 401 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 06/03/2026 10:07 PM | [DIY SHAKE] | Supplements | Resveratrol | 1.5-10.5g | 10.5g | 10.5g | If substituting - note differences between trans-resveratrol and resveratrol (use trans-resveratrol at 50% dose). | 1 | 1 | Start slowly, eg. 50mg, x3/day and increase to 500mg per dose. PDH kinase inhibition to help protect against lactic acid excess with improved glycolysis flux vs TCA cycle. | 129 | US | Supplements | 135g | https://www.bulksupplements.com/products/resveratrol-pure?variant=32133451186287 | Start slowly. PDH kinase inhibition to help protect against lactic acid excess with improved glycolysis flux vs TCA cycle.. Additional benefits for ALDH, dopamine and microbiome. | https://bornfree.life/learn/4-3-diy-powder | |||||||
| 402 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 06/03/2026 10:07 PM | [DIY SHAKE] | Supplements | Resveratrol | 1.5-10.5g | 10.5g | 10.5g | If substituting - note differences between trans-resveratrol and resveratrol (use trans-resveratrol at 50% dose). | 1 | 1 | Start slowly, eg. 50mg, x3/day and increase to 500mg per dose. PDH kinase inhibition to help protect against lactic acid excess with improved glycolysis flux vs TCA cycle. | 129 | EU | Supplements | 135g | https://www.bulksupplements.com/products/resveratrol-pure?variant=32133451186287 | Start slowly. PDH kinase inhibition to help protect against lactic acid excess with improved glycolysis flux vs TCA cycle.. Additional benefits for ALDH, dopamine and microbiome. | https://bornfree.life/learn/4-3-diy-powder | |||||||
| 403 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 06/03/2026 10:07 PM | [DIY SHAKE] | Supplements | Resveratrol | 1.5-10.5g | 10.5g | 10.5g | If substituting - note differences between trans-resveratrol and resveratrol (use trans-resveratrol at 50% dose). | 1 | 1 | Start slowly, eg. 50mg, x3/day and increase to 500mg per dose. PDH kinase inhibition to help protect against lactic acid excess with improved glycolysis flux vs TCA cycle. | 129 | AU | Supplements | 135g | https://www.bulksupplements.com/products/resveratrol-pure?variant=32133451186287 | Start slowly. PDH kinase inhibition to help protect against lactic acid excess with improved glycolysis flux vs TCA cycle.. Additional benefits for ALDH, dopamine and microbiome. | https://bornfree.life/learn/4-3-diy-powder | |||||||
| 404 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 19/01/2026 03:27 AM | [REPLETION] | Minerals | Strontium | 1 | 1 | May be stimulating. Test a small dose, by opening the capsule and using a fraction.. | 130 | US | Minerals | 1 | https://iherb.com/pr/life-extension-strontium-caps-90-vegetarian-capsules-250-mg-per-capsule/29332 | (Optional) Bone health. Often missing in restricted diets. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 405 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 19/01/2026 03:27 AM | [REPLETION] | Minerals | Strontium | 1 | 1 | May be stimulating. Test a small dose, by opening the capsule and using a fraction.. | 130 | EU | Minerals | 1 | https://iherb.com/pr/life-extension-strontium-caps-90-vegetarian-capsules-250-mg-per-capsule/29332 | (Optional) Bone health. Often missing in restricted diets. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 406 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 19/01/2026 03:27 AM | [REPLETION] | Minerals | Strontium | 1 | 1 | May be stimulating. Test a small dose, by opening the capsule and using a fraction.. | 130 | AU | Minerals | 1 | https://iherb.com/pr/life-extension-strontium-caps-90-vegetarian-capsules-250-mg-per-capsule/29332 | (Optional) Bone health. Often missing in restricted diets. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 407 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 19/01/2026 03:35 AM | [REPLETION] | Minerals | Boron | 1 | 1 | (Sublingual) 6mg/day. Ideally non-oral route required. Fillers will not absorb sublingually.. | 131 | US | Minerals | 1 | https://iherb.com/pr/now-foods-boron-3-mg-250-veg-capsules/428 | (Sublingual) Calcium and magnesium retention, hormone synthesis, broad other benefits. Oral route converts into boric acid (see antiseptic) and glycine in the gut. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 408 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 19/01/2026 03:35 AM | [REPLETION] | Minerals | Boron | 1 | 1 | (Sublingual) 6mg/day. Ideally non-oral route required. Fillers will not absorb sublingually.. | 131 | EU | Minerals | 1 | https://iherb.com/pr/now-foods-boron-3-mg-250-veg-capsules/428 | (Sublingual) Calcium and magnesium retention, hormone synthesis, broad other benefits. Oral route converts into boric acid (see antiseptic) and glycine in the gut. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| 409 | 3dghs | 10/08/2024 09:44 AM | 3dghs2 | 19/01/2026 03:35 AM | [REPLETION] | Minerals | Boron | 1 | 1 | (Sublingual) 6mg/day. Ideally non-oral route required. Fillers will not absorb sublingually.. | 131 | AU | Minerals | 1 | https://iherb.com/pr/now-foods-boron-3-mg-250-veg-capsules/428 | (Sublingual) Calcium and magnesium retention, hormone synthesis, broad other benefits. Oral route converts into boric acid (see antiseptic) and glycine in the gut. | https://bornfree.life/learn/2-3-2-remineralisation/ | |||||||||||
| region |