https://www.ncbi.nlm.nih.gov/books/NBK513346/
Much like in alcohol dependence, individuals with SIBO may experience metabolic impairments due to the fermentation of sugars into alcohol and acetaldehyde within the gut. This process can disrupt homeostasis, precisely mimicking the metabolic challenges faced by chronic alcohol users.
When treating alcoholism, the typical approach involves gradually reducing alcohol intake, supported by high doses of thiamine (Vitamin B1) and large amounts of Vitamin C. In addition, psychological counseling is often recommended as part of the recovery process
https://pmc.ncbi.nlm.nih.gov/articles/PMC8302359/
In some cases, doctors may prescribe Naltrexone, a medication that can help regulate dopamine and GABA metabolism, offering relief from alcohol cravings. Naltrexone has additional benefits beyond this primary use, such as improving mood and reducing anxiety - however there are some additional benefits.
https://pmc.ncbi.nlm.nih.gov/articles/PMC2565602/
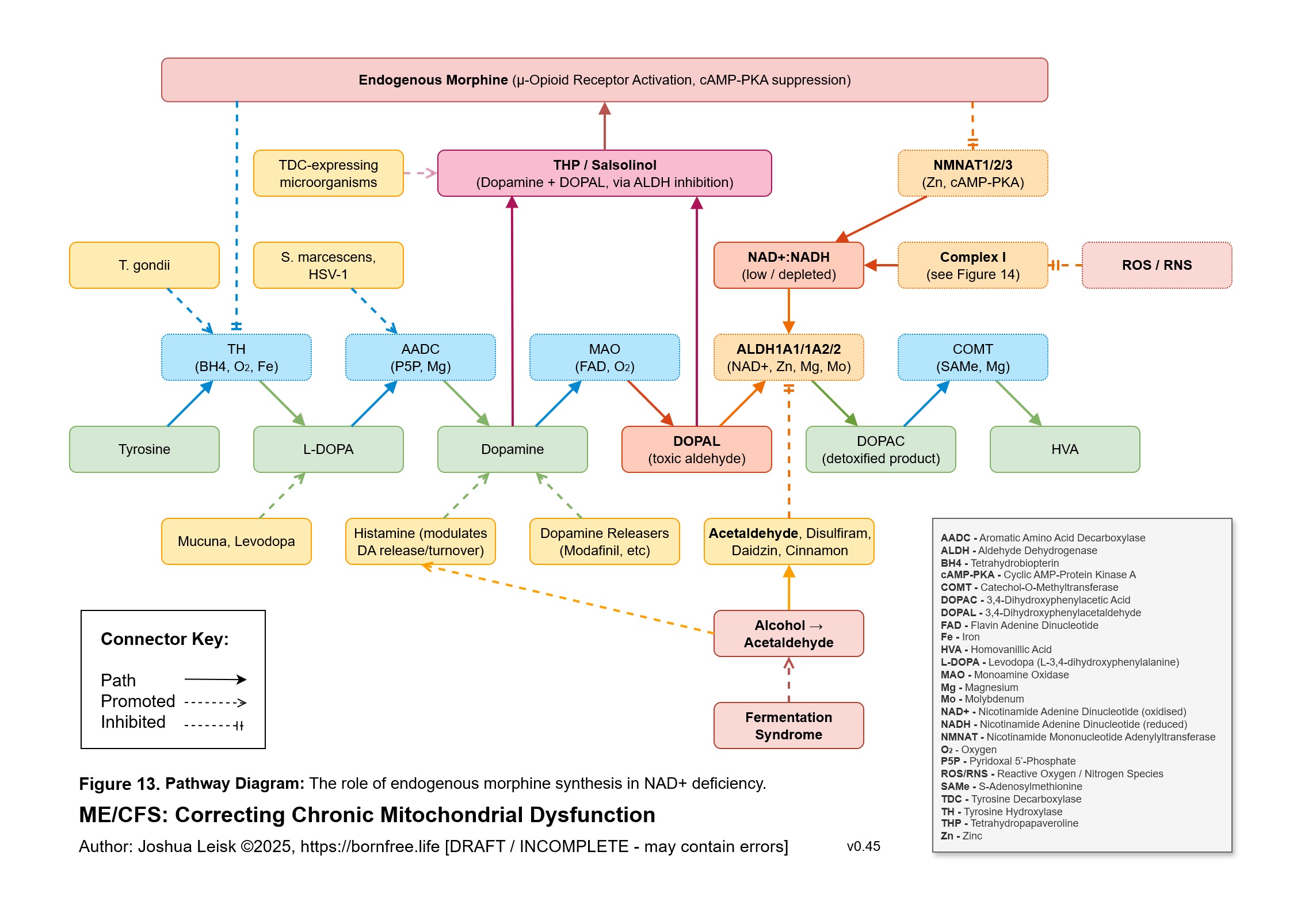
What has not been fully understood or appreciated is that alcohol -> acetaldehyde elevation further elevates endogenous synthesis of morphine, codeine and gamma-hydroxybutyrate (GHB), as can severe and chronic Complex I inhibition. Both acetaldehyde and Complex I inhibition are commonly observed in collected ME/CFS data.
For endogenous morphine and codeine synthesis, the mechanism is related to dopamine metabolism. When ALDH1A1 and/or ALDH2 are inhibited, elevated dopamine and DOPAL cause an elevation of Tetrahydropapaveroline (THP) (also known as (S)-norlaudanosoline), which is the first step in the morphine biosynthesis pathway. This altered metabolism leads to behavioural changes that overlap ADHD, coupled with homeostasis alterations and dependence .
https://onlinelibrary.wiley.com/doi/10.1111/j.1755-5949.2009.00114.x
https://www.pnas.org/doi/10.1073/pnas.050324410
https://www.science.org/doi/10.1126/science.557839
THP has also been observed in Alzheimer's and Parkinson's disease patients, however the model suggests it will be found in numerous others. Morphine and DHMA has been observed in collected data by younger members of the Born Free community, without any exogenous use.
https://www.mdpi.com/1420-3049/28/5/2166
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3560700/
https://pubmed.ncbi.nlm.nih.gov/1545408/
Naltrexone, particularly in its low-dose form (LDN), is a well-known therapeutic intervention for managing opioid use disorder. It is also increasingly used to treat conditions such as Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS), Long COVID, and Post-Vaccine Syndrome. The disease model suggests additional mechanisms for its observed therapeutic benefits.
https://pubmed.ncbi.nlm.nih.gov/38267326/
The body’s production of gamma-hydroxybutyrate (GHB) is linked to changes in GABA metabolism through a process connected to the GABA shunt. In this pathway, GABA is normally converted into succinic acid via an intermediate called succinic semialdehyde (SSAL). However, when the enzyme ALDH5A1 is inhibited, often due to low NAD+ levels, while NADPH levels are elevated, SSAL is instead metabolized into GHB.
https://www.ncbi.nlm.nih.gov/books/NBK1195/
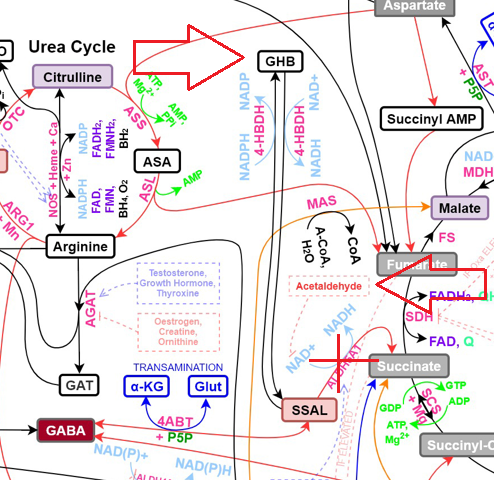
GHB is marker #75 on the OAT results and is often quite elevated in more severe patients:

As we gain a better understanding of how the gut microbiome interacts with these metabolic processes, it becomes crucial to anticipate potential withdrawal symptoms during microbiome remodelling. A rapid improvement in gut health, especially after a significant dietary shift or use of antimicrobials and/or biofilm breakers, can lead to sudden withdrawal from multiple endogenous narcotics. This is expected when introducing low-dose methylene blue in Stage 1 and also during Stage 2 of the protocol, where removing acetaldehyde producing species is the primary focus.
The more rapidly any successful gut fermentation syndrome remediation is performed, the more likely that someone will go into rapid withdrawal symptoms for multiple simultaneous narcotics. Microdosing methylene blue to provide alternative Complex I functions and restore NAD+ redox is a reliable trigger.
For instance, transitioning to a ketogenic diet or using antimicrobials can trigger an initial wave of endotoxaemia (toxins released from dying bacteria), which may temporarily suppress withdrawal symptoms. However, as microbial production of alcohol and its byproduct acetaldehyde decreases, there is a corresponding reduction in the synthesis of morphine and GHB. This may result in metabolism and symptoms expected during chronic alcohol, opioid, and GHB withdrawal, which can peak about a week after significant microbiome changes.
Depending on the significance of the alcohol / endogenous narcotic reduction, symptoms may include any of:
Insomnia, Low Liver Glycogen - Nausea and Vomiting, Sweating, (severe) Fatigue, Hypothermia (low body temperature), Diarrhea, Abdominal Cramping, Hypometabolism, Tremors, Tachycardia (rapid heartbeat), Muscle Aches/Cramps, Seizures, Hypertension (high blood pressure), Anxiety, Agitation, Panic, Terror, Reduced Motivation, Difficulty Concentrating, Hallucinations, Delirium/Confusion, Depressed Mood, Psychosis, Yawning, Goosebumps (piloerection), Runny Nose (rhinorrhea), Lacrimation (tearing), Dilated Pupils, Internal Vibrations, "Band Around Head" Pressure (warning, this is an indication for severe withdrawal, ahead of seizures).
The symptoms are largely relating to cAMP-PKA-CREB homeostasis, can be potentially life-threatening / self-harm inducing and are expected to appear and disappear multiple times over typically 2-3 weeks, like a swinging pendulum over-shooting, on its way back to the center, where homeostasis is restored (see Figure 18 on the disease model page for additional information).
With each swing, one direction has a "drugged" feeling (low cAMP-PKA tone) and the other direction includes panic, depression, elevated heart-rate, insomnia, etc. (elevated cAMP-PKA tone). Hormonal status greatly controls this pathway and for females, it would be distinctly advantageous to start any endogenous opioid withdrawal process just after menses. Oestradiol amplifies excessive cAMP signalling and progesterone calms it. During excessive cAMP signalling, any adrenergic triggers will be amplified - small signals can easily become panic, terror and spiralling. This may also explain why women suffer from neuropsychiatric symptoms manifest at different stages of their menstrual cycle (pre-ovulation and luteal phase) and why they are more likely to suffer when this pathway loses homeostasis than men, generally. More understanding and empathy around this could help inform appropriate patient care.
As this process usually accompanies restored NAD+ pool status, being the primary currency and sensor for cortisol's regulation of innate immune activity (XO, and NOS, NOX - via further NAD+ conversion to NADPH), it's expected that any tissue with an active infection or tissue repair functions orchestrated by IFN-gamma activity will flare with inflammation and pain. This can feed into adrenergic signalling to promote cAMP.
Both of these processes can be "cushioned" and managed to make them tolerable.
Ironically, the logical solution is fairly simple, although it may understandably raise some initial concerns.
It has often been said that "alcohol is the cause of and solution to all of life's problems" and never more literally than in this instance.
This observation has been shared by various well-known people with ME/CFS and related online groups such as https://www.reddit.com/r/hangovereffect/.
Although this author's opinion is bound to attract some criticism, I'd also advocate that using exogenous alcohol, as an over-the-counter tapering schedule against withdrawal from the microbial-sourced alcohol (and the 2 downstream endogenous psychoactive substances) is a far simpler and less problematic therapeutic intervention than administering exogenous opioids and/or benzodiazepines, in an attempt to create an effective tapering schedule.
These 2 classes of drugs are both well-known to be "drugs of dependence" and will likely require high doses to be effective symptomatically. High doses of these interventions can create a long tapering schedule of their own that may last 6 months to a year and is known to be highly unpleasant.
Following a strict alcohol tapering schedule and avoiding dosing at levels which induce alcoholic intoxication is required. The goal is to remain in a tolerable level of withdrawal symptoms during the taper, rather than attempting to make the process "feel pleasurable" and extending the process. This will be highly personalised and likely involve multiple doses over the day / night, which decrease over time. Having appropriate monitoring and management would be highly advisable.
Caveats and Risks
1) It would be optimal to avoid alcohol reaching the gut microbiome.
Neat alcohol such as gin, vodka or whiskey, when taken in small sips
and absorbed largely via the mucous membranes found in the mouth, throat
and oesophagus would be a preferred route of administration. These can be attempted at 1/2 a "typical" drink, eg. 15ml of neat spirits, or 1/2 a beer / wine / cider, etc. and allow 20-30 minutes to test if stability / relief has been achieved.
2) While alcohol add-back therapy is known to be problematic in chronic alcohol use withdrawal due to the risk of behavioral disorders, such issues are less likely to arise in conditions like ME/CFS or Long COVID where alcohol consumption was not voluntary or habitual. However, professional oversight and adequate peer support is still recommended to manage the process effectively and provide a safety-net.
Cinnamon contains compounds which also inhibit ALDH and can provide some tapering support for a few hours per dose. Effective dosing ranges may span from 1/10th to 1 teaspoon of cinnamon powder.
NB. Excess amounts of cinnamon can trigger a "drugged" or "drunk" feeling.
In addition to alcohol tapering, certain supplements may also help manage withdrawal symptoms relating to hyper-metabolism / panic / depression / insomnia during rebound excess cAMP signalling.
These include:
1. Tiny doses of bacopa, eg. 25-50mg active bacosides to modulate CREB and without spiking cAMP. NB. Higher doses flip the other way and exacerbate symptoms.
2. Lithium sufficiency to inhibit GSK-3beta and promote CREB.
3. Low doses of progesterone, eg. 10-50mg, to calm cAMP and promote CREB.
4. Progesterone > oestradiol balance modulators, like chasteberry.
5. Ivabradine, low dose propranolol, etc.
6. 0.5-1.5g of L-theanine, multiple times per day, to antagonise glutamate signalling.
7. Carbohydrates, uridine monophosphate. phosphate and magnesium sufficiency to promote glycogen synthesis and help negate cAMP spikes -> PEM, POTS, etc.
Other influences:
1. Insulin spikes lower cAMP (perhaps explaining "stress-eating").
2. Post-orgasmic period lowers catecholamines, reducing adrenergic signalling (perhaps explaining part of the ADHD "hypersexual" behaviour as a soothing / stress-regulating mechanism).
Various foods, drugs and supplements that promote beta-adrenergic signalling, or cAMP, or inhibit PDE will significantly exacerbate any rebound excess cAMP symptoms and should be avoided / managed appropriately during the "adrenergic excess and insomnia" side of the "pendulum swing".
These include:
1. Forskolin (cAMP promoter).
2. Yohimbe / yohimbine, rauwolscine (indirect cAMP promoters).
3. Caffeine (cAMP promoter).
4. Hesperidin and some formulations of other citrus bioflavonoids like quercetin (PDE inhibitor).
5. Luteolin (PDE inhibitor).
6. Boswellia (cAMP promoter, PDE inhibitor).
7. Cialis, viagra and related drugs (PDE inhibitors).
8. SNRIs and/or exogenous cortisone dosing may need reduction.
NB. While removing methylated B9 and B12 *can* "pull the fuse" on SAMe synthesis (needed for PNMT and epinephrine levels), this also affects a wide array of other important enzymes and leads to decline, histamine sensitivity, etc. This is not advisable except as an emergency and temporary measure.
Some effects of chronic opioid use will take many months to fully recover. Many of the related studies were conducted on heroin users and may not reflect the prognosis for someone actively supporting mineral status and other variables.
Overall, the withdrawal process is unpleasant, but manageable with the right tools and is essential to recovery.