Acetaldehyde is one of the primary toxins released during microbial die-off events and also in smaller amounts, multiple times per day, in response to normal dietary intake of nutrients. Our food intake also feeds our resident microorganisms – including the pathogenic species – which allows them to produce (toxic) metabolites and poison us following each meal.
Acetaldehyde potentially places a difficult burden on our metabolism in key places – histamine degradation, neurotransmitter degradation, collagen synthesis, carnitine synthesis (needed to transport longer chain fatty acids), fatty acid degradation, glucose transport and glycolysis, GABA metabolism, choline metabolism, methylation, vitamin B6 degradation, vitamin A metabolism, lysine degradation, pyruvate metabolism and many other pathways.
Countering that, in appropriate doses, it appears to function as an antidepressant - by slowing down the neurotransmitter degradation pathway and triggering endogenous morphine + GHB synthesis. (see 2.3.4 Rapid withdrawal)
It also functions as an exertion mimetic, by increasing the mitochondrial NADH pool level for Complex I to take electrons from and feed the electron transport chain. (see 2.2.4 The importance of pacing and Figure 14)
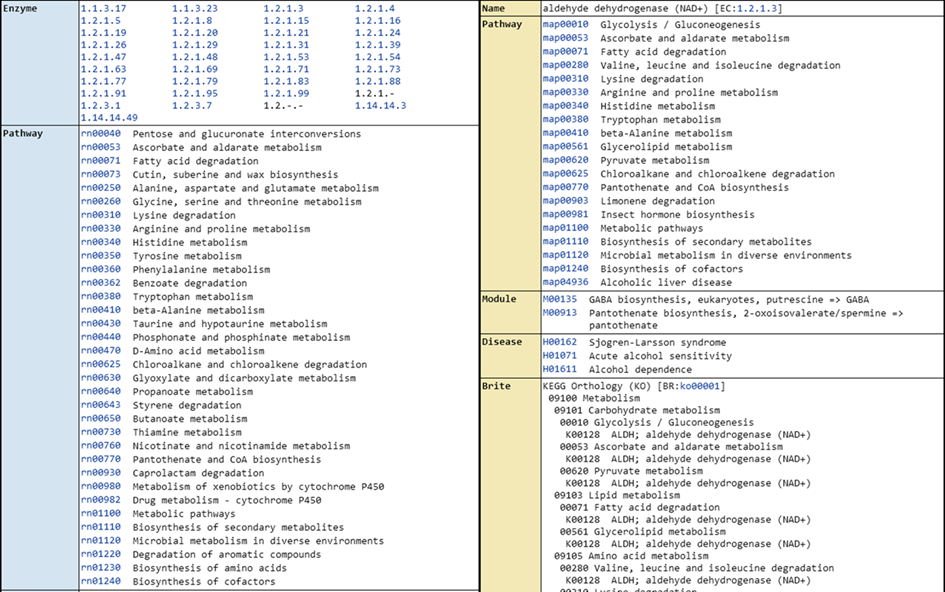
Aldehyde dehydrogenase enzymes (ALDH2, 1A1, 1A2, etc.) detoxify acetaldehyde into acetate as a priority over their normal substrates due to the kinetics involved. This means that these enzymes are the primarily affected reactions by chronic acetaldehyde and this will initially create a number of metabolic impairments to important pathways. This may be observed as eg. elevated LDL cholesterol, elevated serum vitamin B6, elevated histamine, elevated retinol / beta-carotene and an array of symptoms.
However, having low NAD+ as a result of chronic IFN-γ
activity, and/or
inhibited NMNAT activity (eg. low cAMP-PKA, oestradiol, MAPK)
exacerbates this problem significantly, creating a loop / trap and extends the impact to a wide
range of important enzymes requiring NAD+ as a cofactor.
As ALDH normally requires NAD+ (and magnesium, zinc), this also includes the majority of ALDH isoforms, affecting a wider array of aldehyde metabolism.
Taurine, NAD+, magnesium, zinc and molybdenum help promote ALDH activity and restore normal metabolism. Cultivating acetaldehyde metabolising probiotic species like bifidobacterium and reducing acetaldehyde producing species is the long-term goal, however using one of these short-term interventions can be very helpful pre-meal and during die-off:
Some generally helpful intervention options:
Thiamine - the thiazolium/N-heterocyclic carbene of thiamine (or thiamine pyrophosphate (TPP) / cocarboxylase) catalyses self-condensation of two acetaldehyde molecules to acetoin and can then be further reduced to 2,3-butanediol. This process is catalytic, not stoichiometric and needs an alkaline environment. Without sufficient acetaldehyde metabolism support or large doses of thiamine (often grams), expect decreased cellular TPP availability.
Glutathione - creates a nucleophilic attack of the cysteinyl thiol on carbonyl carbon, making S-Hydroxyethyl-glutathione. Creates up to to four adducts per tripeptide and requires adequate glutathione reductase activity to be sustainable. Chronic acetaldehyde / low zinc throttles this route, via low active riboflavin (FAD). Typically dosed at around 250mg.
Kislip - https://ase-onlinestore.com/products-list/asetablet-1box/ (Worldwide shipping, from Japan)
L- Carnosine - can be used at 100mg - 1g, with meals / die-off. (Being explored as a standard inclusion for future updates. Careful, if being used where zinc is still low / methylation otherwise impaired, as excess carnosine is a precursor for histidine and is normally degraded by SAMe-requiring enzymes.)
(USA / Worldwide) - https://www.bulksupplements.com/products/l-carnosine
(AU) - https://aminonutrition.com.au/products/carnosine
(EU) - https://www.amazon.de/dp/B09CH8V6S5
ZBiotics - https://zbiotics.com/products/zbiotics (Perhaps too expensive for daily use)
NAC - small amounts after meals are now included in the DIY Sipper recipe and help remove acetaldehyde.
DHM - now included in Stage 1, though additional amounts can be taken. It promotes ALDH, however this still requires NAD+ and mineral sufficiency.
Binders - Silicon binds acetaldehyde and is included in Stage 1, however you can find a table of binders for multiple purposes in 2.2.3 - Binders.
Methylene Blue - "A lifeguard for the NAD+ pool"
Methylene blue is one of the oldest synthetic medicines still in clinical use. Heinrich Caro first prepared it in 1876 for BASF as a textile dye. Fifteen years later Paul Ehrlich gave it to malaria patients, launching modern chemotherapy, and within another decade anaesthetists were using it to reverse drug-induced methaemoglobinaemia. Over the following century the dye turned up in bacteriology labs, psychiatry wards and, more recently, neurodegeneration trials.
Before implementing anything from this section, it's very important to understand that rapidly correctly a severe NAD+ or chronic acetaldehyde issue can create rapid withdrawal symptoms, mirroring those seen in alcohol and opioid use disorders.
Do not start microdosing methylene blue without first reading and preparing for this withdrawal process. (See "2.3.4 Rapid withdrawal, hypo/hypermetabolism".)
At nanomolar concentrations methylene blue slips into mitochondria and behaves like an auxiliary wire in the electron-transport chain. It accepts electrons from NADH then hands them to cytochrome c, restoring the NAD⁺∶NADH ratio, raising Complex IV activity and trimming reactive-oxygen leakage. In human fibroblasts 100 nM postponed senescence by roughly fifty per cent and boosted ATP production, a finding revisited many times since the original Atamna-Ames work.
Picture the respiratory chain as an electrical harness running across the inner mitochondrial membrane. Normally electrons step down that harness from NADH into Complex I, then through ubiquinone to Complex III, finally jumping onto cytochrome c before sliding into Complex IV and oxygen. When Complex I is inhibited by eg. chronic innate immune response and/or oxidative stress, the first hand-off stalls, the upstream NAD⁺ pool shrinks and everything requiring it as a cofactor idles.
Methylene blue slips in as a short jumper wire bridging the break. In the matrix the oxidised dye (MB⁺) meets an NADH-dependent flavoprotein such as NQO1 or a nonspecific diaphorase. The flavin passes two electrons and a proton to the dye:
NADH + H⁺ + MB⁺ → NAD⁺ + leucomethylene blue (MBH₂)
Leucomethylene blue is colourless, lipophilic and diffuses toward the inter-membrane face where oxidised cytochrome c is waiting. Because the MBH₂/MB⁺ redox pair sits at about +10 mV while the Fe³⁺/Fe²⁺ couple of cytochrome c sits at +260 mV, the electron drop is energetically downhill:
MBH₂ + 2 cytochrome c(Fe³⁺) → MB⁺ + 2 cytochrome c(Fe²⁺) + 2 H⁺
Oxidised methylene blue is now ready to shuttle back for another round; reduced cytochrome c hands its electrons to Complex IV just as if they had come through Complex III. Proton pumping at Complex IV continues, ATP synthase turns, and, crucially, NAD⁺ is regenerated inside the matrix even though Complex I never fired.
At the nanomolar doses used for redox support the cycle is gentle: the flavoprotein step limits the rate, so electrons leak only minimally to oxygen, avoiding significant superoxide. However, increase the concentration into higher single-digit micromolar and our jumper wire becomes a redox treadmill. MB accepts electrons faster than cytochrome c can take them, spills some to molecular oxygen and the extra reactive oxygen species flip the dye from helper to hazard.
(This concentration is also protective against glutamate excitotoxicity.)
In short, the “auxiliary wire” reaction is a two-stroke shuttle: NADH reduces methylene blue, methylene blue reduces cytochrome c, and the dye recycles. It restores the NAD⁺:NADH ratio and keeps oxidative phosphorylation alive without relying on a poorly-performing Complex I. You could consider micro-doses of methylene blue as a Complex I analogue.
However, once plasma levels climb into the low-micromolar bracket the story changes. Around one micromolar plasma concentrations, the dye becomes a potent reversible inhibitor of monoamine-oxidase A; that action has been explored for depression but also explains why high doses can trigger serotonin toxicity if mixed with SSRIs. Push it further, especially with light activation, and methylene blue behaves as a photosensitising antimicrobial, generating singlet oxygen lethal to bacteria and some parasites. At the top of the range, an intravenous bolus of one to two milligrams per kilogram is the standard antidote for life-threatening methaemoglobinaemia because the reduced form, leucomethylene blue, donates electrons directly to ferric haem.
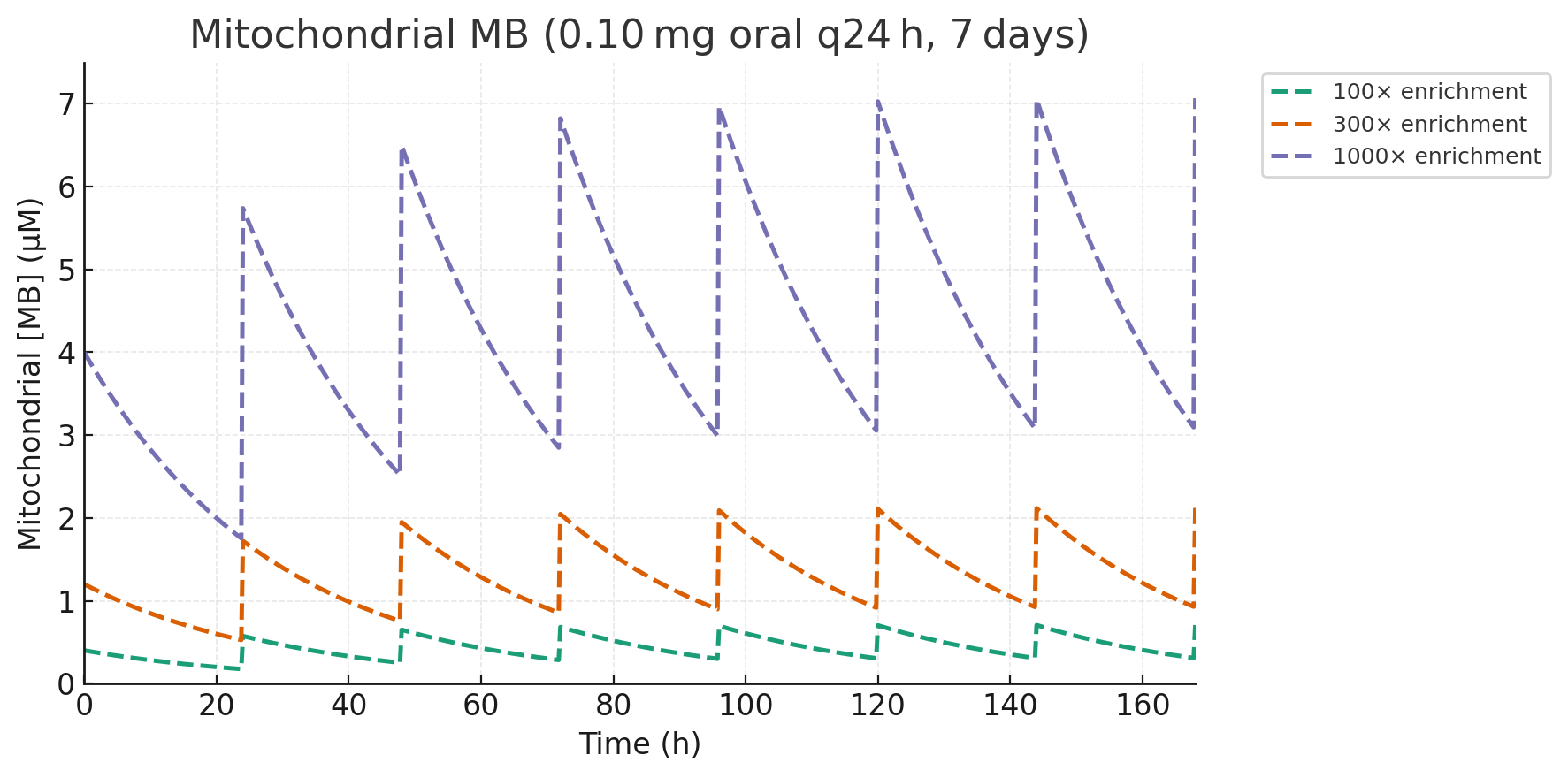
Methylene blue is a lipophilic monocation. As soon as it reaches the bloodstream it starts migrating down every negative membrane potential it can find, the steepest of which is the -150 to -180 mV drop across the inner mitochondrial membrane. One proton motive force equals roughly tenfold enrichment for a monovalent cation per 60 mV, so a healthy mitochondrion will concentrate MB by 100-to 1000-fold, relative to free plasma.
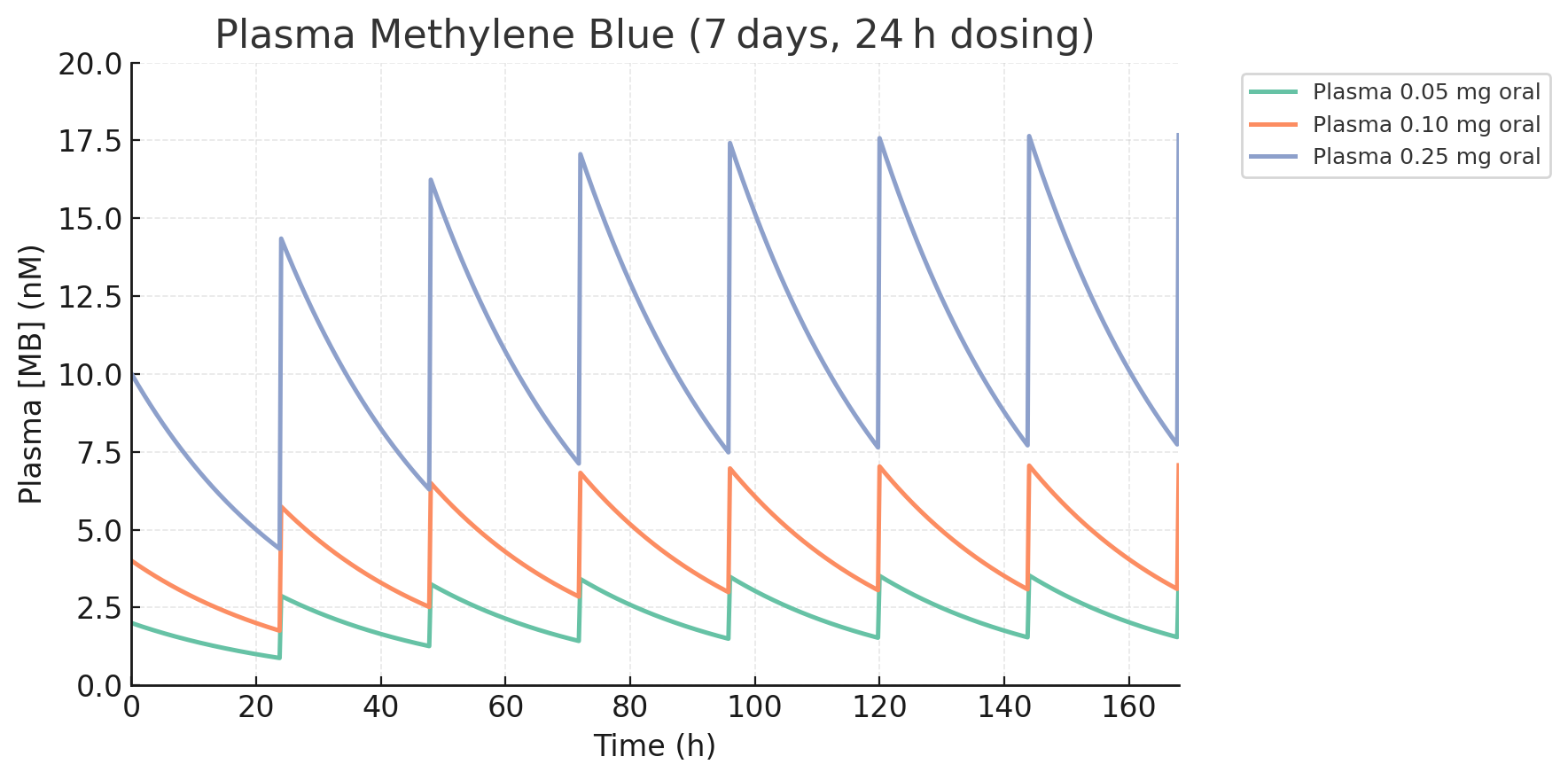
Low-dose pharmacokinetic work in healthy volunteers is uncomplicated and
linear up to about 20 mg. A 1 mg immediate-release capsule yields a
peak plasma concentration (Cmax) of roughly 40 nM
within an hour, and a half-life of five hours for the fast distribution
phase followed by a terminal half-life of fifteen to twenty-four hours.
Scale the dose down and the numbers scale with it. A 0.5 mg dose tops
out at about 20 nM, while a 25 µg “pin-prick” dose peaks at a whisker
under 1 nM. Roughly forty per cent is excreted unchanged in the urine,
which turns a striking blue-green that can dye test strips and,
occasionally, the toilet bowl when used at much higher doses.
Translate those plasma numbers across the membrane potential and life inside the mitochondrial matrix looks very different. Even with a conservative 100-fold enrichment, for unhealthy
mitochondria, a 0.1 mg dose drives mitochondrial matrix MB to about 0.7
µM. For healthy mitochondria, at the more usual 1 000-fold it hovers
around 7 µM, which is just skirting the threshold where things start
becoming quite unhelpful. At 10 µM, ALDH2 will be inhibited by
approximately 30%.
However, this creates a new challenge, as the
goalposts are going to move once we introduce methylene blue (and
restore active B vitamin metabolites, CoQ10, etc), as the mitochondria
will be expected to shift from an unhealthy to a healthy state. The
concentration of methylene blue inside the mitochondrial matrix may
increase ten-fold. This means the dose will normally need to be
decreased, as mitochondrial health improves. What starts as a
functional 0.1 - 0.25mg oral dose, once per day may decrease to 0.05 -
0.1mg per day, over the first week of introducing it.
Above 0.25 mg of MB per day, the mitochondrial concentration can become
orders of magnitude above the 100 nM threshold associated with redox
shuttling, glutathione support and mild neuroprotection. As the proton
gradient is preserved, wash-out is slow, giving a useful rule of thumb -
anything that peaks at 10 nM in plasma keeps the mitochondrial concentration above 100 nM for close to one day.
Most adverse effects are concentration-dependent. Sub-milligram doses of MB may sharpen working memory yet rarely colour the urine or stools. At the other end of the scale, taking >20mg+ doses invites strong ALDH inhibition, nausea, AChE inhibition, headache, dizziness and well beyond the threshold for MAO-linked serotonin risk, while glucose-6-phosphate-dehydrogenase deficiency introduces a theoretical chance of haemolysis, though recent malaria trials found that clinically insignificant. There are a range of dose-dependent applications, in between.
When working with MB, spills happen. Fresh stains fade if they are dabbed with three per cent hydrogen peroxide, which reduces the dye to its colourless leuco form. Rinse quickly, because exposure to air re-oxidises the molecule and the blue returns; a second peroxide round usually finishes the job.
Relating to this section of the protocol, for acetaldehyde metabolism and NAD⁺ redox support, methylene blue is best dosed inside a rather narrow window. 0.05 - 0.1 milligram oral doses in water are enough to ferry electrons from NADH to cytochrome c, even when Complex I is inhibited. The 0.1mg per day end of the range is more appropriate for unhealthy mitochondria and 0.05mg is more appropriate as they improve.
NB. Taking methylene blue at this dose range can rapidly remove the NAD+ redox bottleneck. At higher doses it will do the opposite and inhibit ALDH2.
Restoring NAD+ and ALDH activity can quickly restore part of the neurotransmitter degradation pathway, so caution should be taken and expect a mood dip. This should be added only in conjunction with interventions to restore the synthesis pathway in a balanced fashion, or a longer net decrease in neurotransmitters may be experienced - creating energy, sleep and emotional dysregulation, before homeostasis is restored. (see: pre-protocol support)
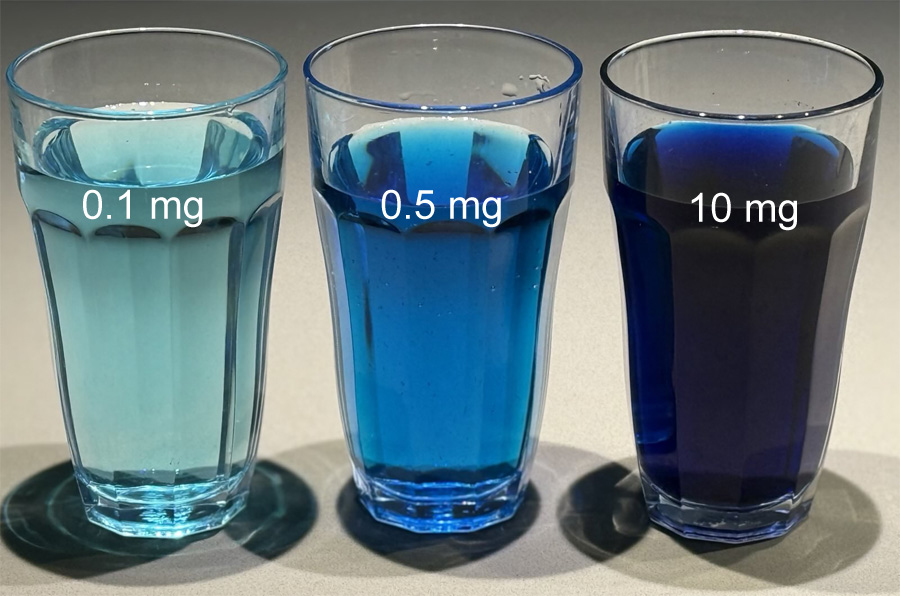
Using 1% methylene blue (MB), 1 single drop is 0.5mg. This is already 5-10x the target daily dose for most people. We'll need to convert the 1% solution into a 0.1% solution, to make it quick and easy to use.
There are multiple ways to achieve this:
1) Dropper bottle
(More initial setup, maximum convenience)You'll need one of the empty dropper bottles and a larger syringes described in 5 Ordering supplements. The empty dropper bottles listed can hold up to 60mL, however smaller batches may be preferable. In this example, we'll make up a 30mL bottle:
Boil and cool some clean water. Pour some into a glass. We'll only need 27mL of this in a future step.
Using the 1% MB dropper bottle as a source, add 60 drops (3mL, being 10% of the target total solution) into the empty dropper bottle.
Using the syringe, draw up a total of 27mL of boiled and cooled water and squirt it into the same dropper bottle you added the 1% MB to in the previous step.
Screw the cap on the finished bottle and shake it for 10 seconds.
USAGE: 1 drop from your finished bottle now contains 50mcg / 0.05mg and the bottle contains 600 doses. Add desired dose to a glass of water and consume.
2) Water bottle
(Minimal setup, more long-term effort)Adding 1 drop of 1% MB into a (eg. 1L) bottle of water will mean that 1/10th (100mL) of that blue water is now 50mcg / 0.05mg. Any bottle size works, providing you use 1/10th of the total, eg. a 25ml serving is 1/10th of a 250ml bottle.
USAGE: Pour 1/10th of the total solution volume into a glass, per desired 50mcg dose and consume. You can use kitchen scales to measure a serving, where 1g = 1mL of water.
3) Syringe
(Fast, but fiddly - not ideal)As 1 drop = 0.05mL, it could be dropped into an empty glass and drawn up in a 1mL or 10mL syringe. By filling the rest of the syringe with clean water, every 1/10th of the syringe is 50mcg / 0.05mg of MB.
USAGE: Add 1/10th of the syringe content to a glass of water, per 50mcg/ 0.05mg of desired dose and consume.
Some example doses in 250mL of water, to help confirm your product label / dosing accuracy:
"1% USP Methylene Blue" can be found in 5 Ordering supplements.
By supporting the NAD⁺ pool without consuming it, the dye helps ALDH5A1 clear succinic semialdehyde and keeps ALDH2 from stalling, which in turn eases the brain fog that comes from endogenous GHB and tetrahydropapaveroline. Acetaldehyde and histamine metabolism will see benefits, along with neurotransmitters, energy and other important metabolism.
Successfully deployed, methylene blue may be able to negate a number of interventions supporting metabolism downstream of NAD+ deficiency and ALDH inhibition, depending on mineral status. This may be reflected in future updates.
Again, an important reminder that rapidly correctly a severe NAD+ or chronic acetaldehyde issue can create rapid withdrawal symptoms, mirroring those seen in alcohol and opioid use disorders. It is best to introduce any acetaldehyde scavenging interventions for fermenting "food-in-transit" SLOWLY. Use for Herxheimer-related acetaldehyde spikes is more flexible.
Known limitations:
There is a small subset of people with confirmed acetaldehyde markers, Complex I inhibition and significant unresolved oxidative stress issues which don't respond to microdosing methylene blue at 50mcg, or experience the normally expected endogenous morphine withdrawal symptoms.
The described methylene blue microdose appears to be "used" by the reactive oxygen species (ROS) before providing the described mitochondrial benefits.
This subset of people may also test positive for MetHb and further testing via standard pathology into the location of the ROS could prove very helpful, eg. urinary F2-isoprostanes or s-nitrotyrosine for systemic lipid peroxidation, ADMA ± SDMA (endothelial NO axis), MPO for neutrophil-driven vascular oxidants, and either oxLDL or Lp-PLA2 to see oxidised-lipid activity in the arterial wall.
In this group, a single 5-10mg methylene blue dose is often beneficial for this ROS and MetHb, however is not a long-term solution.
One strategy for this subgroup is to slowly increase the dose by 50mcg each day (starting at 50mcg / day and likely not more than 300mcg / day), until *ANY* change is observed - positive or negative, then holding steady at that dose. Eventually, this dose can be reduced to 50 mcg / day.