Cortisol is the “master” negative regulator for IFN-γ related immune activity and promotes catabolic energy availability via epinephrine (adrenaline).
Elevated cortisol doesn't just suppress immune function; it also alters neurotransmitter balance, which can influence mood, cognition, and energy levels.
What this means is that any/all influences which promote cortisol also decrease IFN-γ activity and provide some “relief” for many of the symptoms observed in ME/CFS.. while potentially creating others. This allows periods of increased functionality, while simultaneously inhibiting the necessary suppression of the pathogens that are triggering the innate immune response pathways.
In the disease model, we have described how cortisol acts as a “sensor” and signalling relay for insufficiencies of NAD+, P5P and glucose / glycogen, via phosphatidylserine and HSD11β1/2 flux (see figure 4). The metabolism for NAD+ and P5P is altered by IFN-γ and they act as upstream sensors for specific IFN-γ activities which can upset the metabolism or cause excessive tissue damage via oxidative stress. An inverted diurnal cortisol release pattern is expected.
When any of the sensed metabolites are insufficient, cortisol increases, signalling for an increase of epinephrine. This promotes energy "scavenging" or "catabolism", while inhibiting IFN-γ immune activity. This allows some of the cofactors and metabolites to replenish and by doing so, it helps restore normal metabolism.
However, the same epinephrine -> cAMP-PKA elevation from any trigger also signals for your cells to stop storing glycogen and instead use the existing glycogen pools for energy (see figure 1, upper right). Epinephrine activates hepatic glycogen phosphorylase and inhibits glycogen synthase within minutes; glucagon cooperates during fasting. Cortisol modulates these systems on a slower timescale. Glycogen storage can therefore become problematic when epinephrine and/or cAMP-PKA is dysregulated and chronically elevated.
As the metabolites reach sufficiency, cortisol levels normalise. If any triggers for IFN-γ are still present, then IFN-γ activity will resume and the cycle will repeat, as necessary.
Exercise, sex hormones and heat can increase IFN-γ. Dietary supplements can support IFN-γ activity. Cortisone medications are potent immunosuppressants and will inhibit IFN-γ.
Appropriate carbohydrate and protein intake (with uninhibited metabolism) supports optimal glycogen homeostasis. Sublingual NAD+ or NADH can efficiently support the total NAD+:NADH pool status, methylene blue can support the NAD+:NADH redox and apigenin can reduce the pool degradation. Creatine can reduce the methylation “costs” associated with use of this pathway and also increase glucose transport. Magnesium and zinc can support B6 -> P5P metabolism. Manganese, biotin and B12 sufficiency is required for conversion of other substrates (protein -> amino acids, odd-chain fatty acids) into glycogen, usually via the TCA cycle to the glycolysis pathway, however flowing in reverse.
Hypothyroidism affects both glucose metabolism and “B6 toxicity” / P5P insufficiency. The thyroid hormone, T3 (tyrosine, heme iron, iodide, selenium, calcium) is required to maintain FMN levels, needed for P5P recycling and to induce pyruvate flux into the TCA cycle.
Chronic hypoxia can be a significant contributor to this cascade.
The primary sex hormones (testosterone / DHT in males, estradiol in females) sense the elevation of NADPH (created during physical / metabolic activity), with sufficiency of NAD+, magnesium, boron and zinc. These primary sex hormones then promote creatine synthesis and glucose uptake. They inhibit cortisol levels, promote nitrogen metabolite recycling and glycogen synthesis. This also allows IFN-γ activity to increase, which is also needed for tissue adaptations to exercise. Non-optimal sex hormones can cause chronic cortisol increase.
Overnight, hepatic glucose output draws on glycogen then shifts toward gluconeogenesis; the pre-awakening rise in cortisol supports glucose production, whereas glycogen replenishment resumes mainly with daytime, insulinised feeding.
In severe ME/CFS this diurnal rhythm is
delayed, blunted at night and erratic by day. With hepatic glycogen
never fully restored, even small physical or emotional stresses deplete
the reserve. The body responds with abrupt pulses of cortisol and
epinephrine to keep blood glucose within safe limits, but these surges
have costs and the repetitive signalling can contribute to nervous
system adaptations / programming towards hyper-arousal and sympathetic
overdrive.
Histamine triggers glycogen redistribution
When intestinal dysbiosis shifts towards ethanol‑producing organisms, portal blood delivers a steady acetaldehyde load to the liver. Hepatic aldehyde dehydrogenase (ALDH) is the main clearance route, yet acetaldehyde itself oxidises the enzyme’s catalytic cysteines and slows its own detoxification. The diamine oxidase (DAO) -> ALDH pathway, responsible for extracellular histamine degradation in the gut wall and liver sinusoids, is inactivated by the same aldehyde, as is the monoamine oxidase MAO) -> ALDH pathway, in the brain. Consequently, acetaldehyde and histamine accumulate in parallel. Extracellular ATP signalling can also degranulate mast cells and release histamine, which can be triggered by a number of sources, including autonomic dysfunction.
Microbiome dysbiosis allows basal histamine levels to become elevated and creates further sensitivity to small histamine release triggers.
Histamine released from resident mast cells activates two hepatic pathways. H1 receptors raise intracellular Ca²⁺ and switch phosphorylase kinase, accelerating glycogenolysis. H2 receptors follow the classical Gs → cAMP → PKA → CREB/CRTC2 route, up‑regulating the G6pc gene and sustaining gluconeogenesis. Plasma glucose rises briefly, then falls once hepatic glycogen stores are exhausted, prompting compensatory sympathetic activation. In susceptible individuals this often presents as episodic tachycardia, light-headedness and adrenergic symptoms 45–90 minutes post-meal.
However, histamine also binds H1 receptors on perivascular macrophages in skeletal muscle. The resulting IL‑6 pulse engages STAT3 in adjacent fibres, increasing GLUT4 expression and glycogen‑synthase activity.
Logically, under normal circumstances this histamine signalling cascade would support post‑exercise muscle glycogen recovery, by converting liver glycogen into circulating glucose, whilst promoting muscle glycogen storage.
However, when hepatic glycogen is already depleted, the extra glucose uptake is limited, leaving IL‑6 signalling elevated and favouring low‑grade inflammation. This also creates and/or exacerbates symptoms of liver glycogen depletion.
Acetaldehyde compromises tight‑junction proteins - particularly claudin‑1, occludin and ZO‑1, through oxidation of cellular glutathione and direct adduct formation with junctional proteins. Transepithelial electrical resistance falls, allowing luminal antigens (dietary proteins, lipopolysaccharide, fungal mannans) to enter the portal and systemic circulation. These antigens engage hepatic Kupffer cells and circulating innate‑immune receptors, amplifying IL‑6, TNF‑α and further mast‑cell priming. The additional antigen load therefore strengthens the histamine–acetaldehyde feedback and broadens symptom variability to include post‑prandial urticaria, arthralgia and fluctuating cognitive function.
Mitochondrial ROS generated during acetaldehyde metabolism oxidise tetrahydrobiopterin (BH4) to BH2, uncoupling endothelial nitric‑oxide synthase. Uncoupled eNOS diverts electrons to superoxide formation; superoxide combines with residual nitric oxide to form peroxynitrite, which nitrates and further impairs both ALDH and DAO. The resulting endothelial dysfunction limits capillary dilation, reduces oxygen delivery to muscle and contributes to orthostatic intolerance.
Mast‑cell activity is sensitive to the prevailing sex‑steroid environment. Physiological oestradiol concentrations enhance Ca²⁺ influx through membrane‑bound ER‑α, lowering the threshold for degranulation. Androgens act more slowly via nuclear AR to repress cytokine transcription and reduce mediator content. The net effect is hormone‑dependent rather than genetically sex‑specific: high oestrogen states (peri‑ovulation, pregnancy, oestrogen therapy) generally increase histamine release, whereas adequate testosterone or progesterone temper it.
Understanding this cascade clarifies why seemingly minor dietary choices, hormonal fluctuations or exercise sessions can provoke disproportionate symptoms. Interventions need to address microbial-sourced acetaldehyde, barrier integrity, and enzymatic detoxification simultaneously to break the self‑reinforcing loop.
Figure 9 shows this in a more concise way.
Histamine is also known as the stomach’s on-demand acid tap. Enterochromaffin-like (ECL) cells in the gastric corpus suffuse their neighbourhood with histamine whenever gastrin or vagal acetylcholine says it is time to digest. The molecule travels perhaps a millimetre, binds H2 receptors on neighbouring parietal cells and ignites the Gs → cAMP → PKA cascade that lifts proton pumps to the apical membrane. Within minutes, the luminal pH trends towards highly acidic, pepsinogen flips to pepsin and dietary proteins begin to unravel. Antagonising H2 receptors, as many dyspepsia patients discover, cuts this acid tide by roughly two-thirds, while potentially disturbing protection against oral pathogens entering the small intestine.
Further down the GI tract, histamine’s role becomes subtler. In the muscularis it tweaks peristaltic tone: H1 receptors on circular muscle promote contraction, whereas H2 receptors on longitudinal muscle ease it, ensuring chyme does not idle too long yet still pauses where absorption is richest. In the ileum histamine encourages chloride and water secretion through enteric neural reflexes, a housekeeping flush that keeps the mucosa clear of excessive bacterial growth.
Histamine also acts as a sentinel mediator. Intestinal mast cells sample antigenic fragments leaking through the epithelium; when they degranulate, the released histamine increases local blood flow and vascular permeability, banking extra immune cells against potential breach. At modest concentrations this response is quietly protective, tightening junctions through H4-receptor signalling on epithelial cells and stimulating mucus production that traps pathogens.
At higher levels, eg. created by chronic acetaldehyde, the same mechanisms become counter-productive: permeability rises too far, afferent nerves fire, and the familiar triad of bloating, cramps and watery stool appears. Acid may swing low, motility becomes erratic, antigen load climbs and patients experience the fluctuating constellation of symptoms often labelled “histamine intolerance” or Mast Cell Activation Syndrome (MCAS).
Overall, some of these challenges can influence further self-sustaining cycles, eg.
Increased protein catabolism - cortisol mobilises amino-acids for gluconeogenesis, gradually lowering the circulating pools of (often already problematic, due to low Queuine) tyrosine, histidine, asparagine and aspartate, which are needed for neurotransmitter and enzyme synthesis, affecting energy metabolism, causing additional epinephrine spikes / sympathetic bias.
Dysregulated metabolic feedback - frequent intermittent epinephrine bursts further inhibit glycogen synthase, perpetuating the under-filled liver glycogen tank, causing additional epinephrine spikes / sympathetic bias.
Sympathetic overdrive
There are also many influences observed in ME/CFS which can contribute to sympathetic overdrive and chronic flight/flight. Overall, the balance is normally biased heavily against being able to maintain parasympathetic sufficiency and (liver) glycogen stores.
This bias NEEDS to be shifted towards a neutral balance to restore normal energy metabolism and help remove glycogen deficiency as an influence in debilitating symptoms like POTS, PEM, cognitive, mood and sleep disorders. This means adding / increasing parasympathetic tone promoting influences into your routine and removing as many unnecessary sympathetic tone promoting influences, often sources / triggers of epinephrine spikes.
Some of these influences can induce long-term shifts, some are acute effects.

Separately, the catecholamine degradation pathways needs to be restored and adrenergic receptor expression / sensitivity restored, to remove unhelpful "hair-trigger" response to stimuli.
A simple test for sympathetic overdrive is trying to swallow, three times, quickly. In severe ME/CFS, loss of ability to swallow often coincides with loss of parasympathetic / vagal tone.
https://www.instagram.com/reel/DHtW0iHsbOE/
[A helpful Instagram video by Taylor and Alisha Kruse - they have a lot of relevant neuro content.]
What the parasympathetic system actually does
The parasympathetic nervous system sets the body’s “rest-and-digest” baseline. It is not an on/off switch. Brainstem nuclei send fibres through the vagus to the chest and abdomen, and sacral outflow serves the pelvis. When sympathetic drive runs high for long periods, parasympathetic signalling is blunted or becomes erratic. The result is predictable changes in gut propulsion and secretion, glandular output, pupil behaviour, heart rhythm, bladder emptying, and sexual function.
Gastrointestinal
Swallowing - starting a swallow is a voluntary, somatic motor act coordinated in the brainstem using cranial nerves V, VII, IX, X and XII. Parasympathetic vagal output is not required to initiate it. Once the bolus enters the oesophagus, parasympathetic pathways organise primary peristalsis and relax the lower oesophageal sphincter. The enteric nervous system can still generate secondary peristalsis locally, but global coordination drops when vagal tone is low.
Stomach - vagal input enables receptive relaxation of the fundus, coordinates antral grinding, and gates pyloric opening.
Pancreas and bile - vagal drive stimulates pancreatic enzyme and bicarbonate secretion, and assists gallbladder contraction alongside CCK.
Intestine and colon - parasympathetic-enteric crosstalk supports peristalsis and fluid secretion. Sacral outflow drives the defecation reflex by contracting rectum and relaxing the internal anal sphincter.
Sympathetic overdrive pattern: dry mouth, weak or discoordinated peristalsis, early satiety, reflux from poor LES control, slow gastric emptying, flat or greasy stools from low enzyme/bile delivery, bloating, constipation or paradoxical alternating bowel habit.
Cardiovascular
Vagal tone sets the resting heart rate below the pacemaker’s intrinsic speed and stabilises AV nodal conduction. With persistent sympathetic bias you see a higher resting rate and reduced beat-to-beat variability.
Sympathetic overdrive pattern: resting tachycardia, low HRV, exaggerated heart-rate responses to minor stressors.
Respiratory
Vagal efferents tighten airway smooth muscle and promote mucus secretion, which is part of normal airway defence. Sympathetic signalling tends to dilate the bronchi and dry the mucosa. In real life both systems interleave.
Sympathetic overdrive pattern: dry airways, throat irritation and cough with little mucus. In some phenotypes, unstable vagal reflexes coexist with overdrive and produce intermittent bronchospasm.
Ocular
Parasympathetic fibres constrict the pupil to light and enable near-focus by contracting the ciliary muscle. They also drive tear secretion.
Sympathetic overdrive pattern: larger pupils in room light, difficulty with near vision, dry or gritty eyes.
Salivary and nasal glands
Parasympathetic secretomotor drive sustains watery saliva and nasal mucus that humidifies inspired air.
Sympathetic overdrive pattern: dry mouth, altered taste, tooth and gum vulnerability, nasal dryness or crusting.
Urinary
Sacral parasympathetic outflow contracts the detrusor and relaxes the internal sphincter during voiding. Somatic pudendal control handles the external sphincter.
Sympathetic overdrive pattern: hesitancy, weak stream, incomplete emptying, or conversely urgency from reflex instability.
Reproductive
Sacral parasympathetic activity initiates erectile tissue engorgement via endothelial nitric oxide. Emission and ejaculation are mainly sympathetic and somatic.
Sympathetic overdrive pattern: reduced arousal and erection quality (penile and clitoral), difficulty sustaining engorgement.
Here is a table of influences that promote acute and/or chronic *parasympathetic* tone:
Here is a table of influences that promote acute and/or chronic *sympathetic* tone:
One of the many takeaways from the parasympathetic vs sympathetic influence tables above is that any kind of breathing disorder, especially one that biases mouth breathing over nasal breathing can have a negative affect on achieving a balanced parasympathetic-to-sympathetic tone and will therefore be a high priority for targeted intervention.
https://pubmed.ncbi.nlm.nih.gov/37867476/
In that context, autonomic imbalance has also been reported in small studies for allergic rhinitis using HRV analysis.
https://pmc.ncbi.nlm.nih.gov/articles/PMC3582187/
Chronic sinonasal inflammation has also been studied in relation to autonomic markers (eg. HRV and pupillary light reflex metrics) in CRS cohorts. While this doesn’t prove nasal inflammation causes systemic dysautonomia, it supports the idea that sinonasal disease can couple to autonomic state, directly (sensory/autonomic reflexes) and indirectly (obstruction, sleep fragmentation, hyperventilation patterns).
https://www.nature.com/articles/s41598-021-01153-1
The clinical picture may include fasting intolerance, exaggerated post-exertional malaise, morning hypoglycaemia and wide swings in lactate that resemble certain glycogen-storage disorders, albeit driven by signalling rather than an inborn enzyme defect.
Therapeutic priorities are (i) frequent balanced meals that combine low-glycaemic carbohydrate with medium-chain triglycerides (or large doses of L-carnitine / acetyl L-carnitine used in the protocol), (ii) consider nocturnal adrenergic dampening (for example low-dose clonidine / ivabradine) to allow normal cortisol timing, and (iii) graded re-entrainment of sleep-wake cues so that the liver again “expects” to store glycogen after dusk.
Overall, multiple biochemical bottlenecks converge in ME/CFS to disturb catecholamine balance:
eg.
1. Queuine deficiency (secondary to microbiome dysbiosis) and tetrahydrobiopterin (BH₄) depletion slow translation and activity of tyrosine hydroxylase, the rate-limiting step in dopamine production, causing reduced dopamine synthesis.
2. Acetaldehyde directly inhibits aldehyde dehydrogenase (ALDH), depletes zinc and inhibits thiamine pyrophosphate (active Vitamin B1) synthesis. The zinc deficiency leads to further deficiencies of active B vitamins. Low FAD (active Vitamin B2) and zinc limit monoamine oxidase (MAO) and catechol-O-methyl-transferase (COMT) activity. Released dopamine, norepinephrine and epinephrine may therefore persist longer.
3. Acetaldehyde depleting zinc also affects P5P metabolism and dopamine synthesis by inhibiting aromatic L-amino decarboxylase (AADC) activity.
4. Acetaldehyde triggering mast cell activation and histamine release affects tyrosine hydroxylase activity.
5. Low iron and/or neural hypoxia, affecting phenylalanine and tyrosine hydroxylase.
6. P-cresol from dysbiosis, affecting dopamine beta hydroxylase.
7. Oxidative stress affecting phenylalanine, tyrosine and dopamine beta hydroxylase.
8. Electrolyte deficiencies affecting tyrosine hydroxylase, VMAT2, DAT and NET transporters.
9. cAMP-PKA dysregulation from chronic endogenous opioid synthesis pathway being activated by ALDH inhibition, if MAO is still functioning.
..This is not an exhaustive list.
Chronic sympathetic over-activity down-regulates vascular β₂- and presynaptic α₂-adrenoceptors. The system compensates with larger and less predictable bursts of catecholamines to achieve ordinary physiological tasks (for example standing or minimal exertion). This can also be exacerbated by (presumed regulatory, as a compensation) "autoimmune" antibodies for adrenergic receptors.
These receptor alterations also mean that any shift towards parasympathetic sufficiency can induce a level of temporary hypometabolism until the homeostasis resets, over a few weeks. The level of hypometabolism may also be enough to force a reflex into sympathetic spikes, exacerbating efforts towards normal homeostasis.
When catecholamine levels normalise, but receptors remain desensitised due to the previous sympathetic overdrive, chronic PTSD or stress, symptoms like fatigue, cognitive dullness, low BP, and orthostatic intolerance can appear. This results from a “relative catecholamine deficiency.” Even with normalised levels, desensitised receptors (like alpha2 and beta2) mean there's a decreased adrenergic tone and paradoxical crashes. Surges of epinephrine may occur after episodes of low energy, causing hypoglycemia-related adrenal bursts and crashes, leading to unexpected symptoms like anhedonia and fatigue.
Clinical tell-tales of an epinephrine surge while receptors are still half-asleep:
0–5 min - Sudden heart-in-throat palpitation, cold sweat, tremor, pilo-erection, brief spike in systolic BP. EPI acts on the fraction of β₁/β₂ receptors that are not desensitised; α₁ vasoconstriction is relatively spared.
5–30 min - Shaky hunger, light-headedness, hyper-alert or “wired” feeling. Hepatic glucose release overshoots; brain re-gains perfusion but over-reacts
30–120 min - Crash: profound fatigue, yawning, headache, sometimes nausea. As EPI is metabolised the receptor deficit is unmasked again; glycogen is partly spent, leaving a transient energy hole
Exercise intolerance and easy fatigability will occur. β₂-adrenergic drive to skeletal muscle and myocardium is blunted, so peak cardiac output and mitochondrial substrate flux lag behind demand. This mirrors the desensitisation seen in chronic muscle-pain cohorts.
Impaired β-oxidation impairs catabolic energy metabolism and means small drops in glucose activate hypothalamic “fuel alarm” pathways, causing adrenaline surges that can feel indistinguishable from panic. Sleep will temporarily become broken and difficult, relative to glycogen stores and norepinephrine "long" pulses.
The brain has a hard-wired crisis response for cellular energy deficit -
1. The ventromedial hypothalamus senses falling intracellular ATP or glucose.
2. It fires the sympatho-adrenal axis, causing the adrenal medulla to release epinephrine.
3. Epinephrine burns glycogen stores, elevates hormone‑sensitive lipase in adipose tissue, and raises cardiac output.
This
counter-regulation is best documented in insulin-induced hypoglycaemia:
even modest falls in plasma glucose produce a several-fold surge in epinephrine
that is not fully replaceable by glucagon alone.
These changes can reinforce an anxiety-phobia cycle. Each adrenergic spike produces tachycardia, dizziness and a sense of impending collapse; the cortex learns to associate ordinary movement with danger, encouraging further inactivity and social withdrawal. Poor sleep prevents overnight receptor resensitisation, and the cycle repeats. A large part of overcoming this vicious trap is awareness of the issue and then learning to consciously override the signals being fed to the nervous system while the transition is underway.
The receptors will wake up, however it's a slower journey:
β-receptor resensitisation needs days-to-weeks of lower catecholamine tone and adequate omega-3 intake (membrane fluidity matters).
The α₂ presynaptic brake tends to reset faster (days), which is why clonidine/guanfacine at night could smooth the ride during taper.
Adequate sleep and micronutrients (esp. Mg²⁺, Zn²⁺ and B-vitamins) can also hasten the up-regulation of G-protein coupling units.
Ketotifen can also be particularly helpful. Histamine released from mast cells can stimulate sympathetic outflow and locally augment norepinephrine release. Blocking H1 and stabilising mast cells removes that extra push on the accelerator. Long-term oral ketotifen has been shown to increase β2-adrenergic receptor density. Central H1 blockade and mild anticholinergic tone tilt the ANS parasympathetic, lowering baseline sympathetic tone and improving slow-wave sleep - both conditions that favour receptor resensitisation. Net effect: fewer histamine-triggered norepinephrine releases, shallower epinephrine spikes, and a slow rise in β-receptor responsiveness.
(Practical caveats: drowsiness - take at night, anticholinergic dry-mouth, and mild orthostatic drops; dose-titrate over a week from 100 mcg to avoid a “hung-over” feel.)
Until then, oscillating between “underpowered” and “epinephrine dump” is common. Forewarned is forearmed: frequent small meals with complex carbs and fat, gentle aerobic work (appropriate levels of walking, etc.) to retrain β-oxidation, and cautious use of α₂ agonists or low-dose β-blockers can soften the swings while the receptors crawl back to baseline.
This area of homeostasis reset can be challenging and without awareness, it can easily create another loop / trap. Don't fall into it.
In this protocol, restoring homeostasis starts with biochemical housekeeping. Replenishing the minerals, reducing acetaldehyde through targeted antimicrobial therapy and binders, and rebuilding queuine-producing microbial colonies can give the enzymatic machinery a chance to recover and reduce influences promoting sympathetic overdrive.
Frequent meals that pair low-glycaemic carbohydrates with medium-chain triglycerides (and/or the protocol dosing acetyl L-carnitine) helps protect the liver’s limited glycogen and spare amino-acids, while spirulina and other metabolic supports help realign cortisol timing.
As adrenergic spikes quieten, short recumbent muscle contractions or very gentle cycling become tolerable, promoting vascular conditioning without provoking post-exertional malaise. This can open up to walking and other activities as they become appropriate. A brief daily video call or other similarly "low-demand" social contact can then begin to reactivate normal reward pathways and help shift the balance towards a more parasympathetic state. Within this framework, behavioural strategies such as paced breathing or graded stressor exposure need no longer fight against biochemical headwinds and instead build on a slowly stabilising neuroendocrine landscape.
As described above, chronic disease-related lifestyle factors and trauma imprinting / autonomic learned responses to stimuli - namely stress / fear / anxiety - cause the limbic system to promote cortisol levels and inhibit the IFN-γ pathway / immune response, while decreasing glycogen stores. As this also temporarily decreases some “ME/CFS” symptoms, before rebounding, a persistent cycle of fear / anxiety, and immune dysregulation can also be learned / imprinted.
Has your life been entirely devastating for many months or years?
Have you lost nearly everything?
(Are you lonely?)
..Have you been medically gaslit (or abandoned) during this time and have therefore spent many of your days isolated from your friends, loved ones and former life, while possibly laying for long periods in your own filth and often a mouldy bedroom?
These circumstances can reliably create trauma.. and guess what? No one - literally, no one - can deal with their trauma, alone!
What you’re experiencing is what NORMALLY HAPPENS when a sensitive, intelligent system is asked to survive without the right support. Trauma isn’t imagined - the studies show it gets imprinted in cells. It alters your hormones, neurotransmitters, immune function, and even nutrient handling. This is intrinsic biology and not something to blame.
In addition to the daily trauma created by the disease, the chronic endogenous opioid synthesis pathway PRIMES the nervous system towards hyper-vigilance and rigidity -
see figure 17 and figure 18 and figure 19 on the disease model page. Preliminary data also shows that the adenosine / inosine dampening signal for extracellular ATP alarm signalling is impaired, biasing the nervous system towards hyper-vigilance and hyper-arousal.
These symptoms will normally be exacerbated during withdrawal from the endogenous opioid synthesis cascade, creating another trap, however this will need to be completed to achieve a full recovery.
If your nervous system feels like it’s running the show lately - prioritising short-term survival over long-term repair, THAT'S NOT YOUR FAULT. This is the body’s normal way of surviving / coping. However, over time and repeat exposure to stressors or trauma, your nervous system adapts to existing in this harsh environment and is often reluctant to reset the alarm system, especially if it thinks you might still be unsafe. When this happens, it needs gentle reminders to hand control back to the repair systems, after removing the metabolic crisis alarms and enough of the pathogenic burden.
The nervous system is NOT malfunctioning - it's adapting to excessive chronic stress signalling and trying its best to keep you safe.
By understanding these adaptations, we can work WITH the body to restore balance.
If you find yourself in this situation - which is entirely expected after "living" with ME/CFS or any other named entry-point to the disease model) - then getting help is essential to your recovery.
Your nervous system sends "predictions", not "facts"
It can be helpful to understand that your nervous system is not a neutral, unbiased reporter. It doesn't state "facts". It has a pattern-matching threat predictor function, with a primary goal of keeping you safe. It continually guesses what is about to happen next and prepares you in advance.
When you've had a history of chronic illness, trauma, or prolonged stress, that prediction system can be primed by biochemistry and threat priors to run a “better safe than sorry” program - it overestimates danger and underestimates your capacity to cope, giving you a false and limiting perception of real life.
That program shows up as thoughts like:
“This is unsafe.”
“I’m going to fail.”
"This will hurt me."
“This isn’t the right time.”
“I can’t do this.”
“This will go wrong.”
“If I don’t do X, I’ll be unsafe.”
.. and it is NOT just thoughts - a threat prediction from the nervous system can recruit the whole body to make you really FEEL the message, too. The thoughts may be potentially accompanied by eg. tight chest, nausea, adrenaline dumps, difficulty swallowing, GI upset, immune system activation, mast cell activation, gnawing sensations in the stomach, "stomach drop", weakness, fatigue, pain spikes, breathing difficulties, even panic.
Those sensations and their related biochemistry are completely real and measurable.. however, the BIGGER question is whether the nervous system's prediction is really accurate, or often (without a lot of NEW life experiences to recalibrate from), largely based on OLD fears, OLD traumas, OLD patterns, or OLD emotionally-charged memories… which don't relate to what’s actually happening RIGHT NOW.
"The trap" is treating the ALARM as a true verdict, or FACT, rather than just a PREDICTION.
To move forward from this trap, treat the alarm signal instead as a hypothesis and allow for the idea that your nervous system is running on incomplete and outdated data.
Predictions can be challenged.
Predictions can be tested.
Predictions are not reality.
Next time, you can try this, in the moment:
Ask, “Is this a FACT, or is this my body running a threat PREDICTION?”
Name the prediction, out loud, in one sentence: “My nervous system predicts X will happen.”
Then choose one small, safe test: a 30–120 second action that gathers new evidence (eg. stay in the situation, take one step, send the message, stand up, walk to the door, do the first minute, write the first sentence).
(Nose-breathe slowly, deeply and deliberately throughout the test. Try to keep your nervous system in a parasympathetic state.)
Baby steps. With each successful test, you’re updating the threat-prediction model data and recalibrating the nervous system.
Another good, cheap literary resource - if you want an accessible, non-technical introduction to these systems is "Don’t Believe Everything You Think", by Joseph Nguyen. [Book link]
Trauma counselling / therapy, EMDR, vagus nerve stimulation and various other interventions can also be game-changing for some people who are suffering from chronic "fight or flight" programming induced by complex trauma and chronic illness. A 19 page, downloadable ChatGPT-generated "Deep Research" report on the latest evidence for different interventions as of August 2025 can be found here.
Stellate Ganglion Blocks (SGB) can be another helpful intervention, by resetting and controlling this state, however they are not a long-term solution, unless you use them as a helpful educational tool, to experience a period of remission from the crisis state, which helps you learn to rebuild trust in your body. NB. SGBs should not be used until the underlying issues causing hypometabolism are resolved, otherwise you'll feel like you've taken a backwards step in functionality. The crisis state is providing a level of energy to sustain you, even if that's dysregulated.
However, this protocol also describes an anxiety -> phobic response trap that can cage people and ways to navigate this successfully. From my observations, this affects a significant number of people.
If you are affected by this subconscious programming, you will struggle to make forward progress while still in a chronic "fight or flight" state, due to the downstream metabolic consequences:
The "fight or flight" and/or "crashed" state may also lead to low glycogen and significant amounts of lactic acid and oxalates being generated. If the lactic acid can't be metabolised efficiently to usable energy, this can cause swollen / inflamed / numb / tingling body parts, especially in areas with smaller blood vessels, such as hands, feet, face and lungs.
Lactic acidaemia can also make it very difficult to restore zinc, electrolytes and missing bacteria which are pH sensitive, eg. bifidobacterium and butyrate producers, as excess lactic acid is secreted into the GI tract and also via your kidneys, leading to frequent urination, "sandy urine", kidney stones, etc.
If you are feeling lost or in a crisis, THRIVE Lifeline offers 24/7 international text-based crisis support to anyone aged 18+, with a specific focus on multiple marginalized communities. They do not engage in non-consensual "active rescue" and they prioritise the texter's consent + autonomy.
For urgent help
SMS: +1.313.662.8209
General enquiries
Website: https://thrivelifeline.org/
Email: info@thrivelifeline.org
"Anxiety", isolation, and phobia
Before continuing, for clarity, I'll restate my previously published, long-standing position against using CBT and GET as a primary therapy for ME/CFS and similar diseases:
I anticipate that there is a special place in hell reserved for clinicians who negligently misdiagnose ME/CFS patients with a purely psychological disease or "anxiety", or force patients with measurable mitochondrial dysfunction from chronic infections / dysbiosis / induced malnutrition to perform "graded exercise".
You wouldn't initially prescribe a diagnosed septicaemia patient CBT and GET as their primary therapy, so it's appalling that this continues to be the "gold standard approach" taken by numerous clinicians for ME/CFS patients. There are decades of evidence against this.
Yes, once the infections and malnutrition are sufficiently resolved and mitochondrial metabolism allows for it, physical rehabilitation is absolutely encouraged as part of the recovery process.
Yes, there are neurological and psychological issues created in this disease model - biochemically and from trauma, isolation, coping mechanisms and learned fear responses. These each require different interventions.
[/RANT]
This section explores the connections between "anxiety", isolation, and phobic responses to symptoms in individuals with ME/CFS or similar chronic diseases. Drawing on parallels between chronic pain, fibromyalgia and ME/CFS, it aims to provide a clearer understanding of these challenges and how to exit another closed-loop / cycle which can be present in some patients.
Understanding the fear-avoidance cycle
A fear-avoidance model, initially developed in the context of chronic back pain by Dr Sarno as "Tension Myositis Syndrome (TMS)" and later extended by Dan Buglio as "Perceived Danger Pain (PDP)", also provides a working description for an observed pattern of daily experiences, physiological responses and behaviour that may create a further trap for some people already suffering from ME/CFS and precursor states on the slippery slope described by the disease modelling.
A popular example of perceived danger pain is the "Rubber Hand
Illusion" - a psychological experiment that demonstrates how the brain
can be tricked into perceiving a fake hand as part of one's own body. In
this setup, a participant's real hand is hidden from view, and a rubber
hand is placed in front of them. Both the hidden real hand and the
visible rubber hand are simultaneously stroked with brushes. Over time,
many participants begin to feel as though the rubber hand is their own.
This illusion highlights the brain's ability to integrate visual and
tactile information to create a sense of body ownership. https://youtu.be/sxwn1w7MJvk
In chronic pain, the fear of pain or "perceived danger pain" can lead to avoidance behaviors, which ultimately reinforce fear and reduce / prevent pain-free movement. The brain creates a genuine sensation of pain and measurable metabolic alterations to a perceived danger, to try and keep you safe. This is described as a learned phobic response that happens even when the original danger has been removed.
https://journals.lww.com/pain/fulltext/2022/08000/impaired_pain_related_threat_and_safety_learning.18.aspx
Similarly, some people with ME/CFS may fear pain from triggering or exacerbating existing metabolic symptoms such as mast cell activation syndrome (MCAS), post-exertional malaise (PEM), inflammation, sleep deprivation, etc, leading them to increasingly avoid foods, supplements and people, along with physical and mental activities. This avoidance can result in severe deconditioning, increased isolation, and a greater severity of symptoms, perpetuating a closed-loop / cycle of fear and avoidance.
Notably, even the possibility of avoiding discomfort can paradoxically increase fear over time. Studies show that individuals who are given the option to avoid pain experience increased fear when that option is removed, highlighting how avoidance can amplify anxiety rather than reduce it.
https://academic.oup.com/abm/article-abstract/55/3/216/5876277
Stress, isolation, and heightened threat response
Heightened threat-perception and response is a significant factor for individuals "living" with ME/CFS, similar to its role in chronic pain. People with ME/CFS often experience heightened anxiety, too - created by the mitochondrial dysfunction and downstream energy crisis. Neural hypoxia can be one of the more common influences, downstream of immune activity, impaired iron homeostasis, oxidative stress, blood-flow and structural issues.
Additional stress can also sometimes be driven by feelings of inadequacy and/or fear from not being able to participate in life and fulfil roles as parents, lovers, workers, or friends. This anxiety is often compounded by fear of the unknown, thanks to inadequate medical care and also anticipatory fear - worrying about potential symptoms exacerbation by taking even small actions. This leads to heightened stress and worsened symptoms.
Isolation and unrefreshing sleep further intensifies this stress. For those with ME/CFS, reduced social contact can enhance the brain’s threat-detection systems, making individuals more likely to interpret normal bodily sensations as signs of danger. Studies indicate that even brief periods of social isolation can increase vigilance to perceived threats, which contributes to the cycle of fear and avoidance.
https://royalsocietypublishing.org/doi/10.1098/rsos.240101
Moreover, as a "perceived danger syndrome", symptoms related to immune activity and die-off, such as inflammation, pain, elevated histamine, rashes, nausea, diarrhoea or flu-like sensations, can be misinterpreted by the brain as a danger signal.
It sounds rather incredible, however mere perception of a threat can alter biology before any contact. In humans, simply anticipating an “infectious” other in virtual reality engages peripersonal-space and salience networks, tightens coupling with the hypothalamus, and transiently shifts innate lymphoid and NK-like cell frequency and activation. In plain terms, prediction alone briefly primes the immune system and readiness circuits, even without a pathogen present.
https://www.nature.com/articles/s41593-025-02008-y
Repeated or uncontrollable threats write a slower trace in limbic circuits. In rodent stress paradigms, extracellular ATP accumulates in the hippocampal microenvironment, activates microglial P2X7, assembles the NLRP3 inflammasome, and increases IL-1β. causing microglial-driven neuroinflammation and behavioural output. Blocking P2X7 or deleting NLRP3 prevents the behavioural phenotype. Translation: ongoing stress can lock in an inflammatory signal in brain immune cells that sustains hypervigilance. (See Figure 19.)
https://www.sciencedirect.com/science/article/abs/pii/S0006322315010367
Top-down outputs then signal for gut microbiome alterations within hours. Chemogenetic activation or inhibition of hypothalamic AgRP or POMC neurons, or central leptin or ghrelin, rapidly re-tiles intestinal microbiota in mice within 2-4 hours, independent of food intake. This is a fast autonomic channel by which threat state can alter microbial metabolites that feed back to glucose handling and inflammatory thresholds.
https://www.nature.com/articles/s42255-025-01280-3.pdf
Early-life experiences set priors that change how the loop runs. In a longitudinal cohort, toddler microbiota composition predicted resting-state network architecture at age 6, which in turn tracked internalising symptoms at 7.5 years. The mediation via the connectome puts the brain in the middle of a gut-to-brain-to-behaviour cascade. This evidence is early, however the direction is consistent.
https://www.nature.com/articles/s41467-025-64988-6
Surprisingly, trauma and threat experiences can be narrowly encoded across generations. Paternal odour-fear conditioning in mice produced cue-specific sensory hypersensitivity and glomerular enlargement in 8 generations of offspring, with hypomethylation at the matched olfactory-receptor locus in sperm. That implies inherited, feature-specific threat priors can raise threat-detection circuit gain before any new learning.. which reminds me acutely of the saying "you either face your demons or they raise your children".. and great-[..]-great-grandchildren.
https://pmc.ncbi.nlm.nih.gov/articles/PMC3923835/
Severe trauma also leaves a durable systems imprint even when symptoms are less obvious. Years after a mass-trauma event, medically healthy survivors showed higher IL-1β, lower IL-2R, lower morning cortisol, higher resting diastolic blood pressure, and blunted cardiovascular reactivity to trauma scripts, with weak coupling to current PTSD or depression scores. This means our biology can remain shifted while conscious distress abates.
https://www.cambridge.org/core/services/aop-cambridge-core/content/view/C5935399886A5B10F0EBD55C6C7B0F4A/S1049023X24000360a.pdf/learning-from-hindsight-examining-autonomic-inflammatory-and-endocrine-stress-biomarkers-and-mental-health-in-healthy-terrorism-survivors-many-years-later.pdf
This heightened threat perception can create a nervous system feedback loop, as a form of dysautonomia, where normal metabolic processes, eg. immune responses are seen as threats, further elevating stress levels and acting as a "fight-or-flight" trigger, chronically depleting glycogen stores, activating altering blood-flow and potentially leading to avoidance behaviors.
This misinterpretation by your subconscious brain reinforces the fear-avoidance cycle, making it more difficult for people to break free from the loop of symptom exacerbation and fear. The nervous system can create real, measurable symptoms of physical pain and emotional fatigue in the process of keeping you safe.
How this loop sustains itself
Perception of a threat creates inflammation
Anticipatory salience plus limbic extracellular ATP, P2X7 and IL-1β signalling amplify salience for the feared cue. Avoidance then prevents corrective exposure and keeps the prior high.
Metabolic bias
Sympathetic tilt, mast cell activation and cytokine signalling favour rapid glycogen mobilisation and transient insulin-resistant windows, along with histamine-related symptoms.
Gut feedback
Hypothalamic outputs acutely shift proximal-gut communities and metabolites, modulating adenosine and inflammasome thresholds that influence microglial reactivity and threat learning.
The phobic response to symptoms
"Do not be bluffed by a symptom.
Accept it. Float through it.
Let time pass." - Claire Weekes, MD
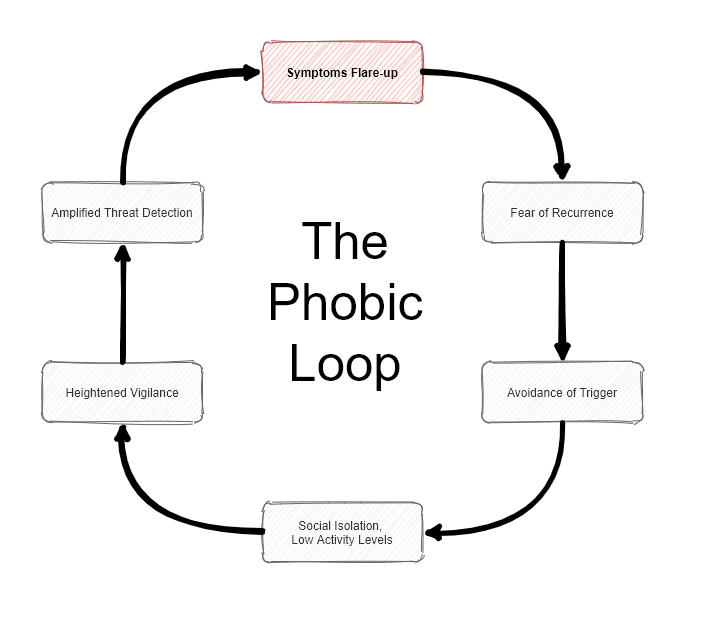
The pattern I call the "phobic loop" has deep roots in biology -
trauma, metabolism, inflammation, sensory gating. However, the
experience of being trapped in that loop isn't new.
Decades ago, a
brilliant Australian physician named Dr. Claire Weekes described a nearly identical cycle [BOOK LINK - highly recommended],
using language like “first fear, second fear,” and explaining how a
sensitised nervous system can become stuck in protective sympathetic overdrive. She
wasn’t simply dismissing symptoms - instead, she was validating them. Her key insight was that the fear of the symptom was more disabling than the symptom itself.
What
she offered patients was a way to float through the storm - not by
ignoring it, but by removing the "fuel": the resistance, the bracing,
the fear of fear. There are similarities to key elements in this section
- restoring safety to the system, not by silencing it, but by helping
it stand down.
Repeated experiences of PEM, MCAS, etc., can result in a conditioned, phobic response to certain triggers. This means that the brain starts to associate specific activities - such as physical exertion or even mental tasks - with symptom exacerbation, leading to an increased fear response. The brain, in a state of chronic stress or "under siege", may misinterpret normal sensations as threats, reinforcing feelings of vulnerability and the development of phobic responses to a wide range of stimuli.
People with strong ADHD and/or OCD-like traits are expected to have a
more difficult time with this, as the subconscious hyper-focus and
pattern-recognition traits can easily be fixated on the symptoms,
instead of the recovery progress. As an analogy, I'm reminded of a lesson once given by my motorcycle riding instructor:
When
riding a motorcycle, you seamlessly "merge" with the bike, to the point
that wherever you're looking is where the bike will travel towards.
Imagine a scenario where you're riding a motorbike around a large
paddock that has a single tree in the middle of it. The paddock is so
large that there is absolutely no reason that the tree should present a
significant risk of collision - you have a lot of wide open space to
enjoy. However, if you're consciously or subconsciously afraid of
hitting the tree, you'll keep glancing or looking over at it to make
sure you're safe. Consequently, by these actions, you'll increase the
risk of actually hitting the tree, or perhaps succeed in doing so. By
simply focusing on the wide open space where you want to actually be
riding, you will be significantly safer and enjoy your ride more.
This lesson applies to ME/CFS in the same way: don't focus on the symptoms - focus on the destination. Trust your body. The symptoms that we worry about the most may persist the longest. We give energy and life to things by paying attention to them.
It's important to understand that your symptoms are NOT imagined - they’re real, measurable, and rooted in biology. Whereas, HOW your nervous system INTERPRETS and AMPLIFIES those symptoms can change the entire trajectory of the illness.
In other words, it's NOT "in your head", it's "through your nervous system" ...and that gives us tools to work with.
The loop is debilitating, but not irreversible. Every loop has a way out - and that’s what this section is about.
Steps towards recovery
Several strategies can help people with ME/CFS, etc., navigate the complex interplay of physical, neurological and psychological symptoms:
Recognising the Role of the Mind
Understanding the powerful connection between the mind and body is crucial. Unregulated fear can perpetuate symptoms, so addressing these emotions is an essential part of recovery.
Perceptual Recalibration
Graded stressor exposure with interoceptive control to reduce salience-hypothalamus coupling to the cue. Expect the transient innate lymphoid cell signature to normalise as exposure succeeds.
Purinergic Damping
Aim to lower extracellular ATP signalling or raise adenosinergic tone conceptually. This is an area being actively researched. Early data suggests the inosine + adenosine synthesis, which acts as the dampening signal to extracellular ATP is dysregulated by impaired glycolysis, pentose phosphate pathway, methylation, acidosis and low glutamine:glutamate. Inosine is included in the protocol to help regulate this imbalance.
Autonomic Gating
Slow nasal-breathing or baroreflex-oriented work to raise RMSSD and blunt post-prandial adrenergic spikes, then re-test symptom provocation.
Gut Microbiome Modulation
Increasing fermentable-fibre intake and other microbiota-supportive tactics in the post-exposure window can exploit the short hypothalamus → microbiota latency and stabilise feedback metabolites.
Daily Mantras / Replacing Unhelpful Thoughts
This can help re-frame negative thoughts and beliefs about symptoms, thereby removing unnecessary obstacles, fears and anxiety, eg.
1. "This is a chapter in my life, not the whole story."
This
mantra puts the illness experience into perspective, reminding people
that their lives are not defined by their symptoms. It encourages them
to look beyond the present moment and envision a future filled with
possibility. It helps to counteract the sense of hopelessness that can
accompany chronic illness. It reminds people that their lives are still
unfolding and that their illness, while a significant challenge, does
not have to define their identity or their future.
2. "I choose to focus on what I can do, not what I can't."
This
mantra promotes a positive outlook and encourages individuals to find
joy and fulfillment in the present moment, even within the constraints
of their illness. This affirmation helps to shift attention away from
limitations and towards possibilities. It encourages people to explore
activities that bring them joy and a sense of accomplishment, however
small, to counteract the sense of loss and frustration that can
accompany chronic illness.
3. "Every step I take, no matter how small, is a victory."
This
mantra celebrates small wins and acknowledges the courage it takes to
move forward even when faced with fear and uncertainty. It encourages
people to appreciate their efforts, no matter how seemingly
insignificant. It emphasizes that progress is not always linear and
that even small steps forward contribute to overall healing.
4. "I am not alone in this journey."
This
mantra reminds people that they are part of a larger community of people
who understand their struggles. It helps to combat feelings of
isolation and foster a sense of belonging. It underscores the importance
of connecting with others who have experienced the challenges of living
with ME/CFS. Sharing experiences, offering support, and learning from
one another can be a powerful source of healing and hope.
5. "I am learning to listen to my body with kindness and curiosity."
This
mantra encourages a compassionate and non-judgmental approach to
symptom management. It fosters a sense of collaboration with the body
rather than seeing it as an adversary. This affirmation helps to shift
the internal dialogue from one of self-criticism and blame to one of
understanding and acceptance. It encourages people to pay attention to
their body's signals and respond with care and compassion.
6. "My body is healing, even when I can't see it."
This
mantra fosters patience and hope, reminding people that recovery is a
process that may not always be visible. It encourages trust in the
body's innate capacity to heal. It helps to counteract the
discouragement that can arise when progress feels slow or setbacks
occur. It reminds people that healing is happening on multiple levels,
even when it's not immediately apparent.
7. "My symptoms are a signal, not a sentence."
This mantra helps to re-frame symptoms as messengers rather than threats. It acknowledges that symptoms are trying to communicate something, but they don't dictate the future or define one's limitations. It draws on the idea that pain, fatigue, and other symptoms in ME/CFS are often amplified by fear and anxiety. It encourages a shift in perspective from viewing symptoms as inherently dangerous to seeing them as signals that need to be understood and addressed.
8. "I am safe, even when I experience symptoms."
This mantra directly addresses the fear response, offering a powerful message of reassurance. It emphasizes the distinction between experiencing a sensation and being in actual danger. It is particularly helpful in breaking the cycle of fear and avoidance. By repeating this affirmation, people can begin to retrain their nervous systems to associate symptoms with safety rather than threat.
9. "I am stronger than my fear."
This mantra
empowers people to face their fears and challenge the limitations they
have imposed on themselves. It emphasizes that fear does not have to
control their lives. This affirmation promotes self-efficacy and
encourages individuals to take an active role in their recovery. It
reminds them that they have the inner strength to overcome their fears
and gradually expand their boundaries.
These mantras, when repeated regularly and with intention, can help to rewire the brain's threat response, reduce anxiety, and foster a sense of safety and empowerment in the face of challenging symptoms. With practice and persistence, belief in these mantras strengthen. It only takes a few wins or reductions of something to see this approach is helping.
Gradual Exposure and Pacing
Gradually increasing exposure to normal activities and day-to-day life, along with appropriate pacing, can help desensitize the nervous system and break the fear-avoidance cycle.
Emotional Processing
Techniques such as journalling, therapy, or other methods for exploring and expressing emotions can be key in addressing underlying emotional issues that may contribute to symptom persistence. Recovery is not linear. Record your wins as a list. On bad days go back to the listed wins list and focus on the positive.
Somatic Practices
Practices like mindfulness, gentle movement, and breath-work can help people with ME/CFS develop a greater sense of safety and connection with their bodies, shifting the nervous system from sympathetic to parasympathetic mode.
Try this:
Place your hand over your chest and breathe slowly into your ribs for 10 seconds.
As you exhale, say (in your head, or aloud): "I’m safe. I’m adaptive."
Happily, this isn't about "magic thinking" - it's reprogramming the body's fear interpretation loop through safe, predictable signals.
Self-Compassion
Cultivating patience and kindness towards oneself during the recovery journey is crucial, as ME/CFS recovery can be a slow, non-linear and challenging process.
Building Social Support
Connecting with others who understand the experience of ME/CFS and critically, are supportive of the process you are undertaking and / or are ideally further along the same recovery process than you, can reduce feelings of isolation, provide validation, and offer emotional peace.
Recovery from ME/CFS is a deeply personal journey of "putting Humpty Dumpty back together again". Everyone has slightly different shaped pieces to reassemble.