Yeasts, moulds and fungi are found everywhere in nature and have an important role. They decompose animals, plants and other organisms, recycling their elements and other nutrients, thereby continuing the circle of life.
Usually, these decomposing animals are not alive, however when an organism’s immune response is incapable of maintaining a defence against the normal daily background level of fungal challenge, the living organism will become food for yeast, mould and/or fungi. Various lifestyle influences contribute positively and negatively to maintaining this daily defence.
Lack of exposure to sunlight, lack of sufficient activity to maintain a specific immune function and/or lack of a balanced, protective microbiome can also contribute to an organism being more susceptible to mould. It has been previously said “we don’t grow old, we mould!”
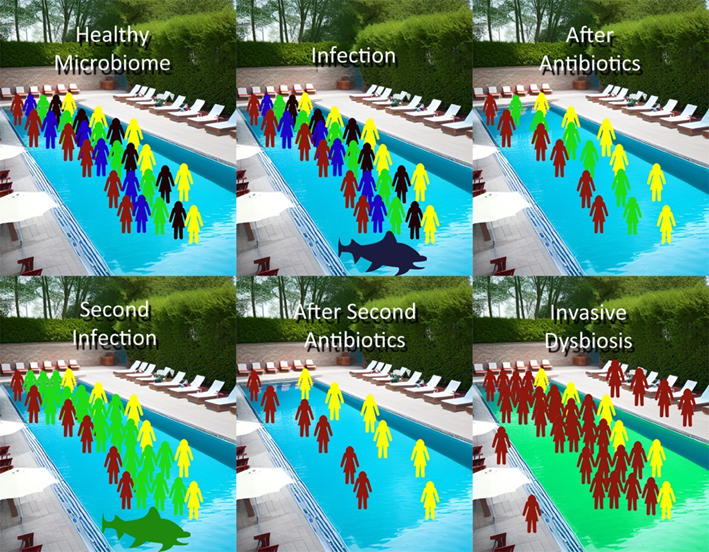
Antibiotics are powerful tools in controlling bacterial infections, however they are also broadly indiscriminate in their effects and are overused in food production + minor infections, leading to a loss of microbiome diversity and also the development of drug-resistant strains. Acute use of them decreases systemic levels of both "good" and "bad" bacteria, creating opportunities for opportunistic fungal overgrowth. Without paying careful attention to diet, probiotics, prebiotics and host metabolism, using broadly destructive interventions against your microbiome can have deleterious effects on your health and happiness.
eg. If you pour weedkiller all over your garden, killing almost all of the flora and then don't replant and cultivate the garden again afterwards, you'll find that over a short time, the plant life now growing back is made up of the most hardy, versatile, adaptable species either left behind or reintroduced by natural processes. These are often the species of weeds you were trying to remove in the first place.
Growing a beautiful garden means making space for what you want to flourish, planting the seeds and then feeding the species you want to keep, so they can out-compete the others. Selective weeding is also helpful. Some fertilisers are selective for species, also. These will be discussed in the Probiotics and Prebiotics sections below.

Maintaining a protective gut microbiome in modern times has a number of challenges due to the germicidal effects of stomach acid, metabolic acidemia and chronic disconnection from our natural source of probiotics via our industrialised food chain / use of preservatives and general preference for cooked food.
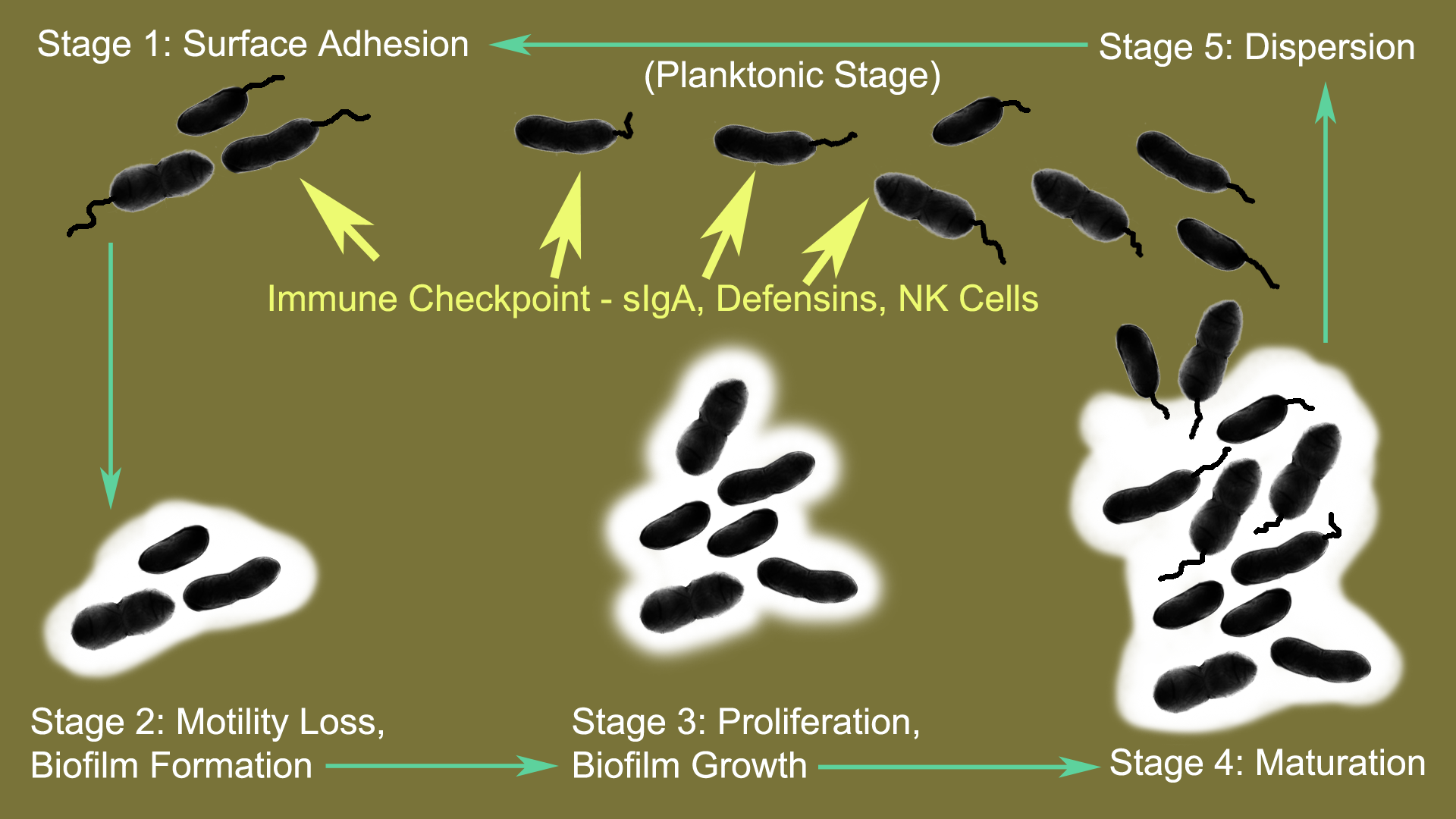
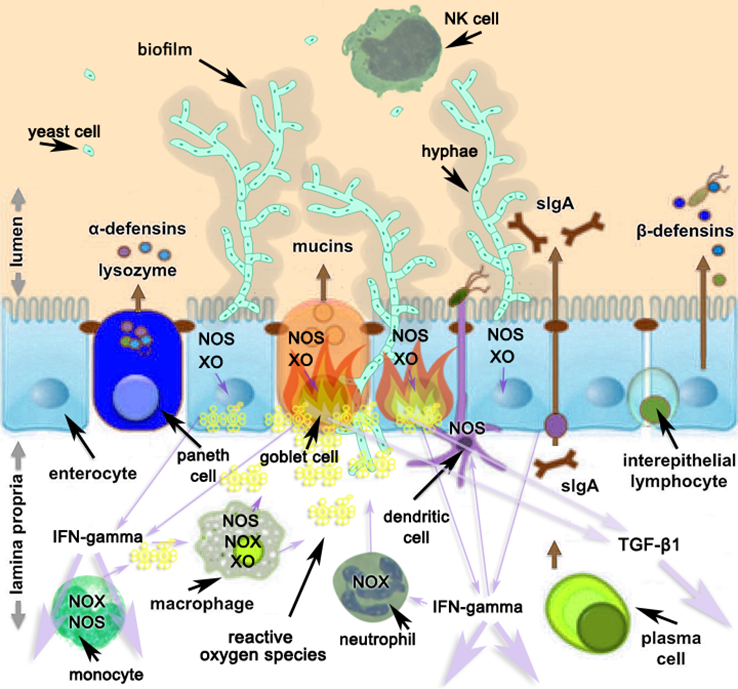
The barrier function of the skin and mucosal layers play an important part in resilience against pathogens. Unfortunately, the human body has a number of tissues that are opportunistic for yeast / mould / fungal and bacterial infections to thrive with minimal interference from direct immune activity, thanks to their ability to form biofilms.
https://www.sciencedirect.com/science/article/pii/S0016508524050546
Subgrouping for ME/CFS, PFS, PSSD and other patients may have a
relationship with the locations of infected tissues. Localised
pathogenic biofilm accumulation and chronic innate immune activation.
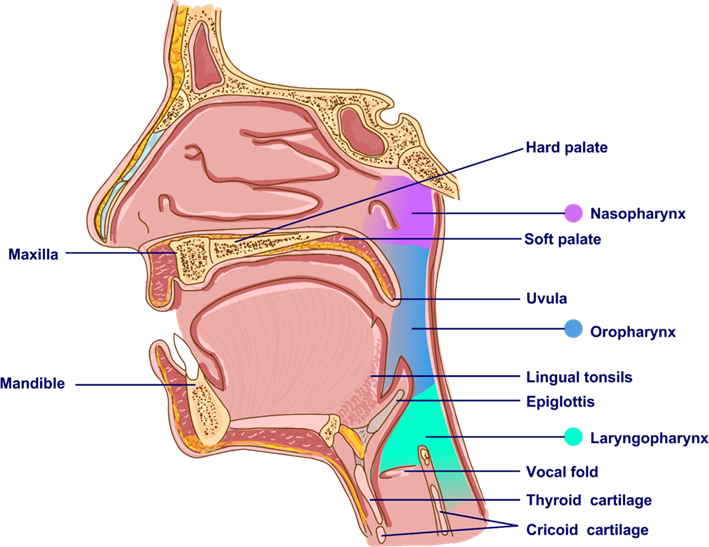
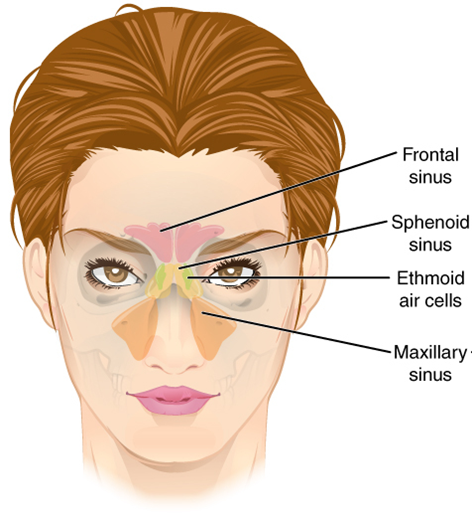
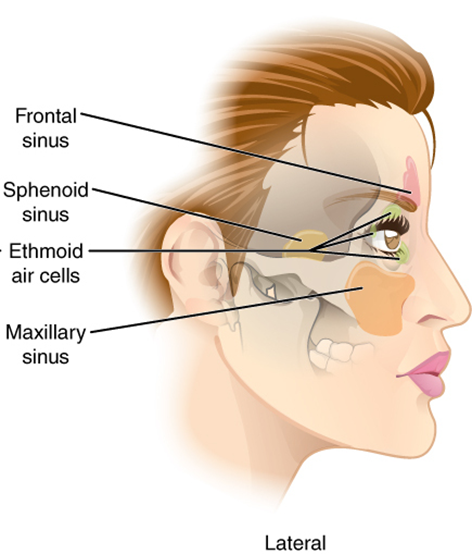
Nasopharnyx
One example for possible subgrouping relates to the nasopharynx (and surrounding areas), which have a direct route to the central nervous system and also potentially prevents critical signalling from normal nasal breathing, which creates a balanced parasympathetic : sympathetic tone. (see "2.2.6 Cortisol, limbic system, glycogen and IFN-γ - Sympathetic overdrive")
Swollen / enlarged lymph nodes can often be found nearby infected tissues. If these blocked lymph nodes include the nasopharyngeal, occipital and cervical vessels in the neck and face, then crippling intracranial pressure can also be expected, as these nodes regulate intracranial pressure. This can cause debilitating pain, also creating a blocking issue / preventing remineralisation unless resolved beforehand. You can read more about this topic in 2.2.2 Lymphatic maintenance.
Do you have a history of cracked lips / ears / toes / feet / rectum,
flaking skin, severe acne, dandruff, hair loss, red / inflamed skin patches / rashes,
eczema, psoriasis, nasal inflammation, tonsillitis, sleep breathing
disorder, gut pain / issues, cystitis, prostatitis, mastitis,
epididymitis, white or green/black film on tongue or discharge?
These are strong indicators for potentially invasive microbiome dysbiosis. The extent / severity of the invasiveness of these microbes has a direct correlation with the intensity and duration for activation of chronic innate immune response pathways. These alter energy metabolism towards specific immune functions and generate predictable symptoms, such as neurotransmitter and endocrine dysregulation, POTS, dysautonomia, elevated cholesterols, insomnia, frequent urination, etc., especially where coenzyme or mineral deficiencies are also present.
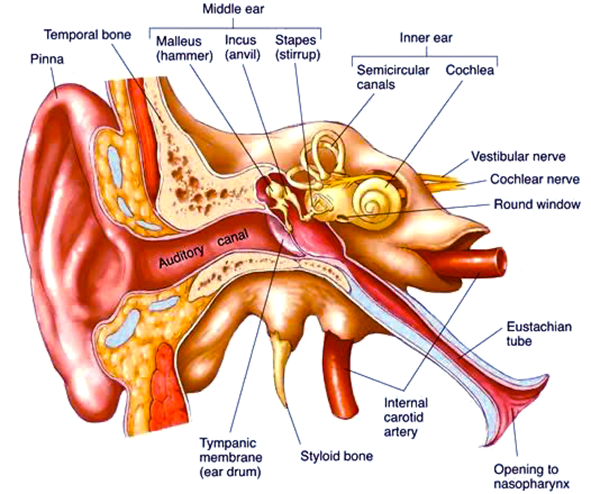
Orifices and tissues such as the nasopharynx, sinuses, throat, Eustachian tubes, ears, GI tract, rectum, vagina, feet, toes are areas which are not regularly exposed to direct sunlight. This list might well include all tissues, where someone is bed-bound or house-bound. These tissues provide “safe spaces” for any pathogenic microorganisms to colonise, create biofilms and thrive, without appropriate immune surveillance.
{kind=link}
{kind=link}
Gastrointestinal biofilms and pathogens
In the case of a GI tract infection, this may also
affect dietary absorption efficiency and cause endotoxemia, sometimes
leading to gastroparesis, nausea / vomiting in response to food
consumption, along with other potential systemic impairments.
The timing of symptoms onset, in relation to meals may be helpful in identifying the location of unhelpful biofilms / colonies and also which interventions may be the most appropriate. Generally, the shorter the duration between meals and symptom onset, the closer the biofilm / overgrowth is to the stomach.
Upper GI / small intestine dysbiosis / overgrowth may benefit from oral dosing of specific biofilm breakers and related interventions, whereas lower GI / large intestine dysbiosis / overgrowth can be more easily targeted by administration of eg. robusta coffee enemas.
Similarly, upper GI microorganism colonies bloom in response to dietary intakes of simple sugars, BCAAs, etc., whereas colonies in the large intestine benefit more from more complex carbohydrates and proteins, which break down into simple sugars and BCAAs further along the digestion journey.
Upper GI biofilms containing overgrowth of fermenting species can produce toxic gases that are known to cause inflammation, epithelial damage and sphincter dysfunction, which is further connected to reflux / GERD.
Vitamin U (some example supplements - [AU] | [US] | [EU]) also known as S-methylmethionine or DL-methylmethionine, specifically as cabbage juice for bioavailability in the upper GI) was the primary treatment for reflux prior to proton pump inhibitors - primarily as a tissue-restorative intervention and arguably better.
https://pubmed.ncbi.nlm.nih.gov/12671885/
https://pmc.ncbi.nlm.nih.gov/articles/PMC12133511/
Different strategies are needed for different parts of the GI tract.

[adapted from source: https://in.pinterest.com/pin/640355640799063911/]
This protocol currently includes a number of staged interventions to address biofilms and pathogens in different locations inside the GI tract, such as Candex, Biofilm Phase 2 Advanced, NAC, spirulina, curcumin, fulvic acid, prebiotics, targeted probiotics, biofilm flushes, dietary interventions and water-fasting, with an aim of not unduly circulating endotoxins / acetaldehyde in the process of eliminating them, if at all possible. These strategies have been testing well and we are always exploring ways to improve on this process (please join the Discord online community to join the discussion).
Professional endoscopic biofilm removal is possible, however there appears to be a significant problem with general awareness of biofilm issues amongst gastoenterologists, so finding a willing clinician is currently challenging. A paper and video of removal here - https://x.com/joshual_tm/status/1825355958568304834
One of the key challenges is that invasive microorganisms which breach the (mucosal) barrier function can trigger an IFN-γ response, which causes collateral damage and inflammation to infected tissues in the process of oxidising pathogens, using reactive oxygen species.
If the rate of collateral oxidative damage + pathogenic damage exceeds the regenerative capacity of the tissue, this could further compromise the barrier function and dysregulate IFN-γ activity, leading to a “deadlocked” cycle / state. External indicators for insufficient collagen synthesis rates may include hEDS symptoms, poor skin texture, chronic cranial instability, slipped rib syndrome, thoracic outlet syndrome, etc.
A healthy microbiome appears to play a very important role in providing protection against invasive bacterial, yeast, mould and fungal infections.
Chronic illnesses, including Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) and various inflammatory or metabolic diseases, are frequently associated with gut dysbiosis. A key feature of this dysbiosis is often the reduction of butyrate-producing bacteria and an increase in fermentative species.
https://pmc.ncbi.nlm.nih.gov/articles/PMC12564589/
This loss of butyrate producing species appears to have a strong relationship with (lactic) acidaemia / acidosis and pH drop in the lumen.
Although there is human clinical data showing a 2-3 fold increase of rectal luminal lactate in settings like cardiopulmonary bypass and severe sepsis, this is largely discussed as reflecting mucosal metabolic dysfunction/ischemia (local production and barrier dysfunction), rather than “lactate being intentionally transported into the gut for disposal” and the exact mechanism is unclear.
https://pubmed.ncbi.nlm.nih.gov/16199418/
https://pubmed.ncbi.nlm.nih.gov/17116255/
Normally, lactate is discussed in the other direction of gut-derived lactate entering the system. Mechanistically, lactate is absolutely transportable across gut epithelium. Monocarboxylate transporters, eg. MCT1, SLC16A1 are proton-coupled and are reported as being located on both lumen-facing and basolateral membranes in intestinal epithelium, meaning the flux direction depends on concentration gradients and the local pH gradient.
https://pmc.ncbi.nlm.nih.gov/articles/PMC11748985/
https://pmc.ncbi.nlm.nih.gov/articles/PMC2835396/
https://pmc.ncbi.nlm.nih.gov/articles/PMC6019286/
For lumen pH - the GI tract is already running strong pH control via acid secretion (stomach) and bicarbonate secretion/transport (small intestine, colon). Papers on intestinal bicarbonate transport describe that these processes regulate luminal pH (and the epithelial surface microclimate in particular).
https://pmc.ncbi.nlm.nih.gov/articles/PMC11006743/
https://journals.physiology.org/doi/full/10.1152/ajpgi.00341.2014
The baseline luminal pH varies quite a lot by segment in the GI tract - roughly 6.5 in the proximal small bowel rising toward 7.5 by ileum, dropping near the caecum (fermentation acids), then rising again toward the rectum. This might provide the theoretical gradient in specific sections under the right circumstances and needs more study.
However, there’s also decent evidence that systemic acid-base status changes colonic mucosal intracellular pH and bicarbonate-related handling, and that systemic pH (and bicarbonate/PCO2) can modulate colonic transport processes. This is also a route by which systemic acidosis could indirectly shift luminal pH near the mucosa, even if the bulk lumen is buffered by diet, secretions, and microbial metabolites.
https://pubmed.ncbi.nlm.nih.gov/3925792/
https://journals.physiology.org/doi/abs/10.1152/ajpgi.1983.245.2.G230
https://gastrojournal.org/article/S0016-5085%2896%2900459-3/pdf
Overall, “more study is needed” around how this mechanism works.
Butyrate is a short-chain fatty acid (SCFA) produced by specific gut microbes through the fermentation of dietary fibers. It serves as a primary energy source for colonocytes, contributes to the integrity of the gut barrier, and exhibits anti-inflammatory properties. A decline in butyrate-producing species can compromise the gut lining and increase systemic inflammation. Butyrate influences various pathways to support gut health, including fortifying epithelial tight junctions, inducing regulatory immune cells, and affecting metabolism and the nervous system. Adequate butyrate also aids in stabilising hypoxia-inducible factor (HIF) to promote mucosal healing. The loss of these organisms is linked to reduced fecal butyrate concentrations and worsened intestinal inflammation and permeability in chronic disorders.
Key butyrate-producing species primarily belong to the Firmicutes phylum (Clostridiales order) and include Faecalibacterium prausnitzii, Roseburia spp. (e.g., Roseburia hominis), and Eubacterium rectale. These species collectively contribute significantly to colonic butyrate production. In conditions like ulcerative colitis, irritable bowel syndrome (IBS), and ME/CFS, a reduction in these butyrate-producers is consistently observed.
Conversely, an overgrowth of fermenting species often occurs. These microbes ferment carbohydrates into substances such as lactate, ethanol, hydrogen, and carbon dioxide, which can exacerbate bloating, D-lactic acidosis, and gastrointestinal discomfort. Common fermenters include D-lactic acid bacteria like Enterococcus and Streptococcus, which can produce substantial amounts of lactic acid. Prevotella spp., while capable of fermenting fiber, primarily produce acetate and propionate rather than butyrate, and their overgrowth alongside reduced butyrate-producers may indicate an inefficient cross-feeding network. Proteobacteria (eg. Escherichia, Klebsiella, Enterobacter) can also expand during dysbiosis, potentially driving inflammation and endotoxin release. Yeasts, such as Candida, can also ferment sugars to alcohol and gas, contributing to dysbiosis. There is a large table of fermenting species in the microbiome testing section and a tool to analyse Biomesight report data.
https://link.springer.com/article/10.1186/s12866-025-04650-9
Apart from generating gaseous toxins, ethanol and acetaldehyde -
depleting silicon and other metals in compensation, many yeasts / mould /
fungi and bacteria can cause dramatic metabolic alterations. They have
an ability to break through our skin / epithelial tissue / mucosal
barrier function from immune-evasive biofilms and cause recurring /
chronic immune activation during the invasion. This immune activation
inhibits specific mitochondrial metabolism and reconfigures a number of
other metabolic pathways toward combating these pathogens. However,
while ultimately beneficial, these alterations can be quite
debilitating, under certain conditions.
Consequences of fermenter overgrowth include small intestinal bacterial overgrowth (SIBO), leading to bloating, gas, and malabsorption in the upper gut. In the colon, lactate accumulation can excessively acidify the lumen, inhibiting beneficial species and potentially causing mucosal injury. Metabolic by-products from an over-fermenting microbiome, such as ethanol and ammonia, can burden the liver and impair cognitive function. Normal cross-feeding, where lactate and acetate from fermenters like Bifidobacteria or Lactobacilli are used by butyrate-producers, is disrupted, leading to the accumulation of intermediate metabolites.
A multifaceted approach is necessary to rebalance the microbiome in chronically ill patients, focusing on reintroducing or stimulating butyrate-producing species, providing appropriate substrates, potentially supplementing beneficial metabolites, and reducing fermentative overgrowth.
A phased approach for rebuilding the gut microbiome typically involves:
Phase 1 - “Clean Slate” (1-4 weeks)
If significant dysbiosis is suspected or quantified, measures to reduce pathogenic and fermentative load are initiated. After onboarding the standard protocol interventions to stabilise the metabolism, this may include a 7-14-day course of rifaximin or nifuroxazide for SIBO and/or 4+ weeks of herbal antimicrobials. Bacteriophages can be very helpful. A gentle, gut-friendly diet (e.g., low-FODMAP temporarily) is implemented concurrently to reduce fermentable substrates. Bowel regularity should be ensured.
Phase 2 - Reseeding and Feeding (Weeks 2-12)
This phase introduces probiotics and prebiotics. A high-quality multi-strain probiotic is started once antibiotics are completed, or concurrently if using antibiotic-resistant strains like S. boulardii. Prebiotic fibers, such as partially hydrolysed guar gum (PHGG), are introduced gently and increased gradually, aiming for 10-15 grams daily through diet or supplements. Oral butyrate supplements can also be slowly started and once well-tolerated, replaced with butyrate producing probiotics. The diet transitions to a more diverse, fiber-rich pattern, incorporating fermented foods cautiously. By the end of 3 months, some improvements are expected, but sustained effort may be needed for deeper shifts.
Phase 3 - Maintenance and Monitoring (3 months and beyond)
The focus shifts to maintaining healthy habits and potentially tapering supplements. A high-fiber, diverse diet should be continued indefinitely. Probiotics may be continued for 3-6 months or longer, possibly at lower maintenance doses. Butyrate supplementation and foods can be continued if beneficial. Objective markers like fecal butyrate levels and keystone microbial species, along with subjective improvements in stool form, bloating, energy, and cognitive function, are monitored. Setbacks due to new infections or medications are managed by temporarily adjusting the protocol.
Realistic expectations are important, as rebuilding the microbiome is a gradual process. Initial improvements in digestive comfort may be felt within 2-4 weeks. More robust changes, such as stabilised stool patterns and improving energy, are expected by 8-12 weeks. Long-term remodeling can take 6-12 months, potentially leading to increased activity levels and overall resilience. While not all core chronic illness symptoms may fully resolve, most patients can achieve improvements in gastrointestinal symptoms and nutritional status.
More information on each intervention can be found in related sections below.
Tailoring gut microbiome therapies for frail, home-bound patients is critical. Here are some of the key considerations:
#1 - Start Low and Slow
Introducing fibers, probiotics, or any supplement gradually (e.g., ¼ of the intended dose, increasing every few days) helps the gut adjust and prevents symptom exacerbation.
#2 - Hydration and Diet Texture
Adequate water intake is essential with increased fiber. Fibers can be incorporated into soups, purees, or powders for easier consumption if chewing or digestion is impaired.
#3 - Monitoring Nutritional Status
Repleting nutrient deficiencies (e.g., vitamin D, B12, magnesium, protein) before starting is critical for gut healing.
#4 - Contraindications
High-fiber diets should introduced slowly in cases of intestinal obstruction or stricture. Probiotics should be used cautiously and with medical clearance in severely immunocompromised patients or those recently post-surgery.
#5 - Herxheimer-like Reactions
Patients will likely experience transient "die-off" symptoms (fatigue, headaches, rashes) when the microbiome shifts. Slowing down the intervention or using supportive measures like binders may be helpful.
#6 - Bed-bound Logistics
Administering supplements (powders, open capsules) and enemas may require caregiver assistance and planning.
#7 - Medication Interactions
Be aware that medications like antibiotics, acid blockers, and opiates can affect the gut microbiome. Probiotics like Saccharomyces boulardii can be used during antibiotic courses.
Mammary glands and lactiferous ducts are present in both male and female anatomy. A less well-known fact is that males
are also capable of lactating under unusual circumstances that involve
low dopamine and elevated prolactin. These tissues are also another common area for microbial
biofilm formation.When diagnosed with an infection, this is known as
non-lactational mastitis.
Collecting any data on this microbiome is rather difficult when not lactating. It's possible that repurposing eg. MicroGenDX's WoundKEY panel could be useful, if a sample can be obtained.
For women, where biofilms in these microbiomes contain pathogenic species, it is expected that immune activity and inflammation in these (and any other infected) tissues will ramp up during oestradiol elevation, by allowing more IFN-gamma activity.
This immune activity elevation occurs as a short spike during pre-ovulation and for a range of days during the second half of the luteal phase, pre-menses. (see "2.2.7 Reproductive-health")
Sore and bumpy breasts during these times are common and inflammation may be observed in both the mammary glands and lactiferous ducts, with or without accompanying swollen inframammary, anterior axillary and parasternal lymph nodes.
While traditionally, many women have received advice about reducing oestradiol levels to prevent these symptoms, this logically leads to persistence of the infection.
Working with the body's natural signalling, while helping to manage the localised biofilm, oxidative stress and pathogens may help you break out of this unpleasant monthly cycle.
Topical use of 70% DMSO / 30% water (or 30% aloe vera gel), as a transport enhancer, combined with various biofilm breakers and anti-microbial interventions listed in this protocol may be an effective way to shorten this journey. This intervention can also be used with other tissues.
NB. DMSO is expected to create a localised histamine response when applied to skin, which will feel itchy for a short period. It's best applied with clean hands or gloves.
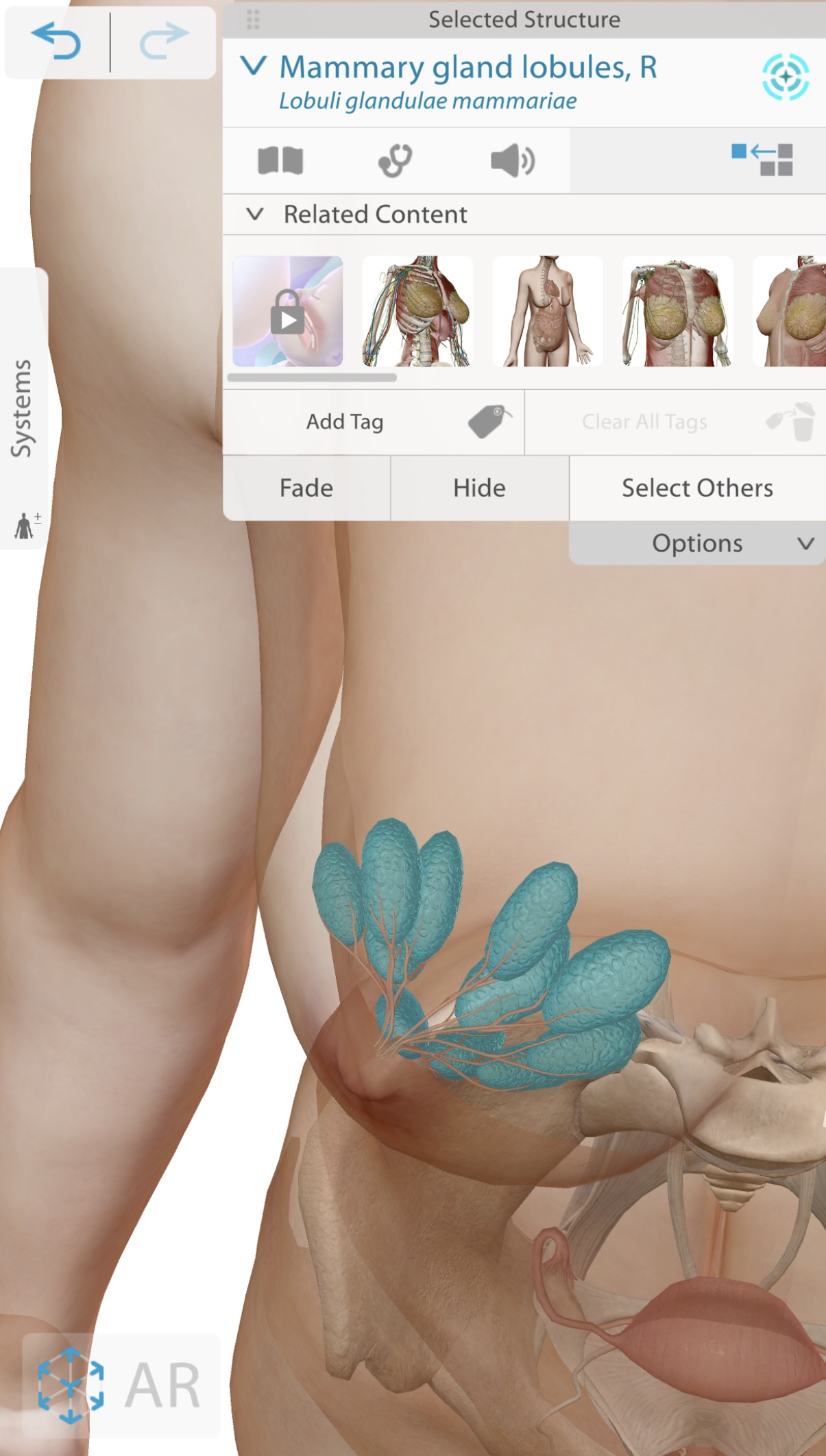
[source: Human Anatomy Atlas, by Visible Body.]
Parasites
Co-infections of flesh-eating parasites such as worms, flukes, amoebas, etc.,
can temporarily induce severe ME/CFS symptoms by directly attacking the
epithelial layer and allowing opportunistic invasion by any/all
microbial species.
Any of these can become systemic and create a chronic, recurring immune response in different tissues.
If you suspect you have a parasitic infection, over-the-counter
and/or prescription pharmaceutical interventions such as ivermectin,
fenbendazole, mebendazole, albendazole, methylene blue and pyrantel may be appropriate.
Some of these anti-parasitics also have anti-fungal and other
properties. This often applies vice-versa, too. These are commonly taken as either a single or multi-dose
intervention by all inhabitants of a household, per your pharmacist’s or
doctor’s advice.
For other species, such as amoebas, paromomycin and similar prescription drugs can be highly appropriate. Additionally, various herbal products based on black walnut, cloves and wormwood have also shown as highly effective, eg.
https://www.australianhealthfoods.com/product/ppc-herbs-herbal-tri-plex
The GI-Synergy product in Stage 2 already includes many of these ingredients.
(WIP: This section is being actively worked on to improve interventions for Bartonella, Borrelia, Babesia, Toxoplasma and some other species. Updates are coming.)
Profile: Toxoplasma gondii
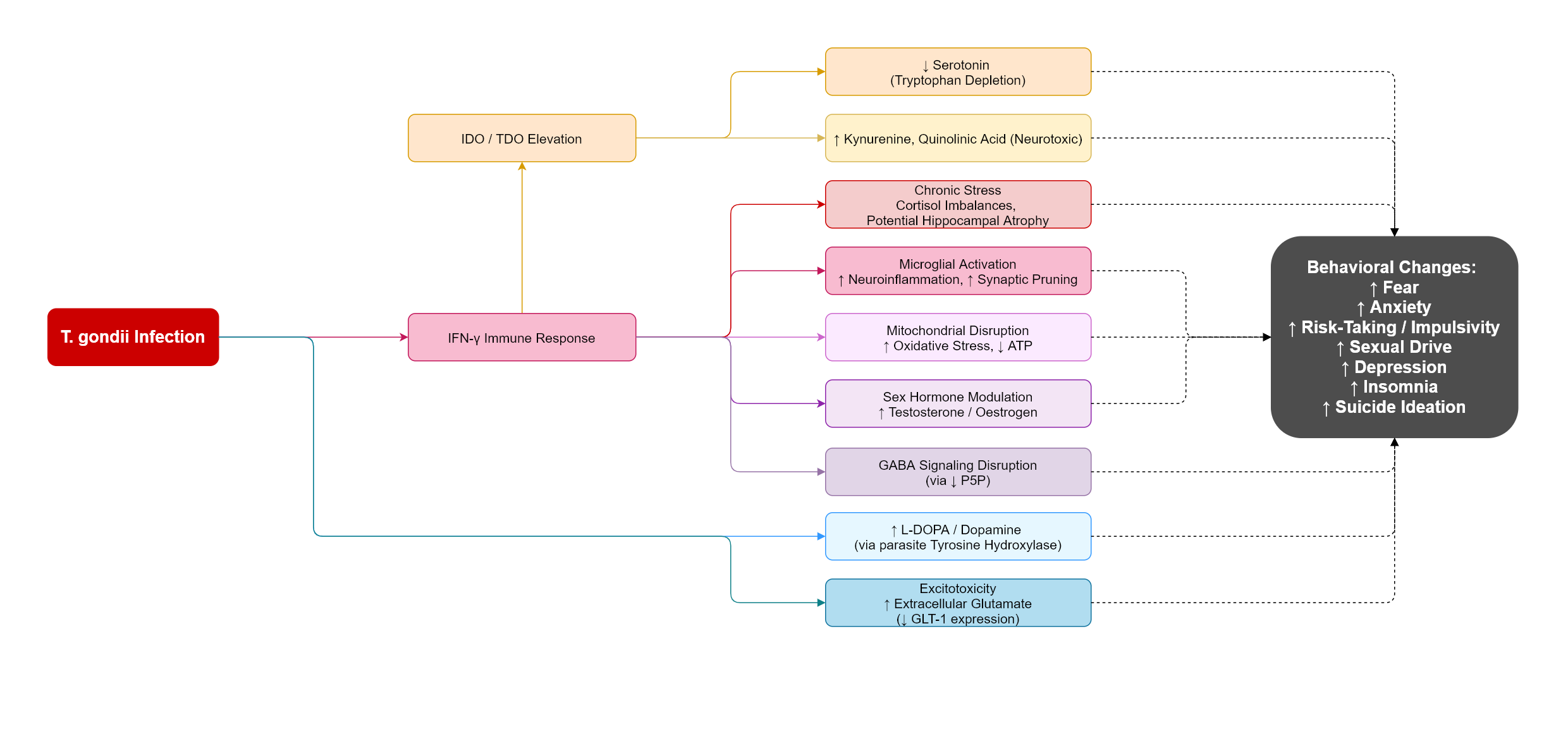
Toxoplasma gondii is a protozoan parasite notable for its capacity to establish lifelong latent infection, often within neural and muscle tissues. Studies suggest over 50% of the population is infected. In immunocompetent hosts, it typically remains subclinical; however, its persistence in the central nervous system has drawn increasing attention due to its association with measurable alterations in behaviour and neurochemistry. Rather than eliciting overt pathology, the organism maintains a long-term presence through intracellular cysts, accompanied by a sustained, low-grade immune response that may itself become a source of chronic neuroinflammatory stress.
The host immune response is predominantly mediated by interferon-gamma (IFN-γ), which activates several downstream pathways, including the induction of indoleamine 2,3-dioxygenase (IDO) and tryptophan 2,3-dioxygenase (TDO). These enzymes degrade tryptophan, limiting parasite proliferation but also reducing serotonin synthesis and increasing production of neuroactive kynurenine metabolites. Microglial activation, mitochondrial dysfunction, and disruption of glutamate homeostasis have all been documented in chronic T. gondii infection, with potential consequences for synaptic regulation, oxidative stress, and overall neurotransmitter balance. Additionally, the parasite encodes tyrosine hydroxylase-like enzymes, enabling it to influence local dopamine synthesis directly within host tissue.
While the behavioural implications remain under investigation, multiple studies have identified correlations between latent T. gondii infection and alterations in fear processing, impulsivity, sexual behaviour, affective disorders, and suicidality in humans. These associations appear to be mediated by both direct biochemical interference and immune-driven changes in neurophysiology. Although causality is not uniformly established, T. gondii serves as a representative example of how persistent intracellular pathogens may exert long-term, system-wide influence on neuroimmune and metabolic function, particularly in people with existing co-infections and mineral deficiencies.
T. gondii infections in immunocompromised people may benefit from specific combinations of antimicrobials that target stategic parasitic proteins at different stages of the parasite's lifecycle - cysts, bradyzoites and tachyzoites. Some of these interventions may need to be rotated on a 3-5 day schedule to prevent parasitic adaptation.
NB. At this time, outside of correcting IFN-γ dysregulation, this parasite is not directly targeted by this protocol and is being actively investigated. There are some recent, encouraging studies using off-label medicines and various plant compounds which show high efficacy against some of the more difficult stages of the lifecycle.
Glycocalyx
The glycocalyx is a delicate, gel-like layer that coats the inner lining of blood vessels, forming a vital interface between circulating blood and the vessel walls. Though invisible to the naked eye, it plays an essential role in maintaining vascular health by regulating fluid balance, preventing the unnecessary leakage of substances, reducing friction between blood and vessels, and acting as a communication hub for immune signals. The integrity of this layer is critical for protecting the inner lining of blood vessels and supporting healthy organ function.
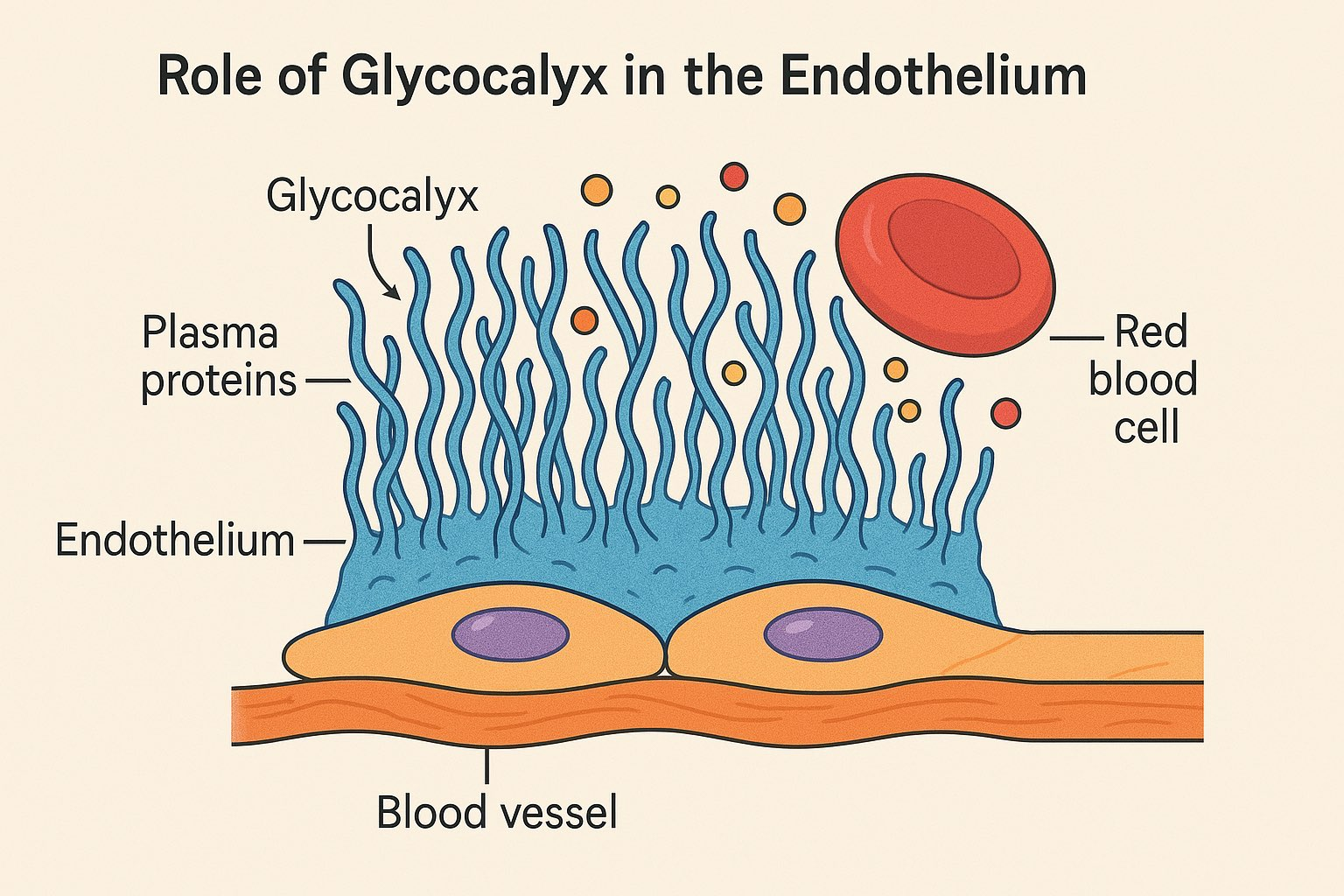
At its foundation, the glycocalyx is made up of complex sugar chains, proteins, and lipids. Its construction begins with basic nutrients: glucose provides the raw material for the long sugar chains called glycosaminoglycans, glutamine fuels the production of nucleotide sugars needed for building these chains, and methylation processes help regulate which parts of the sugar-protein scaffolding are modified or extended. This means that the body’s ability to synthesise a healthy glycocalyx relies directly on having sufficient energy, nutrient availability, and intact metabolic pathways.
However, in chronic diseases where metabolism is compromised, the body’s ability to maintain the glycocalyx begins to falter. In particular, when glycolysis - the process of breaking down glucose to produce energy, hepatic gluconeogenesis - the liver's ability to produce new glucose and Pentose Phosphate Pathway - which produces PRPP, are all disrupted, the raw materials and energy needed for glycocalyx upkeep become limited. This is especially problematic in conditions involving a persistent immune response, such as low-grade bacteremia, where bacteria or bacterial components circulate at low levels and chronically stimulate the immune system. The immune system, in turn, can damage the glycocalyx both directly and indirectly through the release of inflammatory signals and enzymes.
This sets up a vicious cycle. As the glycocalyx erodes, the tight
junctions between endothelial or mucosal cells become leaky. This
increases the permeability of blood vessels and mucosal barriers like
the gut lining, allowing more microbial fragments or toxins to pass
through, which further activates the immune system. With each cycle, the
body becomes increasingly inflamed and less capable of repairing the
very barrier that protects it. In this way, the health of the glycocalyx
becomes both a victim and a regulator of chronic disease processes,
especially in conditions marked by sustained inflammation, microbial
presence, and metabolic dysfunction. Preserving or restoring the
glycocalyx may therefore be a key strategy for breaking this cycle and
supporting overall recovery.
Where glycolysis is impaired, glycoalyx assembly can be supported by dietary sources of N-acetylglucosamine (GLcNAc, NAG) and hyaluronic acid (HA), however functional methylation and sufficient manganese, magnesium and phosphate are also required.
Human studies on NAG in Multiple Sclerosis and other diseases have shown favourable results.
NB. NAG is also beneficial to a range of helpful and unhelpful species, eg. Aggregatibacter actinomycetemcomitans, Akkermansia muciniphila, Arthrobacter bussei, Bacteroides caccae, Bacteroides thetaiotaomicron, Bifidobacterium bifidum, Bifidobacterium infantis, Bifidobacterium longum, Candida albicans, Enterococcus faecalis, Escherichia coli, Faecalibacterium prausnitzii, Hahella ganghwensis, Lactobacillus casei, Lactobacillus rhamnosus, Methanobacterium spp., Pseudomonas aeruginosa, Staphylococcus aureus and Streptococcus mutans. NAG dosing can be taken sublingually, if necessary.

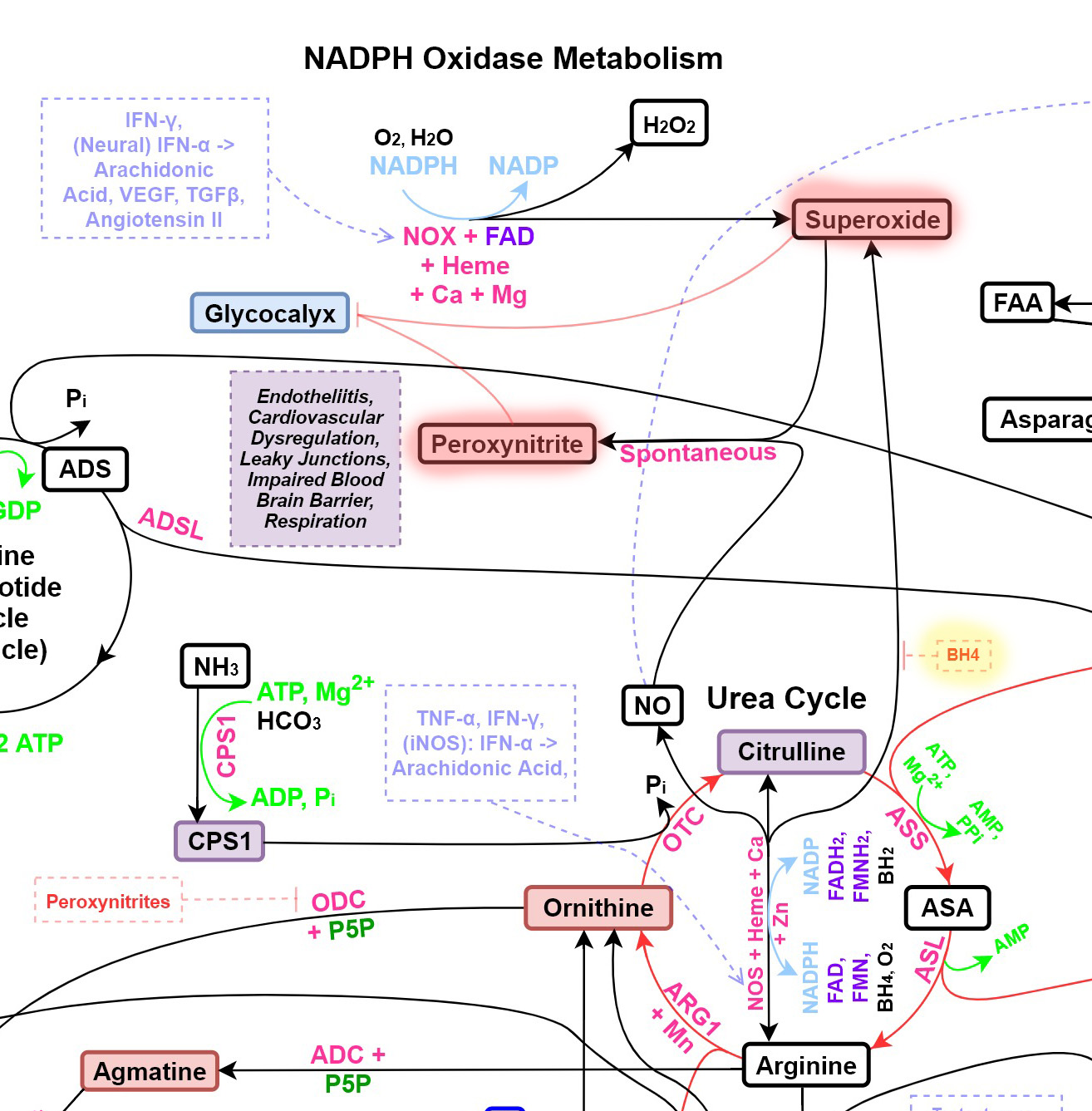
One of the less visible yet deeply consequential ways the immune system can affect the glycocalyx involves the production of reactive molecules. In response to chronic infection or even low-grade bacterial presence in the bloodstream, the immune system normally ramps up interferon signaling. These interferons activate a set of enzymes that include inducible nitric oxide synthase (iNOS) and NADPH oxidase. These enzymes produce nitric oxide and superoxide, respectively - both reactive molecules that in balanced amounts help fight infection. But when produced in excess or under poor metabolic conditions, they can become damaging. Spirulina is a potent NADPH oxidase inhibitor. Curcumin and schisandra are also helpful. Low-dose dextromethophan is an over-the-counter anticholinergic that also acts as a NADPH oxidase inhibitor.
A crucial factor here is a molecule called tetrahydrobiopterin, or BH4. This cofactor is required for nitric oxide synthase (NOS) to properly generate nitric oxide. When BH4 levels are insufficient, which can happen during oxidative stress or nutrient shortages, NOS becomes "uncoupled" and instead of making nitric oxide, it generates more superoxide. This superoxide quickly reacts with any available nitric oxide to form peroxynitrite, a highly reactive and damaging compound. Peroxynitrite can attack lipids, proteins, and DNA, and the delicate glycocalyx is especially vulnerable to this kind of oxidative onslaught.
Compounding this problem is the state of the microbiome. A healthy microbiome contributes to the host in numerous ways, including the synthesis and salvage of rare micronutrients like queuine, a modified base that gets incorporated into human tRNA as queuosine. This modification supports proper mitochondrial translation and protein folding, and helps limit mitochondrial production of reactive oxygen species (ROS). When the microbiome is imbalanced or depleted, levels of queuine can fall, impairing mitochondrial function and allowing ROS to accumulate. These reactive species leak into the surrounding environment, adding to the oxidative burden that the glycocalyx must withstand. Rich sources of dietary queuine include coconut water (not heat-treated), wheat germ (gluten), milk (dairy).

In addition to oxidative stress, chronic inflammation also activates enzymes like matrix metalloproteinase-9 (MMP-9), which can directly degrade components of the glycocalyx and the underlying extracellular matrix. MMP-9 is particularly problematic in chronic immune activation, where its expression is upregulated by inflammatory cytokines and sustained by feedback loops involving ongoing tissue damage and immune signaling. As MMP-9 breaks down the structural scaffolding of blood vessels and mucosal linings, it exposes the underlying cells to further immune activation and microbial intrusion, continuing the cycle.
The end result of these overlapping pathways - interferon-driven enzyme activation, uncoupled nitric oxide production, mitochondrial stress due to micronutrient depletion, and enzymatic breakdown by MMPs - is a gradual but relentless erosion of the glycocalyx. Once this protective layer is compromised, not only does it lose its physical barrier function, but it also becomes less able to buffer mechanical forces, regulate immune signals, and maintain redox balance at the vessel surface. In this way, the glycocalyx becomes both target and amplifier of the chronic inflammatory state, linking microbial signals, metabolic strain, and immune dysfunction into another self-perpetuating loop. Ginger, berberine and doxycycline are all inhibitors of MMP-9.
Interventions
Whenever our interventions or immune system responses are successful in killing microorganisms, their death can cause “dumping” and circulation of these toxins which contribute to a well-known “die-off effect” occurring. This die-off effect is responsible for a number of highly debilitating symptoms, such as headaches, nausea, additional fatigue, dizziness, swollen glands, bloating / gas, constipation or diarrhoea, joint or muscle pain, tachycardia, chills, cold hands / feet, itchiness, rashes, sweating and/or fever which resembles the “disulfiram effect”. Read more here: https://www.thecandidadiet.com/candida-die-off-symptoms/
This cascade can cause an ongoing / recurring cycle of extreme unpleasantness, if these infections and their original “safe spaces” (biofilms) are not fully resolved and a protective microbiome restored.
We have been actively researching a combination of some innovative and existing strategies to help kill these microorganisms and minimise the die-off symptoms (see 2.3.1 Herxheimer / die-off / acetaldehyde support). Some additional challenges relating to biofilms, which provide further protection against our immune activities are also targeted.
In addition to the metabolic supplement schedule included in this protocol, a more rapid clearance of any (somewhat) accessible microorganisms may be achieved by direct or topical interventions for these infected tissues. Commercial preparations are available with various levels of efficacy.
However, the quality of your data will determine the quality of your results. Having known targets allows for precision interventions to be used, whereas having unknown targets leaves you no choice other than "throwing darts in a dark room, hoping one or more of them lands". With a competent immune system, targeting the biofilms allows the immune system to see the pathogens and throw precision "darts".
Binders
Area of effect: localised and systemic interventions exist.
Limitations: somewhat selective interventions - matching products with toxins is important.
Risk profile: "Final binders" are usually non-toxic, some binders can also bind to nutrients, such as minerals, causing deficiencies over a short time.
Silicol Gel, Enterosgel: Both of these readily-available products are non-absorbing silica-based gels that act as “sponges” for endotoxins / LPS / acetaldehyde and salts of heavy metals, backed by clinical trials. These are consumed around mealtimes or interventions that induce die-off, to mitigate the Herxheimer effect symptoms.
Zeolite: Zeolite is a natural volcanic mineral with a high affinity for binding heavy metals, environmental toxins, and radioactive isotopes. It acts as a molecular sieve, trapping toxins within its cage-like structure. Zeolite is non-toxic and passes through the body without being absorbed, making it a popular detox aid. It is often used in detox protocols to support the elimination of lead, mercury, and other harmful substances.
Bentonite Clay: Bentonite is a type of absorbent clay known for its ability to bind toxins, chemicals, and heavy metals. When hydrated, it swells and creates an electrical charge that attracts toxins like a magnet. It is often consumed mixed with water and is widely used for digestive issues, detoxification, and skin health. It can be especially useful after exposure to environmental toxins or as part of a regular detox regimen.
Diosmectite (Smecta): Diosmectite is a natural clay-based binder with potent adsorption capabilities, specifically targeting bacterial toxins, viruses, and harmful substances in the gut. It forms a protective layer over the gut lining, reducing inflammation and aiding in the healing of gut mucosa. Diosmectite is commonly used for gastrointestinal issues like diarrhea and leaky gut and can be helpful in reducing symptoms of food poisoning and infections.
Activated Charcoal: Activated charcoal is one of the most popular and widely available binders. It has a porous surface that traps toxins, chemicals, and gases, preventing their absorption into the bloodstream. Often used for acute poisoning or in situations involving gastrointestinal distress, it can also be part of regular detox protocols. It is taken in capsules or powder form and is effective in reducing bloating, gas, and Herxheimer reactions during detoxification.
Fulvic Acid: Fulvic acid is a natural organic compound found in soil and water sources. It has strong binding properties and can help chelate heavy metals and toxins, making them more water-soluble and easier to eliminate through the kidneys. Fulvic acid is also known for its ability to enhance nutrient absorption and support cellular detoxification. It is often consumed in liquid form as a supplement for detox and overall health.
Humic Acid: Humic acid is a large molecule that works alongside fulvic acid to bind heavy metals, glyphosate, mycotoxins, and other environmental toxins. Its complex structure allows it to act as a natural chelator, pulling toxins from the body and supporting liver and kidney detoxification. Humic acid is commonly used to help restore gut health and improve immune function.
Spirulina: Spirulina is a blue-green algae rich in nutrients and known for its detoxifying properties. It is particularly effective at binding to heavy metals such as mercury, lead, and arsenic, promoting their elimination from the body. Spirulina is often used as part of heavy metal detox protocols and can be consumed in powder or tablet form.
Chlorella: Chlorella, another algae, is renowned for its detoxifying capabilities, especially in binding heavy metals, pesticides, and other toxins. It contains a unique outer cell wall that traps and removes these substances from the body. Like spirulina, chlorella is used in detox protocols and is available in various forms, including tablets and powders.
Pectin: Citrus pectin, especially in modified form, is a powerful binder that helps remove heavy metals and environmental toxins. It works by binding to these toxins in the bloodstream and digestive tract, preventing their reabsorption and facilitating their excretion through urine. Modified citrus pectin is often included in protocols for reducing toxic burden, particularly for lead and mercury.
Chitosan: Derived from the shells of crustaceans, chitosan is a natural polymer that acts as a binder for fat-soluble toxins, heavy metals, and excess lipids. It has therapeutic effects against LPS. It is often used to support weight loss and detoxification by reducing the absorption of fats and toxins from the digestive system. Chitosan supplements are available in capsule form and can be helpful in detox protocols.
Cilantro (Coriander): Cilantro is a natural herb known for its ability to mobilize heavy metals, particularly mercury, from tissues. While it may not be as potent as synthetic chelators, cilantro is often used in combination with other binders like chlorella to promote the safe excretion of heavy metals. It is a common addition to natural detox protocols and is consumed as fresh leaves, tinctures, or supplements.
A number of these binders are already included in the protocol at different stages.
Bacteriophages
Area of effect: localised, replicating and systemic (nebuliser, IV).
Limitations: highly selective intervention - matching products with species and strain are important.
Risk profile: Non-toxic, can create die-off symptoms.
A bacteriophage is a virus which doesn't infect human cells, however it does infect and kill bacteria with high specificity,
unlike antibiotics. They've been studied for over a hundred years and
Russia is well-established as the world-leader in this area.. which makes things a little
tricky in 2024.
Bacteriophages have been studied against gut microbiome dysbiosis in long COVID, with positive results.
https://www.mdpi.com/1999-4915/14/12/2614
A little-known fact about bacteriophages is that they can be found in seawater in concentrations of up to 107 mL−1,
however this does not automatically mean that random doses of seawater
will contain the relevant bacteriophages that eg. match your collections
of pathogenic species.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7150976/
If you have data from a microbiome report that indicates particular species of pathogenic bacteria,
you may be able to use a bacteriophage product in that tissue to help
eliminate them - very, very selectively.
However, on the basis of various species
regularly appearing in different tissues, bacteriophage products are
also available which target a range of common pathogenic species. It's
possible you may need more than one product to target all of the species
reported in your data.
A product selection table and various product instructions translated from Russian to English are provided in 5 Bacteriophage lookup.
For
GI related targets, oral + rectal administration is recommended by
product manufacturers, presumably to avoid being degraded by stomach
acid.
The same W302 nebuliser mentioned in the DIY antiseptic recipe section is also appropriate for bacteriophage delivery to lungs and circulating targets.
Luer slip syringes can be used for other tissues / orifices.
NB.
Just like when using any other any other well-targeted anti-microbial,
die-off is expected. The more potent the anti-microbial, the larger the
wave of toxins you need to metabolise and/or excrete. Some support for
this can be found in 2.3.1 Herxheimer / die-off / acetaldehyde support.
DIY antiseptic recipe: mucosal clean and flush, rinse, topical spray
Area of effect: localised, with some systemic absorption / effects in some cases, eg. black seed oil.
Limitations: broad spectrum, can harm good and bad species. Requires follow-up probiotics.
Risk profile: Negligible toxicity, can create significant initial inflammation and die-off symptoms.
Popular antifungal soaps, shampoos and creams containing zinc pyrithione can be effective at inhibiting fungal overgrowth. However, these products are now banned in Europe due to concerns around causing DNA damage - warning: avoid.
Part of a successful "untargeted" intervention for these tissues may also include first administering a solution to break up any protective biofilms, leaving this solution to incubate for 20–30 minutes before (where possible / appropriate) wiping the area clean and then administering a second solution to selectively inhibit these foreign cells. These two solutions can also be applied simultaneously. The process may be repeated daily for 1–2 weeks, or as necessary.
Getting started:
Ongoing testing and literature review has suggested that a simple solution of NAC and hypertonic sodium bicarbonate water solution can reliably break up many biofilms and lyase cells. Breaking biofilms exposes any remaining microbes to immune surveillance and any other interventions you may explore. Using this recipe in a Neilmed Sinugator, douche or other appropriate tool can be a gentler way to start clearing biofilms and remodelling microbiomes, such as the nasopharynx and sex organs.
Further research has also suggested that a solution containing diluted tea tree oil, clove oil and other oils, when applied with or immediately following NAC yields a tolerable, yet significant inhibitory effect on bacteria, yeasts, moulds and fungi which may rival or exceed existing pharmacological interventions and is appropriate for a range of applications.
Commercial preparations made from tea tree oil and clove oil, are also readily available as shampoos, vaginal douches, topical sprays, mouthwashes, creams and suppositories.
Available from your local chemist, Neilmed make sinus washing products – such as “Sinugator” and “Sinus Rinse”, which can be highly effective at pre-rinsing these difficult-to-reach mucosal tissues, 20 minutes prior to application of any antiseptic products.
2g boric acid and 5–10 droops of Lugol's iodine can also be added to the Neilmed solution, for additional potency. A temporary smell of iodine and some burning / stinging would also be expected where infected tissues exist.
Note: Due to the die-off effect when killing fungi, using this antiseptic recipe while not using the other supplements from Stage 1 may be unnecessarily unpleasant and exacerbate symptoms.
| Part 1: Mix 500mg of NAC powder (preferably not from a capsule, as these usually have fillers, although these could also be filtered / strained after stirring), 500mg of sodium bicarbonate (baking soda), 1g of xylitol and >5 ml of water. |
| Part 2: Separately, mix essential oils – 20 drops of tea tree oil, 80 drops of black seed oil, 6 drops of oregano oil, 6 drops of clove oil, 1 capsule of Biofilm Phase 2 Advanced (BP2A). (You can add more black seed oil if you find this too strong and want to dilute the more potent / irritating oils further.) |
| Mix both parts together to form your final solution – allow a 2 week shelf life. Store in an empty glass bottle with a dropper for convenient dosing. Shake well before use. |
To test this as a nasal antiseptic: while laying on your back, with your head tilted back and breathing through your mouth, drip about 6 drops of the solution into each nostril.
Let the solution run into the nasopharynx and incubate for a minute or so, while you suffer through some shockingly unpleasant burning for a few minutes (the first time), assuming you have infected tissue. (See the experiences reported in the Discord server for more information.)
Healthy tissues won’t be irritated at this concentration, so if it "burns" – repeat this process every 1-3 days until irritation / inflammation is not observed. It will get progressively much easier.
Rotating your head slowly to each side and very gently “equalising” (like pinching your nose, gently exhaling through the nose against the close nostrils and "popping your ears", like on an aeroplane) with fluid in the nasopharynx may allow the solution to access the Eustachian tubes. (Performing the same in reverse and inhaling against closed nostril can evacuate the tubes, also.) After some time, blow / purge your nose, leaving some residue behind. A follow-up nasal probiotic may be very helpful after eg. 5-7 days of this, assuming there is no significant inflammation in response to the antiseptic.
To test this as a topical antiseptic: simply clean the area and then spray / apply the solution. A cotton tip could assist application to the ear canal or rectum (don’t use this in enemas).
To test this as a dental pre-rinse: apply a few drops to your tongue, teeth and gums, or more to gargle and spit. Wait a few minutes, then brush / floss as usual. Note: unpleasant flavour. Note: as an antiseptic, small amounts reaching your throat isn’t likely to cause toxicity, whereas drinking it intentionally could be harmful.
For sensitive tissues
Recipe 2:
Combine a “squirt” of Johnson & Johnson Baby Shampoo (it contains a gentle detergent and EDTA as a biofilm breaker. NB. We are currently exploring organic alternatives) ,
plus;
1 x "Neilmed hypertonic sodium sachet" (or a teaspoon of sodium bicarbonate / baking soda), for osmolality,
in 240mL of clean water.
This recipe makes a gentle, yet potent, biofilm breaking intervention that can be used in a Neilmed Sinugator/Sinus Rinse tool, vaginal douche, Waterpik, etc.
Alternatively, you can also make another DIY rinse recipe:
Recipe 3:
Per 500mL of boiled / cooled water -
Mix 5g of sodium bicarbonate (baking soda) with 5g NAC. This allows an acid:base reaction (and gas release) to occur, which helps create a pH balanced solution.
This can then be combined with ¼ teaspoon of boric acid (making a 1½–2% solution) and 10 drops of the 5% Lugol’s iodine or 25 drops of 2% Lugol’s iodine.
To administer recipe 2 or 3:
- Eyebath: Use 30mL of the solution to bathe each eyeball, also cleaning the eyelids, lashes.
- Urethra: Administer 5–30mL of the solution via a large (needleless, Luer slip) syringe to the opening.
- Vagina: Administer 50-120mL, using a suitable douche tool or syringe and keep your hips and legs elevated for 30 mins.
- Lungs: (Use "Recipe 3" only) Administer 1-3mL via a drop-feed ultrasonic nebuliser, such as a "W302", found in most online marketplaces
- Sinuses, Eustachian tubes: This recipe can also be added to the Neilmed Sinugator reservoir.
The colostrum from Stage 2 can also be successfully used in mucosal tissues to neutralise unwanted species, antigens, etc.
Rotating between the “potent” recipe and the “gentle” recipes for 1–2 days is recommended if intense inflammation for more than 30 minutes is experienced. Continue with the nasal probiotics from the next section once an inflammatory response can’t be provoked by the normal antiseptic recipe.
Other simple and effective tools:
60-70% ethanol, as eg. rubbing alcohol or hand sanitiser, is also a well-known broad-spectrum, highly penetrative, highly indiscriminate intervention that can be used effectively in small amounts against viruses, bacteria, fungi and parasites on externally accessible tissues. In one RCT, where healthcare workers colonised with nasal S. aureus were swabbed intranasally three times daily with 70% ethanol plus natural oil emollients and benzalkonium chloride, they reported a median 99% reduction in CFU and no adverse effects during the study. From personal experience, it will feel temporarily "warm" and briefly quite unpleasant on broken or inflamed tissue and can be potentially damaging, if overused. Caution is also needed with ocular tissue - alcohol will cause damage.
Regardless of the recipe used, strong die-off effects can be expected the first time and should only be implemented after sufficient metabolic and detox support supplements are added in Stage 1 of the protocol / pre-protocol support.
Links to ingredients and tools mentioned can be found in the "5 Ordering products" section.
Biofilm breakers
Area of effect: some are localised, others are systemic.
Limitations: does not directly kill microorganisms - requires immune activity, probiotic species and/or other interventions to eliminate the species inside. Different biofilm compositions respond to different biofilm breakers - more than one may be required in chronic diseases with more than one pathogen indicated.
Risk profile: usually broad effects on biofilms for both good and bad species. Can trigger elevated immune activity and redistribution of microorganisms. If misused or overused, can damage microbiome diversity and abundance profiles.
Biofilm Phase 2 Advanced (BP2A): a localised bismuth-thiol biofilm breaker. Doesn't absorb. Included in Stage 2 and DIY antiseptic recipe.
NAC: a systemic biofilm breaker, particularly at higher doses.
Glutathione: a systemic biofilm breaker, particularly at higher doses.
Fulvic acid / humic acid: a systemic biofilm breaker, even at lower doses.
R-Alpha lipoic acid: a systemic biofilm breaker and metal chelator, particularly at higher doses.
Soap / detergent: a localised biofilm breaker, when used externally.
Ethylene Diamine Tetraacetic Acid (EDTA): a localised biofilm breaker and metal chelator, usually supplied bound to an electrolyte or mineral. Doesn't absorb well, orally - 5%. Can be used IV for circulating biofilms.
Dimercaptosuccinic acid (DMSA): a systemic biofilm breaker and metal chelator. Doesn't absorb well, orally - 25-30%. Can be used IV for circulating biofilms.
Dimercaptopropane-1-sulfonic acid (DMPS): a systemic biofilm breaker and metal chelator. Can be used orally or IV.
Microdacyn / hypochlorous acid: a localised biofilm breaker. Some absorption.
Ethyl acetate: a systemic biofilm breaker, even at very low doses. Found in robusta coffee and various acetone-free nail polish remover products.
Silver: a systemic biofilm breaker, even at very low doses.
Compounds found in foods: Allicin (Garlic), Curcumin (Turmeric), Epigallocatechin gallate (Green tea), Quercetin (Onions, Apples), Resveratrol (Grapes, Red wine), Eugenol (Cloves), Cinnamonaldehyde (Cinnamon), Sulforaphane (Broccoli, Brussels sprouts), Apigenin (Parsley, Celery, Chamomile), Berberine (Goldenseal, Barberry), Thymol (Thyme, Oregano), Carvacrol (Oregano, Marjoram), Fisetin (Strawberries, Apples), Linalool (Coriander, Lavender), Gallic acid (Blueberries, Pomegranates), Cinnamic acid (Honey, Cinnamon), Citric acid (Citrus fruits), Naringenin (Citrus fruits), Rosmarinic acid (Rosemary, Basil), Catechin (Cocoa, Dark chocolate), Ellagic acid (Pomegranates, Raspberries), Diallyl disulfide (Garlic), Capsaicin (Chili peppers), Piperine (Black pepper), Hydroxytyrosol (Olive oil), Xylitol (Berries, Plums), Isothiocyanates (Kale, Mustard greens), Ferulic acid (Rice bran, Oats), Kaempferol (Spinach, Kale), Pterostilbene (Blueberries), Saponins (Beans, Legumes), Chlorogenic acid (Coffee, Potatoes), Luteolin (Peppers, Carrots)
Probiotics: many of the probiotic species included in the protocol have potent functions as biofilm degraders and inhibitors. (see "Protective probiotics").
A number of these biofilm breakers are already included in the protocol. Overall, biofilm breakers should be considered an integral part of any microbiome dysbiosis or infection intervention and food sources should be included in any dietary strategy.
There are some additional strategies being tested which may feature in future updates, for example:
Upper GI biofilm flush, bind and purge recipe (advanced):
This a 3 step process, with similarities to a colonoscopy prep or gallbladder flush procedure. This
is not intended to ever be used a daily routine, as this intervention is
significantly broad spectrum and is highly destructive to the entire microbiome in the
upper GI. It would be used in limited circumstances only.
Step 1
contains a potent mix of biofilm breakers and anti-microbials, plus
some starch and warm water. Some of these items are not normally
consumed, however they are successfully used for pre-faecal microbiome
transplant (FMT) procedures. The mixture of anti-biofilm and
anti-microbial interventions is
adapted from Dr Thomas Borody’s excellent pre-FMT biofilm flush protocol and uses 2g biocompatible detergent (baby shampoo), 4mL of 1% iodine and 50mL Microdacyn).
The biofilm
flush recipe adaptation includes some additional items - an extra
biofilm degrader (ethyl acetate, from 2 shots of ground robusta coffee), 1 spoonful of diatomaceous
earth as a bulking agent and binder, along with an optional (opened) capsule of cascara to irritate / stimulate the bowels and increase GI motility. All of
these items are added to an empty glass and half a glass of hot water is
stirred in.
3 large spoonfuls of sifted potato starch (to prevent clumping) slowly stirred in to make a
rubbery mass that helps dislodge and drag / sweep along the broken biofilms. Fill the remaining part of the glass with cool water.
(This delightful concoction needs to be consumed quickly, or it'll polymerise in the glass.)
Step 2,
20 mins later - binders to help absorb toxins instead of allowing them
to circulate, which was a concern with the original pre-FMT protocol.
This next step includes a generous mix of binders, being 1/2 tablespoon of charcoal, 1/2 tablespoon of zeolite, 1/2 tablespoon of pectin and
1/2 tablespoon ofslippery elm powder, mixed into a glass of water.
Step 3,
20 mins later - this functions just like a colonoscopy prep or
gallbladder flush recipe. A large amount of electrolytes (Epsom salts / magnesium
sulphate) and lots of water are consumed. The large volume of magnesium
sulphate draws water into the bowel and purges the contents in a predictably dramatic fashion.
Add 1 teaspoon of Epsom salts (magnesium sulphate) to a glass of water. Stir until dissolved and consume.
Repeat this step 2 more times - 60 and 120 minutes later.
Overall, this allows the original biofilm breaking concoction from Step 1 around 40 minutes of travel throughout the GI tract, before being chased and diluted by the flush, reducing the impact of the biofilm breakers on the remaining length of bowel. It can potentially be adapted around the timing of peak gas output during a SIBO breath test, or reactivity timing to food.
Expect some unpleasant die-off symptoms / herxheimer-style reactions,
diarrhoea, nausea shortly afterwards. Exclusive bathroom access would be advisable for the next 12-18 hours.
Step 4, 12-24 hours later - consume S.boulardii, Bifidobacteria and Lactobacillus probiotics + prebiotics, related foods.
This flush could be performed
1-3 times, if
severe upper GI overgrowth exists, as evidenced by reactions to food in
under 1 hour. Excessive use of this recipe would NOT be recommended.
Protective probiotics
Area of effect: localised, however can translocate to other tissues.
Limitations: probiotics may not provide a comprehensive solution in isolation.
Risk profile: Non-toxic, can create significant die-off symptoms. The literature suggests some species can be opportunistic pathogens in highly immunocompromised people.
Following on from any efforts in clearing unwanted biofilms and microbial species overgrowth in the eyes, sinuses, nasopharynx, mouth, throat, oesophagus, lungs, GI tract, vagina, urethra and other mucosal tissues, further restorative efforts are usually needed in repopulating these tissues with helpful species to promote and maintain a healthy microbiome. (Links to these products can be found in the “5 Ordering products” section.)
These helpful species assist in inhibiting unwanted species, degrading biofilms and preventing opportunistic growth. They can also provide helpful functions, such as metabolism of oxalates, acetaldehyde, histamine, plus production of short chain fatty acids and other compounds beneficial to humans. Please note inclusion of these probiotics are based on an observed pattern of
diversity loss and are included for specific functions, to generally
promote a healthier balance in the microbiome, when combined with remineralisation and dietary changes.
They are not intended to replace MARCoNS, vaginal swabs, “GI-MAP” or Biomesight gut microbiome tests.
Many of these species were traditionally found in the Bacillus, Lactobacillus and Bifidobacterium genus, although recent taxonomy changes have relabeled / reclassified some of them, providing some minor confusion when researching species.
Bacillus subtilis:
Key Mechanism: Produces enzymes and antimicrobial compounds that degrade biofilms.
Notable Features: Spore-forming bacterium, resilient and able to survive harsh conditions, which allows it to act more potently against biofilms.
Effective Against: Both Gram-positive and Gram-negative bacteria.
Additional Benefits: Supports overall gut health and resilience against environmental stressors.
Lactobacillus fermentum ME-3:
Key Mechanism: Produces glutathione (antioxidant), disrupts pathogenic biofilms, reduces oxidative stress.
Notable Features: Dual-action as a biofilm breaker and antioxidant producer. Glutathione production sets it apart from many other probiotics, as it supports cellular detoxification.
Effective Against: Harmful gut pathogens and biofilm-forming bacteria, also including H. pylori..
Additional Benefits: Supports immune function, reduces inflammation, and has cardioprotective effects.
Lactobacillus reuteri:
Key Mechanism: Produces reuterin, a powerful antimicrobial compound that breaks down biofilms.
Notable Features: Strong antimicrobial activity, especially effective in the oral cavity and gut.
Effective Against: Pathogens like E. coli, H. pylori, and oral biofilm formers.
Additional Benefits: Promotes oral and gut health, reduces inflammation.
Lactobacillus rhamnosus:
Key Mechanism: Produces bacteriocins and SCFAs, which inhibit biofilm formation.
Notable Features: Excellent at inhibiting gut biofilms and maintaining gut balance.
Effective Against: E. coli, Pseudomonas aeruginosa, and other biofilm-producing pathogens.
Additional Benefits: Supports immune system, often used in combating gastrointestinal infections.
Lactobacillus plantarum:
Key Mechanism: Produces hydrogen peroxide and antimicrobial peptides that break down biofilms.
Notable Features: Broad-spectrum biofilm inhibition, active in the gut and oral cavity.
Effective Against: Gut and oral pathogens, including Candida and Staphylococcus aureus.
Additional Benefits: Improves digestive health, supports immune system function.
Lactobacillus casei:
Key Mechanism: Disrupts biofilms through production of bacteriocins and lactic acid.
Notable Features: Particularly effective against Helicobacter pylori biofilms in the gut.
Effective Against: H. pylori and other gut pathogens.
Additional Benefits: Supports digestive health, beneficial in addressing stomach ulcers.
Bifidobacterium bifidum:
Key Mechanism: Produces SCFAs like acetate, which create an acidic environment that disrupts biofilms.
Notable Features: Prevents biofilm formation by pathogenic bacteria in the gut.
Effective Against: Pathogens like Clostridium difficile and other harmful gut bacteria.
Additional Benefits: Supports overall gut health, improves digestion and immune system.
Bifidobacterium longum:
Key Mechanism: Like B. bifidum, B. longum produces SCFAs that lower the pH in the gut, which can inhibit biofilm formation. It also promotes the production of antimicrobial peptides and enzymes that disrupt pathogenic biofilms.
Notable Features: One of the most common Bifidobacterium species in the human gut, B. longum is well-adapted to the gut environment and plays a crucial role in maintaining microbial balance. It is especially good at outcompeting pathogenic bacteria.
Effective Against: Effective against a range of harmful bacteria, reducing biofilm formation in the gut.
Additional Benefits: Enhances immune function and promotes gut health, further protecting against biofilm-related infections.
Bifidobacterium lactis:
Key Mechanism: B. lactis can modulate immune responses, leading to the production of compounds that degrade biofilms or prevent their formation. It also produces lactic acid and acetic acid, which inhibit the growth of biofilm-forming pathogens.
Notable Features: Known for its resilience in the gastrointestinal
tract, B. lactis is widely used in probiotic supplements due to its
strong ability to survive stomach acid and bile. It's particularly
effective at adhering to the gut lining, enhancing its biofilm
prevention capabilities.
Effective Against: Has shown effectiveness in reducing biofilm formation by Escherichia coli and other gut pathogens.
Additional Benefits: Improves gut barrier function and promotes overall digestive health.
Bifidobacterium breve:
Key Mechanism: B. breve produces metabolites that interfere with pathogen adhesion and biofilm formation. It can inhibit the colonization of harmful bacteria by promoting a balanced gut microbiome and maintaining a lower gut pH through lactic acid and acetate production.
Notable Features: B. breve is one of the earliest colonizers of the human gut in infancy, making it especially important in the development of a healthy microbiome. It plays a significant role in maintaining gut integrity and has strong antimicrobial activity against pathogens.
Effective Against: Effective against Clostridium difficile and other gut pathogens that form biofilms.
Additional Benefits: Helps alleviate symptoms of gut dysbiosis, supports digestion, and reduces inflammation in the gut.
Bifidobacterium adolescentis:
Key Mechanism: Produces SCFAs and antimicrobial peptides that help prevent pathogenic biofilm formation. B. adolescentis can also enhance gut mucosal immunity, providing an additional layer of protection against biofilm-forming bacteria.
Notable Features: B. adolescentis is prevalent in the adult gut and plays a crucial role in breaking down complex carbohydrates, contributing to overall digestive health. Its ability to stimulate immune cells makes it particularly effective in preventing gut infections.
Effective Against: Reduces biofilm formation by pathogens in the gut, such as Salmonella and Escherichia coli.
Additional Benefits: Supports the immune system, promotes gut health, and reduces inflammation.
Saccharomyces boulardii:
Key Mechanism: Inhibits biofilms and outcompetes pathogens in the gut.
Notable Features: Effective against Candida and Clostridium difficile biofilms. Not susceptible to antibiotic influence.
Effective Against: Fungal pathogens and gut pathogens, particularly in cases of infection or dysbiosis.
Additional Benefits: Supports gut health, reduces diarrhea and inflammation, commonly used in traveler's diarrhea prevention.
Also potentially helpful is Oxalobacter formigenes, as an oxalate degrading species. When present in the small intestine, it also signals the host to secrete oxalates into the gut, instead excreting them via the kidneys. However, acidemia will override this.
Bifidobacterium are largely pH sensitive. You will have difficulties in restoring diversity and abundance while lactic acid metabolism is overused and zinc is low (hypoxia, impaired glycolysis, low minerals, anxiety disorders). Your OAT results should help indicate if lactic acid (+ oxalates) markers are elevated or the lactic acid : pyruvic acid ratio is elevated.
Studies and dosing information for these microorganisms in different mucosal tissues can be found on the Discord online discussion group and/or the literature. This protocol currently includes a number of key probiotics relating to these studies and their described functions / benefits:
- Life Extension Florassist: (Oral microbiome)
Probiotics - BLIS M18 S. salivarius M18, L. plantarum L-137 - DrFormulas Nexabiotic for Women: (Acid resistant capsule)
PaCran®SP (Cranberry fruit 50:1 extract), D-Mannose,
Probiotics - Saccharomyces boulardii, Lactobacillus helveticus, Lactobacillus delbrueckii LE, Enterococcus faecium, Bifidobacterium bifidum, Bifidobacterium longum, Bacillus coagulans, Lactobacillus rhamnosus LB3, Lactobacillus plantarum LM, Lactobacillus acidophilus, Lactobacillus rhamnosus, Bifidobacterium animalis lactis (formerly named Bifidobacterium infantis), Lactobacillus fermentum, Lactobacillus gasseri, DE111® (Bacillus subtilis), Lactococcus lactis, Lactobacillus casei, Lactobacillus salivarius, Lactobacillus brevis, Lactobacillus reuteri, Streptococcus thermophilus, Bifidobacterium lactis, Low moisture rice dextrin, delayed release capsule (hydroxypropyl methylcellulose, pectin, and water), silica. Allergen warning: Contains milk. - DrOhhira RegActiv Essential ME-3: (Survives stomach acid.)
Probiotics - Lactobacillus fermentum ME-3®, maltodextrin, magnesium salts of fatty acids (anti-caking agent). Vegetable capsule (hydroxypropylmethylcellulose). - CFUful 300 Billion CFU: (Acid resistant capsule)
Probiotics - Bifidobacterium longum BB536, Bifidobacterium longum HRVD90b, Bifidobacterium breve BR3, Bifidobacterium breve HRVD521, Lactiplantibacillus plantarum LP1, Lacticaseibacillus rhamnosus LR6, Lacticaseibacillus rhamnosus HRVD113, Lacticaseibacillus rhamnosus GG, Bifidobacterium infantis M63, Bifidobacterium lactis BS5, Bifidobacterium lactis HRVD524, Bifidobacterium lactis SD150, Lactobacillus crispatus LCR01, Lacticaseibacillus casei HRVD300, Limosilactobacillus fermentum LF8, Lactobacillus reuteri RD830, Lactobacillus acidophilus, Ligilactobacillus salivarius LS1, Bifidobacterium longum CECT7347, Lactobacillus casei CECT9104, Bifidobacterium bifidum, Lactiplantibacillus plantarum LPLDL, Bifidobacterium lactis MB2409.
Prebiotics - Fructooligosaccharides (FOS), Organic Barley Grass Powder, Organic Wheat Grass Powder, Organic Alfalfa Grass Powder, Organic Oat Grass Powder, Organic Beet Juice Powder, Organic Spinach Powder, Organic Suma Root Powder, Organic Licorice Root Powder, Organic Dandelion Root Powder, Organic Astragalus Root Powder, Organic Milk Thistle Seed Extract, Organic Ginkgo Leaf Extract, Organic Bilberry Extract, Organic Ginger Root Powder
- General Biotics Equilibrium Boost MegaDose Probiotic: (2 x acid resistant capsules per container.)
Probiotics - 115 strains, which have their own page, here - https://www.generalbiotics.com/equilibrium/strains/ - Ochek: (Only needed if indicated as missing in gut microbiome data. Promoted by dietary oxalates.)
Probiotics - O. formigenes, L. acidophilus, L. rhamnosus, B. lactis
Prebiotics - FOS - Pendulum Metabolic Daily: (Butyrate producers. Akkermansia promoted by pomegranate.)
Probiotics - Clostridium butyricum WB-STR-0006, Clostridium beijerinckii WB-STR-0005, Bifidobacterium infantis, Anaerobutyricum halii WB-STR-0008, Akkermansia muciniphila WB-STR-0001 - (Various sources, Kimchi) - L. sakei: (Anti-microbial. Also used in food production to prevent spoilage, etc.)
Probiotic - Lactobacillus Sakei
For example:
Nostrils: cotton tip / fingertip and apply inside the nostrils. Eustachian tubes: place drops of liquid into the nose and use the “equalisation” technique.
Mouth / throat / oesophagus / upper GI: gargle and swallow.
Lungs: nebuliser, 1-2 mL.
Vagina: add to a 5ml vaginal douche and elevate hips/legs for 15 minutes, while laying down, or place recently moistened, unopened capsule deep into fornix and allow it to dissolve.
Lower GI tract: use a probiotic rectal syringe (no tip) with <50mL of water, then “down dog” yoga pose for 15 mins to bypass stomach acid. Achieves a similar colonisation rate to FMT.
Eyes: place drops of liquid into the corners of the eyes and / or under the eyelids.
Prebiotics
Area of effect: localised, with systemic benefits.
Limitations: can be highly selective for promoting helpful species, if well-selected.
Risk profile: Non-toxic, can create die-off symptoms. Can promote unwanted species, if poorly selected.
You cannot solve dysbiosis by probiotics alone. Strategically feeding your microbiome and correcting symbiotic host metabolism, via remineralisation, etc. is the best way to make any lasting transformations. If you've ever made yoghurt, you'll have a good understanding of just how rapidly 2L of milk can turn into a (probiotic) fermentation product. 8 - 12 hours can turn eg. 2L of milk into 2L of yoghurt with just a spoonful of starter culture / microorganisms.
Your GI tract is no different, in this respect. Your choice of foods (substrates) allows you to achieve some selectivity in the species being fed and promoted. What you eat matters.
Inulin + fructooligosaccharides (FOS) are types of soluble fiber found in a variety of plants. Some common food sources include:
Chicory root (one of the richest sources), Jerusalem artichokes, Garlic, Onions, Leeks, Asparagus, Bananas, Dandelion greens, Wheat
Galacto-oligosaccharides (GOS)
is often added to foods as a prebiotic fiber, but it is also found in
trace amounts naturally in certain foods. Some food sources include:
Human breast milk (high content of GOS), Cow's milk, Lentils, Chickpeas, Green peas, Soybeans
Resistant starch is a type of starch that resists digestion and feeds beneficial gut bacteria. Common sources include:
Green
(unripe) bananas, Cooked and cooled potatoes (cooking and cooling
increases resistant starch), Cooked and cooled rice, Oats, Legumes
(lentils, chickpeas, beans), Barley, Corn
Polyphenols are compounds found in many fruits, vegetables, and beverages. Some common polyphenol-rich foods include:
Berries
(blueberries, strawberries, raspberries), Pomegranates, Cranberries,
Dark chocolate (high in cocoa content), Green tea (especially rich in
EGCG), Red wine, Olive oil, Nuts (walnuts, almonds), Herbs and spices
(turmeric, cloves, oregano)
These should be considered as high priority food items to introduce when planning your diet. However, they'd be expected to create some die-off reactions, gas and digestive discomfort at first. (see "2.2.1 Diet" for information on food items which also includes prebiotics)
Herbal Anti-microbials
Area of effect: localised and systemic
Limitations: may have broader effects on metabolism.
Risk profile: over-the-counter, generally regarded as safe. Can create significant initial die-off symptoms. Can alter drug metabolism.
There are a number of very effective and highly selective, plant-based anti-microbial products / foods.
Some of these interventions can simultaneously promote good species at the same time as inhibiting unwanted species. These would ideally be introduced in Stage 2 and will relate to your microbiome report data.
Notes:
Vanillin is often used at 2g, 2x per day and has been shown to kill sulphur-reducing and other unwanted species, however these species can be producing metabolites which have an antidepressant-like effect. Removing these species can create antidepressant-like 'rapid withdrawal' symptoms for up to 2 weeks.
Allicin has a particularly potent Minimum Inhibitory Concentration (MIC) for H. pylori, Candida spp., Porphyromonas gingivalis, Prevotella intermedia, Enterococcus faecalis, Clostridia spp. and Escherichia coli.
Resveratrol has broadly beneficial effects at 300-600mg, 3x per day, but can inhibit aldehyde dehydrogenase activity, especially in larger doses.
Short-chain fatty acids (SCFAs) such as butyrate can have highly positive effects on the microbiome and epithelium, however can create significant alterations which induce multi-day long die-off. Starting slowly is advisable.
Quercetin has many beneficial effects, but can inhibit aldehyde dehydrogenase activity, especially in larger doses.
Berberine has potent effects against Clostridia, but has similarly potent effects on enhancing fatty acid transport at CD36 and inhibiting mitochondrial complex 1. May not be well tolerated by some people, especially before Stage 2.
Here is a table of direct and indirect promoters and inhibitors, by genus / species (sorry, this table is too large for mobile and tablet screens):
A highly potent, combination herbal anti-microbial product is available called GI-Synergy. It features many of the interventions listed in the table above. It would be advisable to start slowly and work up to a full dose, in Stage 2.
(Prescription-based interventions and other options)
Area of effect: some are somewhat localised, however usually systemic.
Limitations: highly non-selective and broadly harmful to many species - good and bad. Antibiotic resistance can be created.
Risk profile: may harm mucosal tissues. May inhibit host metabolism. Can create potent die-off symptoms. Requires probiotics, prebiotics and dietary optimisation to prevent deleterious effects on microbiomes. Creates risk for fungal overgrowth, if not combined with anti-fungal interventions.
It’s expected that for “PSSD” symptoms that a UTI or sex organ infection may be present. With good data and a discussion with your doctor, specific antibiotics may be appropriate to treat an indicated infection, as these tissues are difficult targets, especially in males. Bacteriophages may also be an option for many cases.
Once you have collected quality data, you should be empowered to make better decisions around how to move forward. To assist this process, a database of pathogens and overgrowth vs interventions is being developed to help you decide what the best course of action is and will grow, over time. Most of these inhibitors are prescription antibiotics that require a discussion with your doctor, who can also advise you on the risks and benefits of pairing any antibiotic use with anti-fungal medications like itraconazole and fluconazole, to prevent the opportunistic overgrowth of fungal species during any significant microbiome remodelling. Careful attention will also be needed towards probiotics, prebiotics and diet.
Ideally, any antibiotics and anti-fungal interventions would not be started until Stage 2, or very late in Stage 1, if some urgency is required.
For further information on prescription antimicrobials, their mechanisms and effects on human metabolism, you can explore our Antimicrobial Library.
The table below will hide columns on smaller screens. You can use complete or partial words eg. "kleb" or "Klebsiella" for searching genus, species or inhibitors.

When a person is chronically ill and confined to their bed / house, the transfer of pathogenic microbes from their body to their surroundings becomes a significant concern. Pathogenic microbes can transfer easily from the body to the environment and back again, causing an ongoing challenge to an already compromised immune system.
One of the primary concerns is the transfer of pathogenic microbes to the bed, pillows, sheets, and mattress. These surfaces can harbour pathogens and continue a cycle of infection.
Bed linen – sheets, pillowcases, and blankets – should be changed frequently and washed in hot water, with a hygienic detergent to kill any pathogens present and arrest the cycle of reinfection.
Mattresses and pillows should also be rotated and disinfected regularly. A waterproof mattress protector can also help prevent the accumulation of moisture and bacteria. These will also need regular cleaning.
Another concern is the transfer of airborne pathogens through air conditioning systems. Air conditioning systems can spread pathogens throughout a room, increasing the risk of infection. It is important to clean / change the air filter frequently and consider using an air purifier to help remove pathogens from the air.
Wet areas are a common issue - bathrooms and kitchens, etc. Mould, fungi and other microorganisms can be found in water filtration systems, extractor fans, drains, towels, rugs and soft furnishings, tile grout, spaces / voids around baths, showers and sinks, before being transferred to other locations. Mould / fungi also produce mycotoxins in the form of gases, which can be silently poisoning household occupants - inhibiting energy metabolism and neurotransmitter homeostasis.
Nasopharyngeal inflammation and even intracranial pressure can sometimes be a "helpful" clue to investigate if there is a potential mould issue.
Carpets, window frames, walls, skirting boards, ceilings, books and bookcases, etc should also be inspected and maintained appropriately. Commercial air quality testing and mould remediation services are also available.
If not completely bed-bound and where the room doesn't have plants and/or pets (which can be excluded from the room for an hour), a relatively cheap ozone generator can be used to disinfect entire rooms, very effectively. [NB. This will cause a number of materials to off-gas aldehydes and other volatile organic compounds (VOCs). [YOU WILL NEED TO VENTILATE THE ROOM FOR A REASONABLE PERIOD OF TIME, AFTER SANITISING WITH OZONE.]
Sunlight is also helpful in inhibiting certain microorganisms.
Overall, it is essential to maintain good hygiene practices – regularly disinfecting surfaces and fabrics, to prevent ongoing reinfection and unnecessary delays in progress.
We also share our microbiomes with close contacts. This happens in both directions, which can create interesting challenges and yet another reinfection cycle, in some cases. A host with a competent microbiome and immune system should be resilient against new challenges, helping to prevent this.
Where possible, getting outside of the home environment regularly can boost microbiome diversity and improve the efficiency of microbiome remodelling, as can interaction with pets who spend time outdoors. There are many anecdotes of short-term remission events occurring, simply by taking a holiday away from home. Unfortunately, these normally revert within 1-2 months of returning to the original environment, or eg. staying in the same hotel room for more than 1-2 months.