Use at least one of the following two testing methods (hair mineral testing no longer supported for measuring most deficiencies due to unavoidable limitations in the methodology).
There are limitations to any testing methodology and potential ways for errors in sampling to occur. Some of these problems can be identified and avoided. Others can relate to eg. unpredictable sample transport delays.
To identify potential data errors, best practice is to triangulate and validate markers, deficiencies and issues from multiple data sources, eg. direct measurements of minerals and patterns in metabolites of enzymatic reactions which rely on these minerals.
White blood cells (WBC)
Currently, there are 3 competing laboratories which specialise in measuring the intracellular nutrient status inside WBCs - Cell Science Systems CMA (part of their CNA offering), SpectraCell Micronutrients and Vibrant America Micronutrients.
WBCs are used as a proxy to infer the nutrient status of other cell types, eg. brain, muscle, liver, etc. This data is very different to what is reported in serum (data sourced from outside the cells and any/all related mineral transporter function) or red blood cells, which lack mitochondria and therefore have very different metabolism. Vibrant America Micronutrients test does an excellent job of highlighting this issue in their report. It's frankly astonishing that serum testing is still considered the "gold standard" by public health systems, in light of these issues. However, this also highlights why chronic diseases have been difficult to research and solve.
Although all of these laboratories measure WBC nutrients, each of these tests has a different methodology and different array of included markers. Therefore, the advantages and disadvantages for each have been carefully considered. Primarily due to the expansive array of markers more closely matching our requirements, Cell Science Systems CMA is used by this protocol. However, there are limitations to accommodate. In a more perfect world, we would have a test that uses the SpectraCell or Vibrant America methodology, with the CMA scope of markers.
By checking OAT results before ordering the CMA test, you can help identify if you have the hypoxia / acidemia patterns and are likely to have issues:
1. If you see elevated lactic acid (22), relative to pyruvic acid (23), elevated oxalic acid (21), and/or low phosphorus (76), this pattern is suggestive of excessive anaerobic glycolysis / lactic acid metabolism, metabolic acidemia and renal phosphate dumping.
2. A relative drop from citric acid (29) to aconitic acid (28), with similarly low 2-oxoglutaric acid (27) may indicate severe deficiency of magnesium.
The Getting started section may be helpful in stabilsing the baseline metabolism enough to perform the CMA test without issues. Alternatively, you could use the Oligoscan test discussed below, without this limitation.
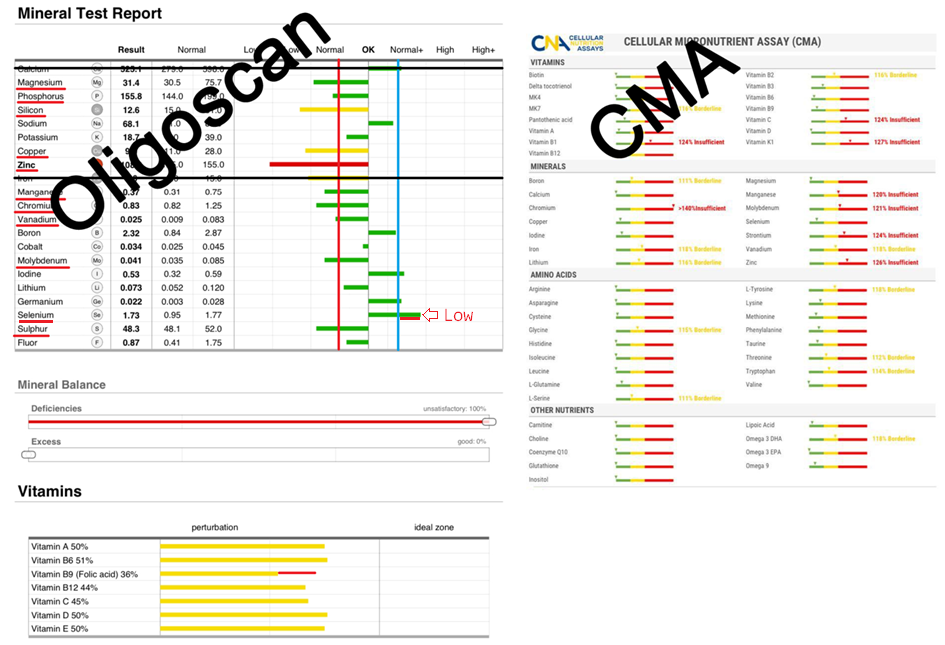
However, if you receive a CMA report which is verifiably affected by this issue, you may be able to partially salvage the results by reinterpreting the markers as follows:
1. Any marker not all the way to the left, yet still green is re-interpreted as yellow.
2. Any marker that is yellow is re-interpreted as red.
3. Any marker that is red is re-interpreted as severely deficient.
Advantages:
1. Directly actionable data from an accredited laboratory.
2. Significant array of markers included.
3. Data is considered a snapshot of "current status", without any lag.
4. Blood sample can be collected at home, using a mobile phlebotomist.
Limitations:
1. 8–12 hours fasting is required.
2. Does not include fluorine, sulphur, silicon, various toxic metals, and some of the electrolytes – phosphorus, sodium and potassium
3. Does not indicate excess nutrient data, although this hasn't been a concern.
4. Transport of the sample needs to be rapid, to accommodate eg. cytokine half-life and nutrient transporter behaviour in the cellular membrane, otherwise report sensitivity can be lost. For non-US citizens, an express FedEx courier service is supplied by the laboratory (with an additional cost), along with any import/export clearance paperwork needed for getting blood samples through border security.
5. Sensitivity in the reporting appears to be significantly impacted by hypoxia, phosphate, sulphur and other deficiencies.
6. Intracellular iron status does not capture systemic iron status data, as 75% of iron is circulating in RBC and serum. A separate test is required.
This comprehensive test is available internationally from a US laboratory. The test normally costs USD$239 - 264, plus express FedEx shipping (usually quoted / invoiced separately, shortly after purchase) and any phlebotomist costs.
Ordering: (International, via USA)
Low iodine may be used to infer high fluorine.
Phosphorus data from the Organic Acids Test (OAT) can infer phosphorus status, although there are some differences, being urine / excretory data.
The protocol uses daily targets for electrolytes, however you won’t have an understanding of the baselines for these markers.
Skin
Research suggests that an Oligoscan, So/Check or Zell-Check report can provide an approximation of your ACTUAL mineral status, using the skin of your hand as a data source. Note that “OligoLab” / “OligoHealth” / “Scantest” branded reports are currently not supported. This is normally an in-clinic test and a local practitioner will be required.Your blood type, age, height and weight affect the sample calibration used to generate this report, so this information will be requested when you visit a clinic. Any inaccuracies can dramatically alter your results.
NEW: An Oligoscan report analysis tool can be found here.
While not happy with the level of published evidence currently supporting this emerging methodology, our testing showed a clear pattern of deficiencies in ME/CFS, Long Covid and Post Vaccine Syndrome, with minor variability, which was not observed in controls.
Follow up Oligoscan reports have also matched supplements taken and previous results. The array of elemental markers collected is almost the same as the Doctors Data HTMA reports, however it also includes silicon and usually fluorine. Unfortunately, it does not show rubidium or strontium markers.
1. As over 75% of systemic iron is circulating, Oligoscan / skin data for iron will be an unreliable proxy for systemic levels – blood tests for serum iron studies (iron, transferrin, tsat% and ferritin) would be needed via your doctor or private lab testing.
Low manganese may also provide a hint for low iron, unless IV iron has recently been administered.
2. Calcium markers in skin data will be similarly unreliable – 99% of calcium is stored in skeletal tissue. This also makes serum calcium insensitive. As strontium and calcium can potentially substitute for each other in biological processes, using the “strontium” marker from the hair test as a proxy to indicate systemic calcium may be possible, but needs further study. Tremors and/or heart palpitations, especially in response to taurine or magnesium could indicate low calcium, also. Low phosphorus may indicate low calcium.
3. Copper and zinc appear to be over-estimated in some cases.
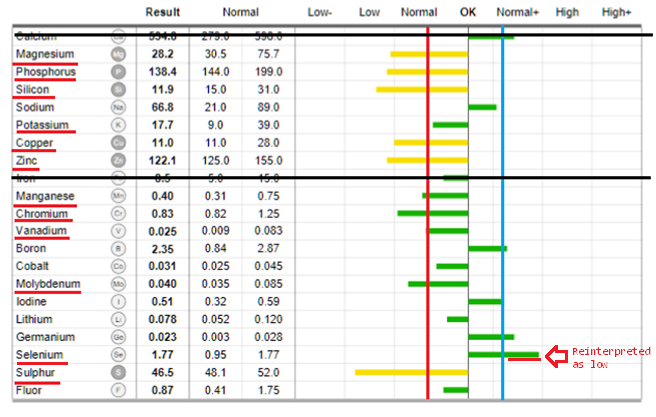
4. Due to an unusual quirk in methodology / reporting, highly elevated minerals need to be re-interpreted as highly deficient.
5. Highly elevated zinc in skin tissue may also indicate low protein / histidine intake and mask an actual zinc deficiency.
Oligoscan and CMA results are not known to be directly affected by the inflammatory cascade, meaning that these reports provide an actionable set of objective markers to use when choosing most mineral supplements to address deficiencies. (HTMA data can be referenced to help supplementation planning for rubidium and strontium, also inferring calcium).
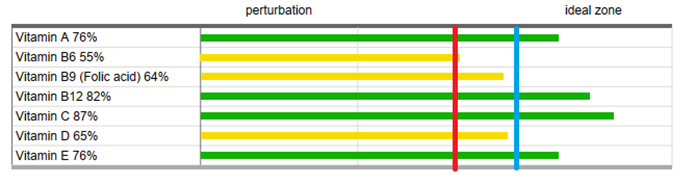
For more information about the effects of specific mineral deficiencies, see the “Rationale for protocol inclusions and general notes” section. The Oligoscan and SO/Check reports include a number of vitamin markers, which appear to track relatively well with other data. A good general target for these is to exceed 55%.
You can search for your nearest provider using our "Find an Oligoscan Practitioner" tool.
If you have a good (or bad) experience with an Oligoscan practitioner, please share details with our community Discord group in the #oligoscan-providers channel.
For Oligoscan, you can also find local practitioners here: https://www.theoligoscan.com/nearest-provider
or try using Google and run individual searches for each company / technology and your suburb (4 separate searches, rather than 1):
eg.
Oligoscan | Oligocheck | So-Check | ZellCheck <your suburb>
Broadly speaking, Oligocheck, So-Check and ZellCheck are more commonly found in and around Europe. Oligoscan is more commonly found in USA, Australia and UK.
Hair minerals (deprecated / limited use)
Research suggests that a Hair Toxin Mineral Analysis (HTMA) may provide an approximation of your functional mineral status, averaged over the period of follicle growth, sampled adjacent to the transporter alterations from inflammation – where circulating minerals can be sequestered inside various brain, liver and kidney cells and consequently low in other cells. It cannot accurately report on the intracellular levels or systemic levels, as sequestered minerals are not shown in this excretory data.
The results obtained from the HTMA data may be used to infer averaged intracellular mineral availability, downstream of any chronic inflammation, for the period of time in which the hair follicles grew, in a similar way to read HbA1C for glucose metabolism. This mechanism is largely relevant to the eleven elements transported by DMT-1 and ferroportin.
A list of vendors offering a compatible list of markers and reference ranges is provided below. Doctors Data and other compatible laboratories
| US | https://www.walkinlab.com/products/view/dd-hair-elements-profile-doctors-data (not available in NY/ NYC and other areas.) |
| AU | https://www.toxno.com.au/articles/heavy-metals/hair-tissue-mineral-analysis-hma-or-htma-in-australia/ (can manually add rubidium) |
| EU / UK | https://regeneruslabs.com/products/hair-toxic-essential-elements-1 |
| EU | https://www.biocoherence.eu/en/shop/htma/ (doesn't include rubidium) |
| EU | https://www.lifelinediag.eu/en/product/eha-standard-en/#products (doesn't include rubidium) |
| NZ | https://www.houseofhealth.co.nz/product/hair-toxic-mineral-analysis/ |
| PL | https://analizawlosa.com.pl/produkt/analiza-wlosa/ |
| UK / some EU | https://www.lauristonlabs.co.uk/product/hair-elements-doctors-data/ |
- Ignore any conflicting vendor-specific instructions.
- The hair needs to be clean, well-rinsed, dry, untreated and uncoloured. Unwashed hair may provide false (elevated) data for sodium and potassium, from dried sweat. Use gloves.
- Select suitable areas of sideburn, scalp and/or neck hair. If the hair is longer than 2.5cm / 1", first trim the sample area to this maximum length with clean stainless steel scissors. By using shorter hair, the report data relates to a more recent period of time.
- Cut the (remaining) hair to be sampled as close to the skin as possible. Do not use clippers or an electric razor – metal contamination from tungsten blades may occur. Collect at least two heaped tablespoons worth of hair, or approximately 250mg, or the sample may be rejected.
- Place the hair sample in the sample kit envelope provided, or in a clean, clearly labelled envelope or sachet. Whilst Trace Elements Inc says not to use resealable plastic bags as apparently hair “sweats” and the sample may be rejected, whereas Doctors Data supplies plastic bags in their kit.